
Abstract
Purpose
The purpose of this study was to investigate the effect of cataract surgery and pupil dilation on iris pattern recognition for personal authentication.
Methods
Prospective non-comparative cohort study. Images of 15 subjects were captured before (enrolment), and 5, 10, and 15 min after instillation of mydriatics before routine cataract surgery. After cataract surgery, images were captured 2 weeks thereafter. Enrolled and test images (after pupillary dilation and after cataract surgery) were segmented to extract the iris. This was then unwrapped onto a rectangular format for normalization and a novel method using the Discrete Cosine Transform was applied to encode the image into binary bits. The numerical difference between two iris codes (Hamming distance, HD) was calculated. The HD between identification and enrolment codes was used as a score and was compared with a confidence threshold for specific equipment, giving a match or non-match result. The Correct Recognition Rate (CRR) and Equal Error Rates (EERs) were calculated to analyse overall system performance.
Results
After cataract surgery, perfect identification and verification was achieved, with zero false acceptance rate, zero false rejection rate, and zero EER. After pupillary dilation, non-elastic deformation occurs and a CRR of 86.67% and EER of 9.33% were obtained.
Conclusions
Conventional circle-based localization methods are inadequate. Matching reliability decreases considerably with increase in pupillary dilation. Cataract surgery has no effect on iris pattern recognition, whereas pupil dilation may be used to defeat an iris-based authentication system.
Similar content being viewed by others


Introduction
Accurate automated personal authentication is a challenging problem and requires a robust solution. Biometrics-based authentication systems are security technologies, which use human characteristics for personal identification.1, 2 These are increasingly replacing conventional systems for access control, identity management, and financial transactions. Among the many physiological and behavioural characteristics, such as signatures, used to identify individuals, iris recognition is considered one of the most reliable forms of automatic human identity verification. Iris recognition systems use iris textures as unique identifiers. The human iris has an intricate structure with many minute characteristics such as furrows, freckles, crypts, and coronas.3, 4 These characteristics are unique as a result of the individual differences that arise during embryonic development. Apart from general textural appearance and colour, the detailed fine structure of an iris is not genetically determined, but develops by a random process. The iris patterns of the two eyes of an individual or those of identical twins are completely independent and uncorrelated.5 In addition, the iris is highly stable over a person's lifetime and lends itself to non-invasive identification, because it is externally visible. Iris-based biometric systems apply filters to iris images to extract information about its features.
Government and commercial organizations across the world are preparing to implement biometric-based authentication systems with fingerprint, face, and iris as the key components, with the latter considered essential for de-duplication of national and international scale databases. It is therefore important to understand the impact of common procedures and medications on iris recognition performance.
Cataract surgery is carried out regularly on thousands of people worldwide. More than 270 000 cataract procedures are performed every year in the United Kingdom alone.6 This may result in deformation of the iris during surgery and shift in its position away from the cornea because of replacement of the lens with a thinner implant. Pupils are dilated routinely before cataract surgery and in conditions such as uveitis, but mydriatics may also be acquired for self-administration. This detailed analysis of the effect of cataract surgery and pupil dilation on iris recognition is an attempt to gain a better understanding of the inherent shortcomings and strengths of any generic iris-based biometric system.
The aim of this study was to answer the research question: Is there an effect of cataract surgery or pupil dilation on iris pattern recognition?
Materials and methods
This prospective non-comparative cohort study was carried out at the Royal Eye Infirmary, Plymouth Hospitals NHS Trust, Plymouth, in collaboration with the University of Bath, United Kingdom. Ethical approval was obtained from the Cornwall and Plymouth Research Ethics Committee.
Patients attending for cataract surgery at the Royal Eye Infirmary were introduced to the study at their pre-operative assessment visit. Participants had iris images taken before and after instillation of dilating eye drops on the day of their cataract surgery. Short acting topical mydriatics (tropicamide 1% eye drops and phenylephrine 2.5% eye drops) were used for pupil dilation. Informed consent was taken in all cases.
Images were acquired from 15 subjects before and after the application of drops. Although the former ones were used to enrol the subjects, the latter ones were used to match. Patients were imaged ∼5, 10, and 15 min after administering the drops. Each patient was given a unique study number and so the study was completely anonymized. All images were localized, encrypted, and analysed by the researchers at the University of Bath.
A novel method for finding the light reflections from the iris was developed, and this proprietary system was used. This is a real security system in which original eye images from patients about to undergo cataract surgery were taken before the application of any medication or dilation drops. These images formed our enrolment set against which comparisons, for identification purposes, were carried out later. Post-operative images were captured 2 weeks after the operation at the routine follow-up appointment.
The original biometric data used for enrolment was converted into a template, which is a small archive called an iris code, consisting of optimized and filtered biometric acquired images (Figure 1a–d). When the user presents his biometric data again, another template is created. The verification template was compared with the enrolment template, and the mathematical difference between the iris codes was computed. This numerical difference between two iris codes is called the Hamming distance (HD). The HD between identification and enrolment codes was used as a score and was compared with a confidence threshold for specific equipment, giving a match or non-match result. The Correct Recognition Rate (CRR) and Equal Error Rates (EERs) were calculated to analyse overall system performance.

(a) Original image. (b) Localization. (c) Unwrapped iris image. (d) Binary iris code.
From the many images captured, three were chosen to form the test set for each subject. The images used for enrolment and matching were segmented to extract the iris. This was then unwrapped onto a rectangular format for normalization and a novel method using the discrete cosine transform (DCT) was applied to encode the image into binary bits.7 The feature extraction capabilities of the DCT are optimized on the two largest publicly available iris image data sets: 2156 images of 308 eyes from the CASIA (Chinese Academy of Sciences Institute of Automation) database and 2955 images of 150 eyes from the Bath database. On this data, we achieve 100% CRR with no registered false accepts or rejects. The exclusion criteria included corneal pathology, pre-existent iris pathology, intra-operative complications including damage to the iris, patients unable to keep still for the assessment (head tremor, dementia), inability to give informed consent, and patient refusal to participate in the study.
Statement of ethics
We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during this research.
Results
Cataract surgery
Promising results were obtained from pre and post-cataract surgery image comparisons. No visible change in iris structure was observed in post-operative eyes.
The iris structure essentially remains the same despite having undergone deformation during cataract surgery. Additional specular reflections occur in the pupil due to multiple reflections of the infrared light source from the surface of the intraocular lens implant. Such reflections could be a potential cause for concern for light-position-based pupil finding algorithms. The localization process used in this study finds the darkest region of significant area nearest to the image centre and is unaffected.
HD for matching and nearest non-matching were calculated for undilated irides after cataract surgery. Clear separation indicates perfect verification and identification with zero false acceptance rate, zero false rejection rate, and zero EER (Figure 2).

Hamming distances (HD) for matching and nearest non-matching for undilated irides after cataract surgery.
Pupil dilation
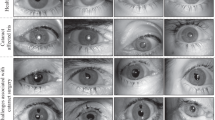
The primary concern with excessively dilated pupils is its non-elastic deformation and consequent loss in circularity (Figure 3).

Effect of dilation drops. (a) Undilated pupil. (b) Loss in circularity after dilation.
For irregular pupils, conventional circular localization deviates significantly from the real outline and the boundary should, thus, be modelled using an accurate shape description method. Matching and nearest non-matching HDs after pupil dilation were plotted. Crossovers in the plot indicate failure to correctly recognize all the cases; 6 failures occurred out of 45, giving a CRR of 86.67% and EER of 9.33% (Figure 4). The effect of increased dilation on the reliability of a match is illustrated in Figure 5. Images taken 5, 10, and 15 min after administering dilation drops were compared with non-dilated ones. With increase in time, and thus dilation, a significant decrease in separation is observed indicating a drastic fall in matching reliability. In addition, for highly dilated cases, as is true for the 15 min ones, the matching HDs become greater than the non-matching ones leading to failed identification and verification.

Matching and nearest non-matching hamming distances after pupil dilation.

Matching and nearest non-matching Hamming distance (HD) plots for an eye imaged 5, 10, and 15 min after administering dilation drops to it. Separation degrades with time, decreasing correct recognition rate.
Discussion
The effect of cataract surgery and pupil dilation on iris matching has been reported here. Initial results from pseudophakic eye comparisons suggest no degradation in performance for the patients enrolled. No visible change in iris structure is observed and successful localization was carried out despite an increase in number of specular reflections in the pupil. Perfect identification was achieved, indicating that the procedure may have little or no effect on an iris-based authentication system. However, to confirm these results, this study should be extended to a larger population.
A similar study by Roizenblatt et al8 in 2004 concluded that cataract surgery brings about a change in iris structure in such a way that iris pattern recognition may no longer be feasible or the probability of false rejected subjects is increased. They recommended re-enrolment of patients subjected to intraocular procedures in iris biometric systems so as to have a new template in the database.
Application of dilation drops, on the other hand, caused a dramatic change in pupil and iris structures within a short period of time. The pupil was seen to deform significantly and non-elastically within a few minutes of administering the drops. In many cases, it lost its circular shape and conventional circle-based localization methods proved inadequate in modelling its actual outline. A novel shape description method was used to handle these cases and more accurate normalized images were generated for feature extraction and matching. Despite accurate localization, system performance was poor with 6 failures to identify out of the total 45 images tested. The EER obtained was also very high at 9.33%. Matching reliability was shown to decrease with increase in pupil dilation.
It may thus be possible for an individual to defeat an iris-based identification system and get a false reject by the simple application of some dilation drops. Such failures need to be addressed before the deployment of projects such as the UK National ID Scheme, in which an individual may be able to exploit this to enrol at multiple places under different identities. In addition, errors in localization and matching are more likely to occur in systems based on the assumption of pupil circularity. Future work is required to draw statistically significant conclusions. However, it is clear that a thorough assessment is required to assess the consequences of variations in pupil size on iris matching. Although the effects of variation caused by illumination may differ from those caused by drugs, the assumption that the deformation of the iris is elastic as pupil size varies lacks supporting evidence and should also be studied.
In conclusion, images from patients acquired before and 2 weeks after cataract surgery showed no visible change in iris structure and automatic matching of these images produced correct identification in all cases. On the other hand, significant non-elastic deformation in iris structure was observed on administering dilation drops.
Despite accurate localization using a novel shape description method, highly deformed irides could fail to match correctly and the CRR obtained was only 86.67%.

References
Rakshit S, Monro DM . An evaluation of image sampling and compression for human iris recognition. IEEE Trans Inform Forensics and Security 2007; 2 (Issue 3), Part 2 605–612.
Jain AK, Ross A, Prabhakar S . An introduction to biometric recognition. IEEE Trans Circuits Syst Video Technol 2004; 14: 4–20.
Kardon R . The pupil. In: Kaufman PL, Alm A (eds). Adler's Physiology of the Eye. Clinical Application. Mosby Saunders: Missouri, 2002, pp 713–743.
Wolff E Last RJ (ed). Anatomy of the Eye and Orbit, 6th ed. HK Lewis & Co. Ltd: London, 1968.
Daugman J, Downing C . Epigenetic randomness, complexity, and singularity of human iris patterns. Proc R Soc Lond B Biol Sci 2001; 268: 1737–1740.
DoH. Hospital Activity and Episode Statistics. http://www.doh.gov.uk/public/stats1.htm.
Monro DM, Rakshit S, Zhang D . DCT-based iris recognition. IEEE Trans Pattern Anal Mach Intell 2007; 29 (4): 586–595.
Roizenblatt R, Schor P, Dante F, Roizenblatt J, Belfort Jr R . Iris recognition as a biometric method after cataract surgery. Biomed Eng Online 2004; 3: 2.
Acknowledgements
This work was sponsored by the Plymouth Hospitals NHS Trust and Smart Sensors Limited, Portishead, Bristol, United Kingdom.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
Professor DM Monro is a major shareholder and advisor to Smart Sensors Limited, which develops human iris recognition software. The remaining authors declare no conflict of interest.
Additional information
This paper was presented in part as a poster at the American Academy of Ophthalmology Annual Meeting, Atlanta, 2008, and as a free paper at UKISCRS annual meeting, Brighton, 2008
Rights and permissions
About this article
Cite this article
Dhir, L., Habib, N., Monro, D. et al. Effect of cataract surgery and pupil dilation on iris pattern recognition for personal authentication. Eye 24, 1006–1010 (2010). https://doi.org/10.1038/eye.2009.275
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2009.275
Keywords
This article is cited by
-
Phacoemulsification Cataract Surgery Affects the Discriminative Capacity of Iris Pattern Recognition
Scientific Reports (2019)
