
Abstract
Purpose
To evaluate anti-VEGF and photodynamic therapy (PDT) for juxtafoveal and extrafoveal choroidal neovascularization (CNV) due to age-related macular degeneration (ARMD), ocular histoplasmosis syndrome (OHS), and degenerative myopia.
Methods
A total of 10 eyes with juxtafoveal or extrafoveal choroidal neovascularization underwent intravitreal anti-VEGF therapy combined with verteporfin PDT (689 nm). Most treatments consisted of PDT every 12 weeks and either ranibizumab 0.5 mg every 4 weeks or bevacizumab 1.25 mg every 6 weeks, initiated concurrently. Retreatment criteria were persistent exudative signs on optical coherence tomography or fluorescein angiography.
Results
Presenting visual acuity (VA) ranged from 20/20 to 20/60 (mean log MAR±SD, 0.338±0.16 (20/44 equivalent)). After a mean follow-up of 17.5 months, it ranged from 20/15 to 20/40 (mean log MAR±SD, 0.150±0.14 (20/28 equivalent); P=0.027, paired t-test). Six eyes improved by ⩾2 lines and four remained within 2 lines of initial VA. Non-ARMD eyes required much fewer treatments than ARMD eyes. All five non-ARMD eyes and three of five ARMD eyes showed no CNV activity at least 5 months after last treatment.
Conclusions
Anti-VEGF therapy and PDT can preserve good visual function and may be suited to some cases of nonfoveal CNV. ARMD eyes require longer courses of treatment than non-ARMD eyes.
Similar content being viewed by others


Introduction
Macular laser photocoagulation therapy is an accepted treatment for selected juxtafoveal and extrafoveal choroidal neovascular membranes (CNVM) due to age-related macular degeneration (ARMD) and ocular histoplasmosis syndrome (OHS).1, 2, 3, 4 It has also been used in degenerative myopia with extrafoveal CNV, although its benefit has been debated.5 The function of anti-VEGF and photodynamic therapy (PDT) as a potential alternative to laser treatment in such cases was evaluated to determine if improved outcomes might be expected with these treatments. Although this approach has been reported for subfoveal lesions,6, 7, 8 few if any reports exist for juxtafoveal or extrafoveal lesions.
Materials and methods
An IRB-approved, retrospective chart review was performed at the Medical College of Wisconsin of 10 eyes of 10 consecutive patients with juxtafoveal or extrafoveal CNV that underwent treatment with intravitreal anti-VEGF agents combined with verteporfin full-fluence PDT (verteporfin dose 6 mg/m2; laser parameters 689 nm, 600 mW/cm2, 83 s), between July 2004 and July 2007. Five eyes had ARMD, three had OHS, and two had degenerative myopia. The CNVM lesions at presentation were sufficiently well demarcated to be classified as extrafoveal in four eyes (two ARMD and two OHS eyes) and juxtafoveal in six eyes (three ARMD, one OHS, and two degenerative myopia eyes). All patients presented with recent onset visual symptoms. Verteporfin PDT (Visudyne; Novartis Inc., East Hanover, NJ, USA) was administered according to the manufacturer's recommendation. Laser spot diameter was the greatest linear dimension of the lesion plus 1.0 mm, such that it extended at least 0.5 mm beyond the lesion margins. For juxtafoveal lesions, if possible, the edge of the spot avoided the foveal centre without reducing CNV exposure. Three ARMD eyes underwent an initial regimen of PDT, followed by anti-VEGF monotherapy (ranibizumab (Lucentis; Genentech Inc., South San Francisco, CA, USA) 0.5 mg every 4 weeks or bevacizumab (Avastin; Genentech Inc.) 1.25 mg every 6 weeks), initiated between 2 months and 2 years later. Intervals between PDT and anti-VEGF treatment varied because of unavailability of the latter for the earliest cases. Two ARMD eyes had PDT every 12 weeks and either ranibizumab 0.5 mg every 4 weeks or bevacizumab 1.25 mg every 6 weeks, initiated concurrently, based upon availability of the particular anti-VEGF agent. The five non-ARMD eyes were treated by PDT given at intervals of 10–12 weeks and intravitreal bevacizumab 1.25 mg given at intervals of 4–6 weeks, initiated concurrently. Retreatment criteria were persistent oedema or subretinal fluid on optical coherence tomography (OCT) and/or leakage on fluorescein angiography (FA).
Results
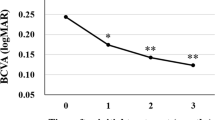
Comparison of presenting and final visual acuity (logMAR) by patient and corresponding diagnosis is indicated in Figure 1. Due to similarity in visual outcomes among the three diagnosis groups, comparison between presenting and final visual acuity (VA) was performed on the entire group combined. Presenting best-corrected VA ranged from 20/20 to 20/60 (mean log MAR±SD, 0.338±0.16 (20/44 equivalent)). After a mean follow-up of 17.5 months, final VA ranged from 20/15 to 20/40 (mean log MAR±SD, 0.150±0.14 (20/28 equivalent); P=0.027, paired t-test). Of the 10 eyes, 6 improved by ⩾2 lines and 4 remained within 2 lines of initial VA. Non-ARMD eyes with combined bevacizumab/PDT required means of 2.6 injections (range 1–7) and 1.4 PDT sessions (range 1–2). ARMD eyes required means of 5.2 injections (range 1–10) and 2.0 PDT sessions (range 1–4). At final follow-up, all five non-ARMD eyes and three of five ARMD eyes showed no oedema or subretinal fluid on OCT and/or no leakage on FA at a minimum of 5 months after last treatment. A representative case is shown in Figure 2.

Comparison of presenting and final visual acuity (logMAR) by patient and corresponding diagnosis. Lines connect paired data for each patient. Lines are shaded differently for each diagnosis.

(a) Preoperative fluorescein angiogram in patient with degenerative myopia and juxtafoveal CNVM. VA was 20/20. (b) Follow-up fluorescein angiogram obtained 4 months after termination of a concurrent course of full-fluence verteporfin PDT (one session) and bevacizumab (two injections). VA was 20/25.
Conclusions
Our visual results were better than those reported by the Macular Photocoagulation Study (MPS) for extrafoveal1 and juxtafoveal CNV2, 3 in eyes that received laser photocoagulation, and better than those of another study in which nonfoveal CNV had been successfully obliterated with laser4 (Table 1). However, the MPS data are provided as a perspective and are not directly comparable to our results because of marked differences in methodology and sample size between the studies. Larger studies are needed to demonstrate the validity of our approach.
Because anti-VEGF therapy in ARMD has proved beneficial with subfoveal CNV,6 it might be expected that extrafoveal or juxtafoveal lesions might have similarly favourable outcomes, as suggested by this series. Because of the concern of progression of CNV to frank subfoveal involvement, a maximally aggressive approach with combination therapy, including PDT, was chosen and good outcomes were achieved. Nevertheless, it is possible that anti-VEGF therapy without PDT might achieve similarly good results in nonfoveal CNV, in light of its superiority to PDT in subfoveal CNV due to ARMD.6 For this reason, we do not recommend PDT alone for either foveal or nonfoveal ARMD cases. Notably, ARMD eyes required longer courses of treatment than non-ARMD eyes.
Our study suggests that physicians may be justified in choosing anti-VEGF therapy, possibly combined with PDT, as an alternative to MPS-style laser photocoagulation for at least some cases of nonfoveal CNV. Our current approach is to more favourably consider a non-laser approach, the closer the proximity of CNV to the fovea.
References
Macular Photocoagulation Study Group. Argon laser photocoagulation for neovascular maculopathy. Three-year results from randomized clinical trials. Arch Ophthalmol 1986; 104: 694–701.
Macular Photocoagulation Study Group. Krypton laser photocoagulation for neovascular lesions of age-related macular degeneration. Results of a randomized clinical trial. Arch Ophthalmol 1990; 108: 816–824.
Macular Photocoagulation Study Group. Krypton laser photocoagulation for neovascular lesions of ocular histoplasmosis. Results of a randomized clinical trial. Arch Ophthalmol 1987; 105: 1499–1507.
Han DP, Folk JC, Bratton AR . Visual loss after successful photocoagulation of choroidal neovascularization. Ophthalmology 1988; 95: 1380–1384.
Virgili G, Menchini F . Laser photocoagulation for choroidal neovascularisation in pathologic myopia. Cochrane Database Syst Rev 2005; (4): CD004765 (web-access only).
Kaiser PK, Brown DM, Zhang K, Hudson HL, Holz FG, Shapiro H et al. Ranibizumab for predominantly classic neovascular age-related macular degeneration: subgroup analysis of first-year ANCHOR results. Am J Ophthalmol 2007; 144: 850–857.
Lazic R, Gabric N, Dekaris I, Gavric M, Bosnar D . Photodynamic therapy combined with intravitreal bevacizumab (Avastin) in treatment of choroidal neovascularization secondary to age-related macular degeneration. Collegium Antropologicum 2007; 31 (Suppl 1): 71–75.
Heier JS, Boyer DS, Ciulla TA, Ferrone PJ, Jumper JM, Gentile RC, et al., FOCUS Study Group. Ranibizumab combined with verteporfin photodynamic therapy in neovascular age-related macular degeneration: year 1 results of the FOCUS Study. Arch Ophthalmol 2006; 124: 1532–1542.
Acknowledgements
The institution with which the authors DP Han, WJ Wirostko, DV Weinberg, and JE Kim are affiliated (Medical College of Wisconsin, Milwaukee, WI, USA) receives research funds to conduct clinical trials from the following entities: Allergan Inc., Genentech Inc., and Novartis Inc.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was supported in part by an unrestricted grant from Research to Prevent Blindness Inc., New York, NY, USA.
Conflict of interest
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Han, D., McAllister, J., Weinberg, D. et al. Combined intravitreal anti-VEGF and verteporfin photodynamic therapy for juxtafoveal and extrafoveal choroidal neovascularization as an alternative to laser photocoagulation. Eye 24, 713–716 (2010). https://doi.org/10.1038/eye.2009.122
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2009.122
Keywords
This article is cited by
-
Eye disease drug as a potential cure for COVID-19: one foot-in-the-door
Eye (2023)
-
Stages, pathogenesis, clinical management and advancements in therapies of age-related macular degeneration
International Ophthalmology (2023)
-
Stellungnahme der Deutschen Ophthalmologischen Gesellschaft, der Retinologischen Gesellschaft und des Berufsverbandes der Augenärzte Deutschlands zur Therapie der chorioidalen Neovaskularisation bei Myopie
Der Ophthalmologe (2014)
-
Choroidal neovascularization following laser in situ keratomileusis for high myopia: a case series
International Ophthalmology (2013)
