
Abstract
Orphan nuclear receptor estrogen-related receptor γ (ERRγ) regulates cell growth and tumorigenesis in various cancers. However, the clinical relevance of ERRγ to hepatocellular carcinoma (HCC) remains unclear. Here we examined the clinical significance of ERRγ in HCC and its potential as a therapeutic target. ERRγ levels in tissues from completely resected specimens from 190 HCC patients were examined immunohistochemically and their association with clinical stage and pathological grade was analyzed. Small interfering RNA (siRNA)-mediated knockdown of ERRγ (siRNA-ERRγ) or an ERRγ inverse agonist, GSK5182, were also used to examine the effects of ERRγ inhibition on the proliferation and growth of a human hepatoma cell line, PLC/PRF/5. Immunohistochemical analysis revealed that tumor tissues showed higher levels of ERRγ-positivity than adjacent non-tumor lesions. Tumors showing high levels of ERRγ immunoreactivity also had advanced tumor node metastasis (TNM) and Barcelona Clinic Liver Cancer stages and a higher Edmondson–Steiner grade. In addition, high-level expression of ERRγ in tumors of advanced TNM stage correlated with poorer overall survival. Treatment of PLC/PRF/5 cells with siRNA-ERRγ or GSK5182 inhibited proliferation through G1 arrest, increased expression of p21 and p27 and decreased expression of phosphorylated retinoblastoma protein. GSK5182-induced reactive oxygen species also suppressed the proliferation of PLC/PRF/5 cells. The present study showed that ERRγ expression is clinically significant in HCC; therefore, it can be considered a biomarker for HCC diagnosis. Moreover, the results provide a rationale for the use of ERRγ inhibitors such as GSK5182 as potential therapeutic agents.
Similar content being viewed by others


Introduction
Hepatocellular carcinoma (HCC) is the sixth most common and leading cause of cancer-related death worldwide.1 Curative treatment is effective only if the cancer is diagnosed at an early stage; however, recurrence rates are high and long-term survival is poor.2 Therefore, it is imperative to identify markers that can improve early diagnostic accuracy and predict disease prognosis; such markers would enable clinicians to decide the most appropriate course of treatment. Increased understanding of the signaling pathways underpinning HCC development and progression has stimulated interest in the identification of molecular biomarkers that may predict the prognosis of patients with HCC and/or be developed as potential therapeutic targets.3
Estrogen receptor (ER)-related receptors (ERRs; ERRα, ERRβ, and ERRγ) belong to the NR3B group of nuclear receptors and are closely related to ERs, sharing highly homologous DNA-binding domains; however, they are constitutively active and do not bind to natural estrogen.4, 5 Among these receptors, ERRγ is expressed in tissues associated with high metabolic demand, including heart, skeletal muscle and brown adipose tissue.6 Accumulating evidence indicates that ERRγ is involved in controlling mitochondrial biogenesis and cellular energy homeostasis and that it has a pivotal role in metabolic deregulation in various tissues.7 Besides its role in metabolic disease, recent studies report the clinical significance of ERRγ in estrogen-dependent cancers such as those of the breast and endometrium. For example, ERRγ is overexpressed in breast cancer and correlates with lymph node-positive status, indicating that ERRγ has an important role in promoting the growth and metastasis of breast cancer.8, 9 ERRγ is upregulated during the acquisition of tamoxifen resistance, suggesting that it may be a predictive marker for a poor therapeutic response by breast cancer.8, 9 Similarly, ERRγ is upregulated in endometrial cancer, and its expression increases with clinical stage, depth of myometrial invasion and an increase in the number of metastatic lymph nodes.10 Moreover, ERRγ mediates estrogen-induced proliferation of endometrial cancer cells.11 However, no studies have examined the clinical relevance of ERRγ to HCC or its potential as a therapeutic target.
Aberrant expression of cell cycle protein kinases is a hallmark of human malignancy; therefore, a considerable number of small molecules targeting cell cycle regulatory proteins have been studied as candidate treatments for attenuating the proliferation of cancer cells.12 Cyclin-dependent kinase inhibitors such as p21WAF1 and p27Kip1 are negative regulators of the cell cycle check point and essential mediators of cell cycle arrest.13, 14 Therefore, increasing the expression of p21 or p27 has been attempted to induce growth arrest in cancer cells.15 In this context, expression of the ERR subfamily in tumor tissues has focused attention on their role in cancer cell cycle progression in conjunction with regulation of cyclin-dependent kinase inhibitor.16 Upregulation of ERRα in breast and colon cancer has a role in cell cycle progression,17, 18 whereas downregulating ERRβ affects the cell cycle and tumor progression in prostate cancer.19, 20 Accordingly, small molecules that enable the selective inhibition of ERRα or activate ERRβ induce cell cycle arrest and inhibit cell proliferation. For example, a synthetic ERRα inverse agonist, XCT790, downregulates cell proliferation and inhibits G1- to S-phase transition by upregulating p21.21 On the other hand, the ERRβ agonist, DY131, inhibits the ERRβ-induced growth of prostate cancer cells, which is attributed to p21 induction.20 However, despite the increasing attention focused on the relevance of ERRγ in cancer, no studies have examined whether the ERRγ inverse agonist, GSK5182, effectively modulates cell cycle progression.
Therefore, the present study examined the expression of ERRγ in HCC and compared it with that in adjacent non-tumor lesions. We also investigated the correlation between ERRγ expression and clinicopathological stage. Furthermore, we determined whether GSK5182 inhibits cell cycle progression and HCC cell proliferation.
Materials and methods
Patients and specimens
Samples of HCC and adjacent non-tumor tissues were obtained from 190 HCC patients who underwent surgical resection at Keimyung University Dongsan Hospital in Daegu, Korea from 2001 to 2011. Patients who had received preoperative anticancer treatment, such as transarterial chemoembolization or local ablation therapy, were excluded. Tumor staging was determined according to the American Joint Committee on Cancer (AJCC 2010, Seventh Edition) tumor node metastasis (TNM) staging system22 and the Barcelona Clinic Liver Cancer (BCLC) staging system for HCC.23 Tumor differentiation was defined according to the Edmondson grading system.
Immunohistochemical staining and scoring
A tissue microarray containing tissue from HCC (n=190) and adjacent non-tumor tissues (n=187) was constructed as previously described,24 Immunohistochemical analysis was performed on 5-μm thick tissue sections using an anti-ERRγ antibody (1:1600) (R&D Systems, Minneapolis, MN, USA). ERRγ expression was evaluated using the proportion score, defined as the estimated fraction of positively stained tumor cells (0, none; 1+, <10%; 2+, 10–25%; 3+, >25%). Scores of 2 and 3 were considered as high-level expression. All slides were evaluated independently three times by a senior pathologist blinded to the patients’ clinical information and follow-up data.
Cell culture
The human hepatoma cell line PLC/PRF/5 was purchased from ATCC (American Type Culture Collection, Manassas, VA, USA) and grown at 37 °C/5% CO2 in Roswell Park Memorial Institute 1640 medium (Life Technologies, Carlsbad, CA, USA) supplemented with 10% fetal bovine serum (Hyclone, Logan, UT, USA). Cells were trypsinized and then stained with 0.2% trypan blue solution (Sigma, St Louis, MO, USA) and counted using a hemocytometer (Superior, Marienfeld, Germany).
Western blotting analysis
Cells were washed three times with phosphate-buffered saline (PBS) and lysed with lysis buffer containing 20 mM Tris-HCl (pH 7.4), 5 mM EDTA (pH 8.0), 10 mM Na4P2O7, 100 mM NaF, 2 mM Na3VO4, 1% NP-40 and protease and phosphatase inhibitors. The protein concentration in the whole-cell lysate was determined using the BCA assay (Thermo Fisher Scientific, Waltham, MA, USA). Denatured protein (25 μg) was separated on a 10% polyacrylamide gel and transferred to a polyvinylidene difluoride membrane. The membrane was blocked with 5% skim milk in Tris-buffered saline (TBS) containing 0.1% Tween 20 (TBST) and incubated with each primary antibody overnight at 4 °C. The primary antibody against ERRγ was purchased from R&D Systems; antibodies against p21 and p27 were purchased from BD Pharmingen (Lexington, KY, USA); the antibody against phosphorylated retinoblastoma protein (p-pRb) was purchased from Cell Signaling Technology (Beverly, MA, USA); and the antibodies against total-pRb and β-actin were purchased from Santa Cruz Biotechnology (Santa Cruz, CA, USA). Membranes were washed three times with TBST and incubated with horseradish peroxidase-conjugated mouse (Santa Cruz) or rabbit (Cell Signaling Technology) secondary antibodies. ECL reagent (Bionote, Hwaseong-si, Korea) was used to detect horseradish peroxidase, and images were analyzed using an ImageQuant LAS4000 mini (GE healthcare Life Science, Piscataway, NJ, USA).
Small interfering RNA (siRNA) transfection
Cells were transfected with 50 nM of scrambled siRNA or siRNA-ERRγ using lipofectamine LTX (Invitrogen, Carlsbad, CA, USA), according to the manufacturer’s protocol. The following siRNA sequence was used for ERRγ silencing: sense: 5′-CUGAUAGGUUUCCUCUACU-3′, and antisense: 5′-AGUAGAGGAAACCUAUCAG-3′.
Flow cytometric analysis
The cell cycle was analyzed by staining cells with propidium iodide. Briefly, cells were trypsinized, washed twice with PBS and fixed with absolute EtOH overnight at −20 °C. The fixed cells were then washed twice with PBS and stained with 0.5 μg ml−1 propidium iodide solution. The cell cycle was examined using an Accuri C6 flow cytometer (BD Biosciences, San Jose, CA, USA) operating at 585/40 nm with a fl2/A filter. After gating to eliminate debris and doublets using side scatter and forward scatter, 104 cells were collected and analyzed per sample. Analysis was performed with the BD Accuri C6 software (BD Biosciences).
DCF-DA staining
The generation of reactive oxygen species (ROS) by ERRγ inhibition was analyzed by chloromethyl-2′,7′-dichlorodihydrofluorescein diacetate (CM-H 2 DCF-DA) staining. Briefly, 20 μM of DCF-DA was added to cells plated on a coverslip and incubated for 30 min. Cells were then washed three times with PBS and fixed in 4% paraformaldehyde for 20 min at room temperature. Fixed cells were then washed three times with PBS, and images were captured using an Olympus IX81 fluorescence microscope (Olympus Corp., Tokyo, Japan).
Luciferase reporter assay
PLC/PRF/5 cells were used for transient transfection assays. Cells were transfected with a luciferase reporter gene plasmid using Mirus TransIT-LT1 transfection reagent (Mirus Bio LLC, Madison, WI, USA), according to the manufacturer’s protocol. Cells were transfected for 1 day and then treated with GSK5182 for 2 days. Luciferase activity was then measured using a luminometer (Berthold Detection Systems, Pforzheim, Germany). β-Galactosidase activity was used for normalization. The plasmid encoding stf4-Luc was kindly donated by Heung-Sik Choi (Chonnam National University, Gwangju, Korea).25
Chemicals
GSK5182 was synthesized as previously described.26 GSK5182 was obtained as an HCl salt, dissolved in dimethyl sulfoxide and used at the indicated concentrations for in vitro experiments. N-acetylcysteine was purchased from Sigma.
Relative quantification analysis
Relative protein levels and fluorescence signals for DCA-DA were analyzed using the Image J software (US National Institutes of Health, Bethesda, MD, USA).
Ethics statement
The study was approved by the institutional review board (IRB) of Keimyung University Dongsan Hospital (IRB no: 11-256). Written informed consent was obtained from each patient.
Statistical analyses
Statistical analysis was performed using a two-tailed Student’s t-test. Data are expressed as the mean±s.e.m. Clinical data management and statistical analyses were performed using the SPSS software (version 18.0; SPSS, Inc., Chicago, IL, USA). The association between protein levels and categorical variables was evaluated using Pearson’s χ2 test. Overall survival was estimated using the Kaplan–Meier method. P<0.05 was considered statistically significant.
Results
ERRγ levels in HCC and their association with clinical stage and pathological grade
We first measured the level of ERRγ in tumors obtained from 190 HCC patients after liver resection and compared it with that in adjacent non-tumor tissues obtained from the same patients. The baseline characteristics of the 190 patients24 are described in Supplementary Table S1. The immunoreactivity of ERRγ in non-tumor and tumor tissues was scored from 0 to 3+ according to the intensity of staining. Immunohistochemical analysis revealed that 183 non-tumor lesions stained negative, with only four cases staining positive. By contrast, only 55 tumor lesions stained negative, whereas 135 cases stained positive. Notably, high levels of ERRγ (defined as an immunoreactivity score of 2+ or 3+) were observed only in tumor tissues; all non-tumor tissues expressed low levels of ERRγ (immunoreactivity score of 0 or 1+) (Figure 1a).

Immunohistochemical (IHC) analysis of ERRγ expression in surgically resected human HCC tumors and corresponding adjacent non-tumor tissues and its clinicopathological associations. (a) Representative images showing IHC staining of ERRγ in tumor (n=190) and adjacent non-tumor (n=187) lesions (original magnification: × 400). The degree of IHC reactivity was scored from 0 to 3 according to the proportion of positively stained tumor cells: 0, none; 1+, <10%; 2+, 10–25%; 3+, >25%. Three cases of non-tumor tissues were missed. (b–d) Proportion of tumors with early and advanced TNM (b) and BCLC (c) stages and with low and high Edmondson grades (d) according to ERRγ expression.
We next examined whether this upregulation correlated with tumor stage and grade. The results showed that a higher percentage of patients with low-level ERRγ expression had tumors at TNM stage I and II, whereas a higher percentage of patients with high-level ERRγ expression had tumors at TNM stage III (P=0.005; Figure 1b). Furthermore, a significantly higher percentage of patients with low-level ERRγ expression had early-stage BCLC (0 and A) and showed a lower Edmondson–Steiner grade (I and II) (Figures 1c and d; P=0.049 and P=0.026, respectively). Taken together, these results suggest that the ERRγ level was markedly higher in HCC than in adjacent non-tumor liver tissues and that higher ERRγ immunoreactivity correlated with more advanced clinical stage and higher HCC pathological grade.
Relationship between ERRγ level and overall survival
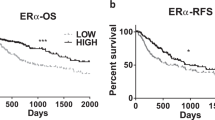
Next we examined the relationship between ERRγ immunoreactivity and overall survival. The median follow-up period was 31.4±1.41 (range, 0.2–136.0) months. Although there was no correlation between ERRγ level and survival at early TNM stages (stages I and II) (P=0.200, Figure 2a), high-level ERRγ expression and an advanced TNM stage (stage III) correlated with shorter overall survival (median survival, 47.1 months vs 99.9 months for high and low level of ERRγ immunoreactivity in tumors, respectively; P=0.012; Figure 2b).

Kaplan–Meier analysis of the survival of HCC patients according to ERRγ immunoreactivity. (a) Early TNM stages (I and II). (b) advanced TNM stage (III). Low-level ERRγ expression was defined as a score of 0 or 1+; high-level ERRγ expression was defined as a score of 2+ or 3+.
Knocking down ERRγ inhibits HCC cell proliferation and induces G1-phase arrest
Because ERRγ was upregulated in human HCC tissue, we next explored whether downregulating ERRγ inhibits HCC cell proliferation and growth. As shown in Figure 3a, siRNA-mediated knockdown of ERRγ inhibited PLC/PRF/5 cell proliferation. We then examined whether knocking down ERRγ inhibits cell growth by measuring the expression of cell cycle regulatory proteins and by fluorescence-activated cell sorting analysis of cell cycle progression. Immunoblot analysis showed that siRNA-ERRγ increased the expression of the cyclin-dependent kinase inhibitors, p21 and p27, but reduced p-pRb levels (Figure 3b). Flow cytometric analysis revealed that siRNA-ERRγ caused a significant increase in the percentage of cells in G1 phase (55.2% in transfected cells vs 38.2% in control cells), with a concomitant decrease in the percentage of cells in S phase (17.7% in transfected cells vs 26.3% in control cells) (Figure 3c).

Knocking down ERRγ inhibits HCC cell proliferation and induces G1 phase arrest. (a) Growth curve analysis of PLC/PRF/5 cells after transfection with scrambled or siRNA-ERRγ. A white circle denotes scrambled siRNA and a black circle denotes ERRγ-siRNA. (b) Representative western blotting showing the effect of siRNA-ERRγ on the levels of cell cycle regulatory proteins. PLC/PRF/5 cells were transfected with scrambled siRNA or siRNA-ERRγ for 2 days. ERRγ, p21 and p27 levels were normalized to β-actin and phospho-pRb levels were normalized to total-pRb levels. Data are expressed as the mean±s.e.m. of three independent measurements. **P<0.01, and ***P<0.001 vs scrambled control. (c) Representative flow cytometric data derived from the analysis of cell cycle progression in PLC/PRF/5 cells. Quiescent cells were transfected with scrambled siRNA or siRNA-ERRγ. Propidium iodide-stained cells were separated by flow cytometry.
The ERRγ inverse agonist, GSK5182, attenuates HCC cell proliferation
Next we used the inverse agonist, GSK5182, to examine whether pharmacological inhibition of ERRγ activity has an antitumor effect. HCC cells were transiently transfected with the Stf4 luciferase reporter plasmid containing the ERRγ response element and then exposed to various doses of GSK5182.25 A luciferase reporter assay revealed that GSK5182 significantly attenuated ERRγ activity in a dose-dependent manner (Figure 4a). Consistent with the results from experiments involving endogenous knockdown of ERRγ, we found that treatment with GSK5182 led to a significant and dose-dependent reduction in the number of proliferating PLC/PRF/5 cells (Figure 4b). GSK5182 also caused a dose-dependent increase in the expression of p21 and p27 while at the same time reducing the level of p-pRb (Figure 4c). The results obtained from flow cytometry revealed that GSK5182 induced cell cycle arrest at G1 phase, which in turn induced a corresponding dose-dependent reduction in the percentage of cells in S phase (Figure 4d). Taken together, these data indicate that the antitumor effect of GSK5182 in HCC cells is mediated by the induction of cell cycle arrest at the G1/S checkpoint.

An ERRγ inverse agonist, GSK5182, inhibits HCC cell proliferation. (a) Luciferase reporter assays were used to examine the effect of GSK5182, which inhibits ERRγ activity. PLC/PRF/5 cells were transfected with the luciferase reporter construct stf4-Luc in the presence of the indicated doses of GSK5182. Relative promoter activity was determined after 2 days. (b) Growth curve analysis of HCC cells after treatment with DMSO or with the indicated doses of GSK5182. A white circle denotes the vehicle; a gray circle denotes 10 μM GSK5182; a black circle denotes 20 μM GSK5182. (c) Representative western blotting showing the effect of GSK5182 on the expression of cell cycle regulatory proteins. PLC/PRF/5 cells were treated with DMSO or with the indicated doses of GSK5182 for 24 h. ERRγ, p21 and p27 levels were normalized to β-actin and phospho-pRb levels were normalized to total-pRb levels. Data are expressed as the mean±s.e.m. of three independent measurements. *P<0.05, **P<0.01 and ***P<0.001 vs control. (d) Representative flow cytometric data derived from analysis of cell cycle progression in PLC/PRF/5 cells. Quiescent cells were treated with DMSO or with the indicated doses of GSK5182. Propidium iodide-stained cells were separated by flow cytometry.
The antitumor effects of GSK5182 are also mediated by ROS
To examine the factors that contribute to GSK5182-induced cell cycle arrest, we next examined whether cellular GSK5182 increased ROS levels. As shown in Figure 5a, GSK5182 increased the level of cellular ROS (as measured by DCF-DA staining) in a dose-dependent manner (Figure 5a). Moreover, pretreatment with the antioxidant, N-acetylcysteine, attenuated GSK5182-induced suppression of HCC cell proliferation (Figure 5b), indicating that the antitumor effects of GSK5182 are, at least in part, mediated via ROS generation.

GSK5182 induces ROS generation and NAC attenuates GSK5182-induced suppression of HCC cell proliferation. (a) Representative DCF-DA fluorescence images showing the effect of GSK5182 on ROS generation in PLC/PRF/5 cells. Cells were treated with DMSO or with the indicated doses of GSK5182 for 24 h and then stained with 2’,7’-dichlorodihydrofluorescein diacetate (DCF-DA). (Original magnification: × 200). (b) Effect of NAC on GSK5182-induced inhibition of HCC cell proliferation. PLC/PRF/5 cells were pretreated (or not) with 8 mM NAC for 1 h, followed by incubation with the indicated doses of GSK5182 for 24 h. Data are expressed as the mean±s.e.m. of three independent measurements. *P<0.05, **P<0.01 and ***P<0.001 vs indicated group.
Discussion
Here we showed that the level of ERRγ-positivity in HCC tissues was markedly higher than that in adjacent non-tumor liver tissues and that tumors expressing high levels of ERRγ were of more advanced clinical stage and pathological grade. Furthermore, we found that inhibiting ERRγ had an apparent therapeutic effect on HCC cells by inducing cell cycle arrest.
Previous studies have noted inconsistent expression of ERRγ in various tumor tissues and have attempted to examine its role in tumor growth.8, 9, 19 Overexpression of ERRγ is frequently observed in endometrial and breast cancers, whereas ERRγ is downregulated in many prostate cancer cell lines; this suggests that ERRγ has different roles depending on the tumor type.19 The present study showed that ERRγ was upregulated in human HCC tissue but was rarely expressed in adjacent normal liver tissue. The clinical significance of high ERRγ expression in patients is highlighted by the results showing that tumors expressing high levels of ERRγ were also of advanced TNM and BCLC stage and had a higher Edmondson–Steiner grade. We also showed that high levels of ERRγ expression in patients with TNM stage III tumors were associated with worse overall survival, supporting the role of ERRγ as a potential prognostic marker for advanced HCC. However, because the study cohort included patients who had undergone curative tumor resection, none of the patients had TNM stage IV tumors. Therefore, to fully elucidate the clinical significance of ERRγ at all stages of HCC, further studies should examine the association between ERRγ and clinical features in a cohort that includes patients with inoperable tumors. Considering that early detection of small HCC is an important prognostic factor for curative resection, it is also important to identify biomarkers that increase diagnostic accuracy. Although the cohort in the present study was not selected to estimate diagnostic accuracy, the tumor-specific expression of ERRγ suggests that it is of diagnostic value. Indeed, the sensitivity, specificity and positive and negative predictive value of ERRγ for HCC were 71, 98, 97 and 77%, respectively. These results are comparable with those obtained for other proven HCC markers.27, 28, 29 Taken together, the results presented herein suggest that ERRγ might be a novel prognostic marker of an unfavorable clinical outcome and may have utility as a diagnostic biomolecule that can improve diagnostic accuracy for HCC when combined with other tissue markers.
The association between ERRγ expression in HCC tissue and clinical significance prompted us to investigate the possibility that ERRγ may be a potential therapeutic target for HCC. We examined this possibility using siRNA-mediated knockdown of ERRγ and a 4-hydroxy tamoxifen analog, GSK5182, which is a selective inverse agonist of ERRγ that does not interact with other nuclear receptors, including ERRα or ERα, owing to additional noncovalent interactions with Y326 and N346 within the active site of ERRγ.26, 30 Indeed, ERRγ knockdown and GSK5182 treatment reduced HCC cell proliferation by inducing cell cycle arrest. The results showing that ERRγ knockdown and GSK5182 treatment upregulated p21 and p27 protein levels suggest that the antitumor effects occur via p21- and p27-mediated blockade of G1–S transition. Our data are consistent with a previous study showing that overexpression of ERRγ induced S-phase cell cycle progression in Hela cells through the induction of Plk2 expression.31 Mounting evidence shows that p21-mediated oxidative stress induces p53-dependent and p53-independnt cell cycle arrest.14 In line with this, our own results showed that GSK5182 induces ROS generation and that antioxidant treatment prevents the GSK5182-induced reduction of HCC cell proliferation, indicating that GSK5182 mediated its effects via ROS generation.
To the best of our knowledge, the present study is the first to show the clinical significance of ERRγ in HCC. The evidence presented herein strongly suggests that further studies are necessary to fully elucidate whether ERRγ is a novel biomarker for the diagnosis and prognosis of HCC. Furthermore, the finding that GSK5182 inhibits of HCC growth and proliferation raises the possibility that chemical inhibitors of ERRγ may be a potential resource for HCC treatment.
References
Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM . Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 2010; 127: 2893–2917.
Bruix J, Sherman M . Management of hepatocellular carcinoma: an update. Hepatology 2011; 53: 1020–1022.
Llovet JM, Bruix J . Molecular targeted therapies in hepatocellular carcinoma. Hepatology 2008; 48: 1312–1327.
Razzaque MA, Masuda N, Maeda Y, Endo Y, Tsukamoto T, Osumi T . Estrogen receptor-related receptor gamma has an exceptionally broad specificity of DNA sequence recognition. Gene 2004; 340: 275–282.
Giguere V . To ERR in the estrogen pathway. Trends Endocrinol Metab 2002; 13: 220–225.
Bookout AL, Jeong Y, Downes M, Yu RT, Evans RM, Mangelsdorf DJ . Anatomical profiling of nuclear receptor expression reveals a hierarchical transcriptional network. Cell 2006; 126: 789–799.
Giguere V . Transcriptional control of energy homeostasis by the estrogen-related receptors. Endocr Rev 2008; 29: 677–696.
Riggins RB, Lan JP, Zhu Y, Klimach U, Zwart A, Cavalli LR et al. ERRgamma mediates tamoxifen resistance in novel models of invasive lobular breast cancer. Cancer Res 2008; 68: 8908–8917.
Heckler MM, Thakor H, Schafer CC, Riggins RB . ERK/MAPK regulates ERRgamma expression, transcriptional activity and receptor-mediated tamoxifen resistance in ER+ breast cancer. FEBS J 2014; 281: 2431–2442.
Ren Z, Yang H, Wang C, Ma X . The effects of PGC-1alpha on the proliferation and energy metabolism of malignant endometrial cancer cells. Onco Targets Ther 2015; 8: 769–774.
Sun Y, Wang C, Yang H, Ma X . The effect of estrogen on the proliferation of endometrial cancer cells is mediated by ERRgamma through AKT and ERK1/2. Eur J Cancer Prev 2014; 23: 418–424.
Lapenna S, Giordano A . Cell cycle kinases as therapeutic targets for cancer. Nat Rev Drug Discov 2009; 8: 547–566.
Waldman T, Kinzler KW, Vogelstein B . p21 is necessary for the p53-mediated G1 arrest in human cancer cells. Cancer Res 1995; 55: 5187–5190.
Gartel AL, Tyner AL . The role of the cyclin-dependent kinase inhibitor p21 in apoptosis. Mol Cancer Ther 2002; 1: 639–649.
Senderowicz AM . Small-molecule cyclin-dependent kinase modulators. Oncogene 2003; 22: 6609–6620.
Bianco S, Sailland J, Vanacker JM . ERRs and cancers: effects on metabolism and on proliferation and migration capacities. J Steroid Biochem Mol Biol 2012; 130: 180–185.
Deblois G, Hall JA, Perry MC, Laganiere J, Ghahremani M, Park M et al. Genome-wide identification of direct target genes implicates estrogen-related receptor alpha as a determinant of breast cancer heterogeneity. Cancer Res 2009; 69: 6149–6157.
Bernatchez G, Giroux V, Lassalle T, Carpentier AC, Rivard N, Carrier JC . ERRalpha metabolic nuclear receptor controls growth of colon cancer cells. Carcinogenesis 2013; 34: 2253–2261.
Cheung CP, Yu S, Wong KB, Chan LW, Lai FM, Wang X et al. Expression and functional study of estrogen receptor-related receptors in human prostatic cells and tissues. J Clin Endocrinol Metab 2005; 90: 1830–1844.
Yu S, Wong YC, Wang XH, Ling MT, Ng CF, Chen S et al. Orphan nuclear receptor estrogen-related receptor-beta suppresses in vitro and in vivo growth of prostate cancer cells via p21(WAF1/CIP1) induction and as a potential therapeutic target in prostate cancer. Oncogene 2008; 27: 3313–3328.
Bianco S, Lanvin O, Tribollet V, Macari C, North S, Vanacker JM . Modulating estrogen receptor-related receptor-alpha activity inhibits cell proliferation. J Biol Chem 2009; 284: 23286–23292.
Edge SB, Compton CC . The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol 2010; 17: 1471–1474.
Llovet JM, Bru C, Bruix J . Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin Liver Dis 1999; 19: 329–338.
Lee YJ, Hah YJ, Kang YN, Kang KJ, Hwang JS, Chung WJ et al. The autophagy-related marker LC3 can predict prognosis in human hepatocellular carcinoma. PLoS ONE 2013; 8: e81540.
Sanyal S, Kim JY, Kim HJ, Takeda J, Lee YK, Moore DD et al. Differential regulation of the orphan nuclear receptor small heterodimer partner (SHP) gene promoter by orphan nuclear receptor ERR isoforms. J Biol Chem 2002; 277: 1739–1748.
Chao EY, Collins JL, Gaillard S, Miller AB, Wang L, Orband-Miller LA et al. Structure-guided synthesis of tamoxifen analogs with improved selectivity for the orphan ERRgamma. Bioorg Med Chem Lett 2006; 16: 821–824.
Tremosini S, Forner A, Boix L, Vilana R, Bianchi L, Reig M et al. Prospective validation of an immunohistochemical panel (glypican 3, heat shock protein 70 and glutamine synthetase) in liver biopsies for diagnosis of very early hepatocellular carcinoma. Gut 2012; 61: 1481–1487.
Di Tommaso L, Franchi G, Park YN, Fiamengo B, Destro A, Morenghi E et al. Diagnostic value of HSP70, glypican 3, and glutamine synthetase in hepatocellular nodules in cirrhosis. Hepatology 2007; 45: 725–734.
International Consensus Group for Hepatocellular Neoplasia. Pathologic diagnosis of early hepatocellular carcinoma: a report of the International Consensus Group for Hepatocellular Neoplasia. Hepatology 2009; 49: 658–664.
Kim DK, Ryu D, Koh M, Lee MW, Lim D, Kim MJ et al. Orphan nuclear receptor estrogen-related receptor gamma (ERRgamma) is key regulator of hepatic gluconeogenesis. J Biol Chem 2012; 287: 21628–21639.
Park YY, Kim SH, Kim YJ, Kim SY, Lee TH, Lee IK et al. Polo-like kinase 2 gene expression is regulated by the orphan nuclear receptor estrogen receptor-related receptor gamma (ERRgamma). Biochem Biophys Res Commun 2007; 362: 107–113.
Acknowledgements
This work was supported by grants (NRF-2015R1A2A1A15053422 and NRF-2015R1A2A1A10052745) the National Research Foundation of Korea funded by the Ministry of Science, ICT and Future Planning, and grants (HI11C1300, HI15C0001 and HI13C1905) from the Korea Health technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on Experimental & Molecular Medicine website
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Kim, JH., Choi, YK., Byun, JK. et al. Estrogen-related receptor γ is upregulated in liver cancer and its inhibition suppresses liver cancer cell proliferation via induction of p21 and p27. Exp Mol Med 48, e213 (2016). https://doi.org/10.1038/emm.2015.115
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/emm.2015.115
This article is cited by
-
Inhibition of EZH2 and activation of ERRγ synergistically suppresses gastric cancer by inhibiting FOXM1 signaling pathway
Gastric Cancer (2021)
-
The PGC-1/ERR network and its role in precision oncology
npj Precision Oncology (2019)
-
Estrogen-related receptor gamma functions as a tumor suppressor in gastric cancer
Nature Communications (2018)
-
Transcriptome analysis of genes associated with breast cancer cell motility in response to Artemisinin treatment
BMC Cancer (2017)
