
Abstract
The International Prognostic Scoring System has been revised (IPSS-R) to predict prognosis of patients with myelodysplastic syndromes at diagnosis. To validate the use of the IPSS-R assessed before transplant rather than at diagnosis we performed a retrospective analysis of the EBMT database. A total of 579 patients had sufficient information available to calculate IPSS-R at transplant. Median overall survival (OS) from transplant was significantly different according to IPSS-R: very low 23.6 months, low 55.0 months, intermediate 19.7 months, high 13.5 months, very high 7.8 months (P<0.001). In a multivariate Cox model the following parameters were significant risk factors for OS: IPSS-R, graft source, age and prior treatment. Median relapse free survival also showed significant differences according to IPSS-R: very low: 23.6 months, low: 24.8 months, intermediate 10.6 months, high 7.9 months, very high 5.5 months (P<0.001). Multivariate risk factors for relapse-free survival (RFS) were: IPSS-R, reduced intensity conditioning, graft source and prior treatment. A trend for an increased relapse incidence was noted for very high risk IPSS-R. We conclude that the IPSS-R at transplant is a useful prognostic score for predicting OS and RFS after transplantation, capturing both disease evolution and response to prior treatment before transplant.
Similar content being viewed by others

Introduction
Myelodysplastic syndrome (MDS) is a disease with a highly variable course ranging from stable cytopenia to rapid progression to acute leukemia. Since the management of MDS is largely dependent on the anticipated prognosis of each patient, multiple scoring systems have been developed to predict prognosis using disease related parameters at diagnosis. The International Prognostic Scoring System (IPSS) has been revised to include a more detailed risk stratification of genetic changes in MDS.1 The revised IPSS (IPSS-R) allocates patients into five different risk categories with a predicted median overall survival (OS) from diagnosis from 0.8 years for the very high risk group to 8.8 years for very low risk disease.
The IPSS-R at transplant has been used to predict survival after allogeneic stem cell transplantation.2 However, nearly half of the patients received additional therapy before undergoing transplantation and in these cases IPSS-R was assessed prior to this therapy instead of prior to allografting. A recent study from Korea3 analyzed IPSS-R before and after hypomethylating therapy prior to allogeneic transplantation and found the assessment before transplant to give a better prediction of OS. Several groups have proposed new scoring systems to predict transplant outcome in MDS.3, 4 However the parameters of these scores are largely overlapping with the constituents of the IPSS-R and the improvement in predictive power was only modest compared to the IPSS-R.4
Since the IPSS-R is well established and easily available, we sought to validate it in a large cohort of patients with MDS or transformed AML from the EBMT database. Although the IPSS-R was originally developed for untreated MDS patients only, we included also patients with prior therapy before allografting as well as patients with >30% blasts to reflect the full spectrum of patients with MDS and MDS transformed to AML presenting for allogeneic transplantation.
Patients and methods
A retrospective analysis of the EBMT database was performed. All first allogeneic transplants performed for the diagnosis MDS or transformed AML evolving from MDS in the time period 1982–2010 were selected. Pediatric patients and transplants with cord blood or from mismatched donors were excluded. Only patients with available information on bone marrow blast count, cytogenetics, hemoglobin, platelets and leukocytes at transplant were used to calculate IPSS-R at transplant according to Greenberg et al.1 Since IPSS-R is among others based on the ANC which was not available in the database, the ANC was assumed to be 50% of the leukocyte count. The genetic information was scored according to Schanz et al.5 by a geneticist. Patients with incomplete or inconclusive genetic data were excluded.
Proportions were compared by the χ2 test. Outcomes of primary interest were OS and relapse-free survival (RFS), defined as survival in the absence of a new relapse or progression after transplantation. Univariate survival analyses were performed by the Kaplan–Meier method; outcomes of groups were compared with the log-rank test. Cumulative incidences of relapse (CIR) and non-relapse mortality (NRM) were calculated as each other’s competing risks. Differences in CIR and NRM between groups were compared by the Gray test. All outcomes were measured from time of transplantation onward and were artificially censored at 5 years after transplantation.
Multivariate analyses were done by Cox proportional (cause-specific) hazards regression models. Two series of models were fitted. In the first, the differential impact of the components of the IPSS-R was assessed to see if the points associated with them in the score adequately reflect this impact. In the second series, it was investigated whether IPSS-R kept its impact in the presence of classical predictors. These predictors were selected on the basis of clinical and statistical considerations in models without IPSS-R. For each outcome, a new backward stepwise selection procedure was then performed in a model containing IPSS-R and the selected classical predictors. All analyses were performed in SPSS (version 23) and R 3.0.2, with library ‘cmprsk’.
Results
A total of 3276 allogeneic transplants in patients with MDS or MDS transformed to AML performed between 1982 and 2010 were found in the database. A total of 579 patients had sufficient information to calculate IPSS-R at transplant, yielding a very low risk in 16 (2.8%), low risk in 152 (26.3%), intermediate risk in 141 (24.4%), high risk in 147 (25.4%) and very high risk in 123 (21.2%) of the cases. Most other parameters regarding patient and transplant characteristics were well balanced between the IPSS-R subgroups and are summarized in Table 1. About half of the patients were male, 22% were older than 60 years, about a third had bone marrow as graft source and 40% received a reduced-intensity conditioning. Most patients were transplanted within the first year after diagnosis. There were no significant differences in the above characteristics between the IPSS-R subgroups. The majority of patients had received MDS-treatment before undergoing allogeneic stem cell transplantation and this proportion was significantly higher in the lower risk categories, ranging from 81.2% in very low risk to 50.8% in very high risk (P=0.005).
Overall survival
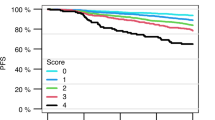
Estimation of OS at 2 years according to IPSS-R at transplant (Figure 1) was 47.4% in the very low risk group, 60.5% with low risk, 46.9% with intermediate risk, 43,5% with high risk and 27.7% in the very high risk group (P<0.001). In a univariate Cox model with the very high risk group as reference, all IPSS-R categories except the very low risk group were significant factors for OS with hazard ratios of 0.518 for very low risk, 0.444 for low risk, 0.607 for intermediate risk and 0.711 for high risk (Table 2a). When analyzing patients with and without prior treatment separately, IPSS-R was still a significant factor for OS in treatment-naïve (P=0.025) and in previously treated patients (P<0.001).

OS according to IPSS-R at transplant.
To assess the contribution of the different components of IPSS-R on transplant outcome, we performed a multivariate Cox model using the categories for genetic risk, blast count, hemoglobin, platelets and neutrophil count as parameters separately. As shown in Table 2b cytogenetic risk group (P<0.001) and bone marrow blasts (P=0.004) were significant predictors for OS while cytopenia was not.
To investigate the IPSS-R in relation to other known risk factors for transplant outcome (age, donor type, graft source, conditioning intensity, CMV-status, female donor for male patients, interval between diagnosis and transplant, year of transplant) and in particular to disease status and previous treatment, both of which were found to be unevenly distributed within the IPSS-R risk categories, we performed a multivariate Cox analysis with a selection procedure. In this analysis the following parameters were found to be significantly associated with OS: graft source (PB vs BM, HR 0.747, P=0.02), age (P=0.041), prior treatment (hazard ratio (HR) 1.695, P<0.001, and IPSS-R (P<0.001) (Table 3, complete Cox model shown in Supplementary Table 1). The size of the impact of IPSS-R was almost equal in the models with and without other risk factors.
Relapse-free survival
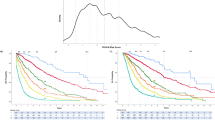
IPSS-R predicted RFS at 24 months after transplant (Figure 2) with 47.7, 52.0, 40.9, 34.2 and 23.7% in the very low, low, intermediate, high and very high risk group, respectively (P<0.001). In a univariate Cox model all IPSS-R categories except very low risk were found to be significant factors for RFS (Table 4a). Regarding the effect of the individual components of the IPSS-R on RFS, neutrophil count was found to be a significant predictor in addition to cytogenetic risk group and bone marrow blasts, while hemoglobin and platelets were not significant (Table 4b).

RFS according to IPSS-R at transplant.
In a multivariate Cox model for RFS including the above mentioned disease- and transplant-related risk factors, conditioning intensity (reduced versus myeloablative, HR 1.289, P=0.027), prior treatment (HR 1.654, P<0.001), graft source (PB vs BM, HR 0.738, P=0.011) and IPSS-R (P<0.001) were found to be significant covariates after backward selection (Table 5, complete Cox model shown in Supplementary Table 2).
NRM and relapse incidence
There was a trend for a higher cumulative relapse incidence (RI) in the very high risk group amounting to 43.8% at 24 months, whereas the RI at 24 months ranged from 26.7 to 34.2% in the other risk categories (Figure 3, P=0.20). The cumulative incidence of non-relapse mortality was 27.5% at 24 months and showed no significant differences in relation to IPSS-R at transplant in a univariate comparison (Figure 4).

Cumulative incidence of relapse according to IPSS-R at transplant.

Cumulative incidence of non-relapse mortality according to IPSS-R at transplant.
To further explore in what way the IPSS-R influences transplant outcomes, we analyzed the risk factors predicting OS and RFS in multivariate Cox models for the cause-specific hazards of relapse and NRM. IPSS-R (P<0.001) and prior treatment (HR 2.62, 95% CI 1.87–3.68, P<0.001) were found to predict relapse risk whereas IPSS-R (P=0.041) and graft source (PB vs BM, HR 0.53, 95% CI 0.37–0.75, P<0.001) were significant factors for NRM.
Discussion
Predicting the outcome after allogeneic transplantation remains a challenge for transplant physicians, in particular for diseases with a variable natural course. While parameters related to the transplant complications like age or donor type have been used widely and are considered in prognostic scores such as the EBMT score, the risks conferred by the underlying—and eventually evolving—disease are more difficult to assess. Several prognostic scores for MDS predict OS from diagnosis, at latest the IPSS-R,1 which incorporates the bone marrow blast counts, five genetic risk categories and cytopenias of the three lineages.
World Health Organisation (WHO) disease stage has previously been found to be predictive of transplant outcome.6 Our results show that WHO disease stage is no longer significant for OS or RFS if IPSS-R is assessed simultaneously, probably because of a high correlation between the variables since both are strongly related to the blast counts. IPSS risk score—assessed at diagnosis—is known to predict outcome of allogeneic transplantation.7, 8, 9 Since often some time evolves between diagnosis and transplantation and MDS-directed therapy might have been applied in between, assessing IPSS-R at diagnosis may not truly reflect the disease status at transplant.
Several attempts have been made to use disease risk scores during the course of the disease to predict transplant outcome: Alessandrino et al.6 have studied 365 patients with AML or MDS from the Italian registry and analyzed both WHO stage and WHO-based prognostic scoring system (WPSS) score at transplant or before induction chemotherapy in those patients receiving prior therapy. Both WHO stage and WPSS were strongly correlated with OS and relapse incidence in univariate and multivariate models. However since both factors were recorded before a given induction chemotherapy, response to this therapy did not enter in the risk score and had to be analyzed as a separate covariate. The achievement of CR after induction before transplantation was a significant factor for OS and relapse incidence in patients with AML, but not with RAEB I or II. It therefore appears advantageous to assess the risk score directly before transplantation to integrate both disease risk and response to prior treatment into on single risk score. Lee et al.9 have reported on transplant outcome in relation to IPSS risk as assessed at transplant in a small single center study including 68 patients. IPSS at transplant was predictive of OS and EFS and eliminated WHO disease stage and IPSS at diagnosis when entered into a multivariate model. However the IPSS score has been generally challenged to underestimate the risk of genetic changes and a novel genetic risk score to estimate survival from diagnosis in MDS patients has been published.5 This genetic five-group risk score has been recently been tested in patients undergoing allogeneic transplantation.10 The French SFGM-TC group analyzed the five group genetic score at diagnosis with regard to its prognostic relevance for allogeneic transplantation. In multivariate analysis the genetic score predicted OS after transplant with blast count at transplant and TBI-containing conditioning as significant covariates. Progression after prior therapy was also a negative factor but did not reach statistical significance. Using the same genetic risk score but assessed at transplant Deeg et al.11 found significant hazard ratios for OS for the poor and very poor risk group with no significant difference for the very good and intermediate risk groups in univariate analysis using the good risk group as reference. Besides genetic risk group, a large number of other parameters were found to predict OS in a multivariate model such as age, year of transplant, conditioning regimen, WHO disease stage, platelet count, donor type and antecedent disease. Thus the five group genetic risk score identified a subgroup of patients with an overwhelmingly high risk of relapse and mortality after transplant. Similar to the findings by Deeg et al.12, our group found the five group cytogenetic risk score to be superior for predicting transplant outcome than the categorization in the IPSS score. WHO disease category and remission status were additional prognostic factors for OS and RFS in multivariate models.
The Italian group2 has published a study investigating the role of IPSS-R to predict transplant outcome in 519 patients with MDS and oligoblastic AML and could show that the IPSS-R was prognostic for OS and relapse incidence. However, the risk assessment was performed at transplant only for patients receiving an upfront transplantation. For patients undergoing prior induction therapy the score was analyzed before induction and response to this therapy had to be captured in a separate variable. Both IPSS-R and response to induction were found to be independent factors for OS and relapse incidence. Thus assessing the IPSS-R before the start of induction therapy does not allow capture of multiple risk factors in a single risk score. In fact a small retrospective study from two Korean transplant centers3 in 201 patients of whom 115 received hypomethylating therapy prior to transplant, IPSS-R assessed at transplant was a better predictor of transplant outcome than IPSS-R before the start of hypomethylating treatment.
In our retrospective registry-based analysis including 579 patients, we confirm the validity of assessing the IPSS-R score immediately before transplant irrespective of a prior treatment and accounting for a number of known factors related to the outcome of allogeneic transplantation. Similar to the study by Yahng et al.3 we found a high proportion of patients being ‘downstaged’ before transplant, starting with AML evolved from MDS and presenting for transplant with a low risk IPSS-R after therapy. With our approach we could limit the prognostic factors for OS in a multivariate model to IPSS-R, age, graft source and prior treatment. For RFS besides IPSS-R we found graft source, conditioning intensity and prior treatment to be predictive. We therefore propose to use IPSS-R as easy and comprehensive score to capture a number of pre-transplant risk factors in a single, widely used scoring system for MDS patients.
Still our study has some limitations to consider: only very few patients fell in the very low risk category and therefor the results for this subgroup have to be taken with caution. In fact OS and RFS appeared to be inferior to the low risk group. This may partly be explained by the high level of uncertainty when analyzing survival data in a cohort of only 16 patients. In addition this subgroup showed the highest rate of prior AML (66.7%) and prior treatment (81.3%) and may biologically be more comparable to AML in complete remission than MDS. However a much larger patient cohort would be needed to further elucidate this point. The neutrophil count required to calculate IPSS-R was not available and had to be estimated based on the leukocyte count. However, given the very limited weight of the neutrophils in the IPSS-R score, we do not think this had an influence on our findings. Of note in the analysis by Della Porta2 the neutrophil count did not have any prognostic implications. Furthermore the genetic information contained in the EBMT database is far from being complete and a large number of patients had to be excluded due to lack of data. Although we cannot exclude a selection bias when analyzing a few hundred cases out of thousands, the overall and relapse-free survival of the initial cohort was comparable to the subgroup with sufficient data to calculate IPSS-R. And finally the role of induction therapy before transplant needs to be considered very carefully. While in our analysis prior treatment was a negative prognostic factor this does by no means prove the futility of induction therapy. It rather suggests that a given IPSS-R score may have a worse prognostic implication if it reflects the result of a prior treatment attempt (and thus potentially resistant disease) rather than spontaneous disease evolution. Conversely a high number of patients with transformed AML presented at transplant with a low IPSS-R risk after effective therapy and may thus have improved their prognosis after transplant. The benefit of induction treatment before allogeneic transplantation remains a controversial issue13 and can only be assessed by prospective studies.
In summary, we have shown the IPSS-R score at transplant includes many of disease- and therapy-related factors in one score and may help to identify patients with a favorable transplant outcome and those needing additional pre- or post-transplant interventions to improve prognosis. In the future the incorporation of molecular alterations such as TP53, RUNX1 or ASXL114 in the pre-transplant assessment may further improve the prediction of transplant outcome in MDS.
References
Greenberg PL, Tuechler H, Schanz J, Sanz G, Garcia-Manero G, Sole F et al. Revised international prognostic scoring system for myelodysplastic syndromes. Blood 2012; 120: 2454–2465.
Della Porta MG, Alessandrino EP, Bacigalupo A, van Lint MT, Malcovati L, Pascutto C et al. Predictive factors for the outcome of allogeneic transplantation in patients with Mds stratified according to the revised Ipss-R. Blood 2014; 123: 2333–2342.
Yahng S-A, Jeon Y-W, Yoon J-H, Shin S-H, Lee S-E, Choi Y-S et al. Dynamic prognostic value of the revised international prognostic scoring system following pretransplant hypomethylating treatment in myelodysplastic syndrome. Bone Marrow Transplant 2016; 52: 522–531.
Shaffer BC, Ahn KW, Hu Z-H, Nishihori T, Malone AK, Valcarcel D et al. Scoring system prognostic of outcome in patients undergoing allogeneic hematopoietic cell transplantation for myelodysplastic syndrome. J Clin Oncol 2016; 34: 1864–1871.
Schanz J, Tuchler H, Sole F, Mallo M, Luno E, Cervera J et al. New comprehensive cytogenetic scoring system for primary myelodysplastic syndromes (Mds) and oligoblastic acute myeloid leukemia after Mds derived from an International Database Merge. J Clin Oncol 2012; 30: 820–829.
Alessandrino EP, Della Porta MG, Bacigalupo A, Van Lint MT, Falda M, Onida F et al. Who classification and Wpss predict posttransplantation outcome in patients with myelodysplastic syndrome: a study from the Gruppo Italiano Trapianto Di Midollo Osseo (Gitmo). Blood 2008; 112: 895–902.
Rubio S, Martins C, Lacerda JF, Carmo JA, Lourenco F, Lacerda JM . Allogeneic stem cell transplantation in patients with myelodysplastic syndrome: outcome analysis according to the international prognostic scoring system. Acta Med Portuguesa 2006; 19: 343–347.
Appelbaum FR, Anderson J . Allogeneic bone marrow transplantation for myelodysplastic syndrome: outcomes analysis according to Ipss score. Leukemia 1998; 12: S25–S29.
Lee JH, Lee JH, Lim SN, Kim DY, Kim SH, Lee YS et al. Allogeneic hematopoietic cell transplantation for myelodysplastic syndrome: prognostic significance of pre-transplant Ipss score and comorbidity. Bone Marrow Transplant 2010; 45: 450–457.
Gauthier J, Damaj G, Langlois C, Robin M, Michallet M, Chevallier P et al. Contribution of Revised International Prognostic Scoring System Cytogenetics to Predict Outcome after allogeneic stem cell transplantation for myelodysplastic syndromes: a study from the French Society of Bone Marrow Transplantation and Cellular Therapy. Transplantation 2015; 99: 1672–1680.
Deeg HJ, Scott BL, Fang M, Shulman HM, Gyurkocza B, Myerson D et al. Five-group cytogenetic risk classification, monosomal karyotype, and outcome after hematopoietic cell transplantation for Mds or acute leukemia evolving from Mds. Blood 2012; 120: 1398–1408.
Koenecke C, Gohring G, de Wreede LC, van Biezen A, Scheid C, Volin L et al. Impact of the Revised International Prognostic Scoring System, Cytogenetics and Monosomal Karyotype on outcome after allogeneic stem cell transplantation for myelodysplastic syndromes and secondary acute myeloid leukemia evolving from myelodysplastic syndromes: a retrospective multicenter study of the European Society of Blood and Marrow Transplantation. Haematologica 2015; 100: 400–408.
Oliansky DM, Antin JH, Bennett JM, Deeg HJ, Engelhardt C, Heptinstall KV et al. The role of cytotoxic therapy with hematopoietic stem cell transplantation in the therapy of myelodysplastic syndromes: an evidence-based review. Biol Blood Marrow Transplant 2009; 15: 137–172.
Della Porta MG, Galli A, Bacigalupo A, Zibellini S, Bernardi M, Rizzo E et al. Clinical effects of driver somatic mutations on the outcomes of patients with myelodysplastic syndromes treated with allogeneic hematopoietic stem-cell transplantation. J Clin Oncol. 2016; 34: 3627–3637.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Scheid, C., de Wreede, L., van Biezen, A. et al. Validation of the revised IPSS at transplant in patients with myelodysplastic syndrome/transformed acute myelogenous leukemia receiving allogeneic stem cell transplantation: a retrospective analysis of the EBMT chronic malignancies working party. Bone Marrow Transplant 52, 1519–1525 (2017). https://doi.org/10.1038/bmt.2017.171
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bmt.2017.171
This article is cited by
-
Room for Improvement: A 20-Year Single Center Experience with Allogeneic Stem Cell Transplantation for Myelodysplastic Syndromes
Indian Journal of Hematology and Blood Transfusion (2022)
-
Current challenges and unmet medical needs in myelodysplastic syndromes
Leukemia (2021)
-
Allogeneic hematopoietic stem cell transplantation for myelodysplastic syndrome in adolescent and young adult patients
Bone Marrow Transplantation (2021)
-
Graft-versus-MDS effect after unrelated cord blood transplantation: a retrospective analysis of 752 patients registered at the Japanese Data Center for Hematopoietic Cell Transplantation
Blood Cancer Journal (2019)
