
Abstract
Background:
Single-nucleotide polymorphisms (SNPs) in genes involved in DNA repair are good candidates to be tested as phenotypic modifiers for carriers of mutations in the high-risk susceptibility genes BRCA1 and BRCA2. The base excision repair (BER) pathway could be particularly interesting given the relation of synthetic lethality that exists between one of the components of the pathway, PARP1, and both BRCA1 and BRCA2. In this study, we have evaluated the XRCC1 gene that participates in the BER pathway, as phenotypic modifier of BRCA1 and BRCA2.
Methods:
Three common SNPs in the gene, c.-77C>T (rs3213245) p.Arg280His (rs25489) and p.Gln399Arg (rs25487) were analysed in a series of 701 BRCA1 and 576 BRCA2 mutation carriers.
Results:
An association was observed between p.Arg280His-rs25489 and breast cancer risk for BRCA2 mutation carriers, with rare homozygotes at increased risk relative to common homozygotes (hazard ratio: 22.3, 95% confidence interval: 14.3–34, P<0.001). This association was further tested in a second series of 4480 BRCA1 and 3016 BRCA2 mutation carriers from the Consortium of Investigators of Modifiers of BRCA1 and BRCA2.
Conclusions and inte
No evidence of association was found when the larger series was analysed which lead us to conclude that none of the three SNPs are significant modifiers of breast cancer risk for mutation carriers.
Similar content being viewed by others


Main
Germ-line mutations in the BRCA1 and BRCA2 genes confer a high lifetime risk of developing breast or ovarian cancer. Estimates of the cumulative risk of breast cancer to age 70 vary from 40 to 85%, depending on the study (Easton et al, 1995; Ford et al, 1998; Antoniou et al, 2003; Chen et al, 2006; Milne et al, 2008). Environmental and other genetic factors (risk modifiers) are likely to explain these differences, at least in part. The few reliable genetic associations that have been reported to date, have all come from the Consortium of Investigators of Modifiers of BRCA1/2 (CIMBA) initiative, which was set up to provide large samples of mutation carriers to reliably assess even modest associations with single-nucleotide polymorphisms (Chenevix-Trench et al, 2007). The CIMBA has assessed risk in BRCA1/2 carriers for various SNPs in genes that had been previously found to be associated with increased breast cancer risk in the general population, mostly via genome-wide association studies (Antoniou et al, 2008, 2009). However, the first evidence of a modifier came from a candidate gene approach studying the RAD51 gene, which interacts directly with BRCA1 and BRCA2. All three genes participate in the DNA double-strand break repair by the homologous recombination pathway. Results from the CIMBA study suggested an increased risk of breast cancer for BRCA2 mutation carriers with two copies of the ‘C’ allele at the 135G → C SNP (rs 1801320) in the 5′ untranslated region of RAD51 (Antoniou et al, 2007). This result suggests that other genes involved in DNA repair could as also function as cancer risk modifiers for BRCA1 and BRCA2 mutation carriers.
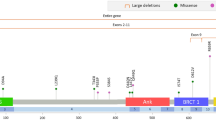
It has been proven that a deficiency in the base excision repair (BER) pathway can give rise to stalling of the replication fork and accumulation of double-strand DNA breaks which, in the presence of a defective BRCA1 or BRCA2 background, could persist and lead to cell cycle arrest or cell death (Farmer et al, 2005). This synthetic lethality interaction led us to hypothesise that SNPs in genes participating in this pathway could be potential modifiers of cancer risk in BRCA1 and BRCA2 mutation carriers. The XRCC1 gene is involved in the BER pathway and its association with different types of cancer have been extensively investigated, with no conclusive results (Kiyohara et al, 2006; Figueroa et al, 2007; Naccarati et al, 2007; Doecke et al, 2008; Fontana et al, 2008; McWilliams et al, 2008; Chang et al, 2009; Zhai et al, 2009). Four SNPs in XRCC1, three of them leading to amino acid changes (p.Arg194Trp, p.Arg280His and p.Gln399Arg) and one in the promoter region (c.-77C>T) are within the most common in terms of minor allele frequency, and a potential effect on the function of the XRCC1 protein has been suggested for them, although no clear association with breast cancer risk has been reported (Takanami et al, 2005; Hao et al, 2006; Sterpone et al, 2009; Sterpone et al, 2010). Nevertheless, the specific interaction mentioned above suggests that common variation in XRCC1 may have an effect on breast cancer risk for BRCA1 or BRCA2 mutation carriers. In this study, we aimed to assess this hypothesis for the three most studied SNPs in XRCC1, c.-77C>T (rs3213245) p.Arg280His (rs25489) and p.Gln399Arg (rs25487) using a two-stage approach.
Material and methods
Patients
Eligible subjects were female carriers of deleterious mutations in BRCA1 or BRCA2 aged ≥18 years from which complete information about year of birth, mutation description, age at last follow-up, ages at breast and or ovarian cancer diagnosis and age or date of prophylactic mastectomy was available (Antoniou et al, 2008). A total of 14 collaborating CIMBA studies from 10 countries, contributed genotypes for the study. Details of each study along with the numbers of samples included from each are provided in Table 1. The CNIO, ICO and MBCSG studies participated in the first stage in which the three SNPs, rs3213245, rs25489 and rs25487 were analysed and a potential association between rs25489 and breast cancer risk was identified. The remaining CIMBA samples were included in the stage II analysis and contributed genotypes for rs25489 only.
Subjects who reported having ethnicity other than white European were excluded from the analyses. This gave a total of 7496 female mutation carriers (4480 with mutations in BRCA1 and 3016 with mutations in BRCA2), 3891 of whom had been diagnosed with breast cancer (2293 and 1598 with mutations in BRCA1 and BRCA2, respectively). All carriers participated in clinical and/or research studies at the host institution under IRB-approved protocols.
Genotyping
The genotyping platform used by each study is detailed in Table 1. For 11 studies, matrix assisted laser desorption/ionisation time of flight mass spectrometry was applied to determine allele-specific primer extension products using Sequenom's MassARRAY system and iPLEX technology (Sequenom, San Diego, CA, USA). The design of oligonucleotides was carried out according to the guidelines of Sequenom and performed using MassARRAY Assay Design software (version 3.1). Three studies carried out genotyping by nuclease assay (Taqman). Taqman genotyping reagents were designed by Applied Biosystems (http://www.appliedbiosystems.com/) as Assays-by-Design. Genotyping was performed using the ABI PRISM 7900HT, 7700 or 7500 Sequence Detection Systems according to manufacturer's instructions. All studies complied with CIMBA genotyping quality control standards (http://www.srl.cam.ac.uk/consortia/cimba/eligibility/eligibility.html).
Statistical analysis
To test for departure from Hardy–Weinberg equilibrium a single individual was randomly selected from each family and Pearson's χ2-test (1 d.f.) was applied to genotypes from this set of individuals. The association of the SNPs with breast cancer risk was assessed by estimating hazard ratios (HRs) and their corresponding 95% confidence intervals (CIs) using weighted multivariable Cox proportional hazards regression with robust estimates of variance (Antoniou et al, 2005). For each mutation carrier, we modelled the time to diagnosis of breast cancer from birth, censoring at the first of the following events: bilateral prophylactic mastectomy, breast cancer diagnosis, ovarian cancer diagnosis, death and date last know to be alive. Subjects were considered affected if their age at censoring corresponded to their age at diagnosis of breast cancer and unaffected otherwise. Weights were assigned separately for carriers of mutations in BRCA1 and BRCA2, by age (<25, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59, 60–64, 65–69, ⩾70) and affection status, so that the weighted observed incidences in the sample agreed with established estimates for mutation carriers (Antoniou et al, 2003). This approach has been shown to adjust for the bias inherent in the oversampling of affected women because of the ascertainment criteria used (Antoniou et al, 2005).
We considered log-additive and co-dominant genetic models and tested for departure from HR=1 by applying a Wald test based on the log−HR estimate and its standard error. Additional independent variables included in all analyses were year of birth (<1930, 1930–1939, 1940–1949, 1950–1959, 1960–1969, ⩾1970), study centre and country. Heterogeneity in HRs by study centre was assessed by the χ2 equivalent of a Wald test based on the interaction terms for the per-allele effect by centre (on 13 d.f.). A number of sensitivity analyses were applied, including censoring at bilateral prophylactic oophorectomy (BPO), adjusting for BPO (as a time-varying covariate) and excluding prevalent cases, defined as those diagnosed more than 3 years before the interview.
All statistical analyses were carried out using Stata: Release 10 (StataCorp. 2007. Stata Statistical Software: Release 10.0. College Station, TX, USA: Stata Corporation LP). Robust estimates of variance were calculated using the cluster sub-command, applied to an identifier variable unique to each family.
Results and discussion
In this study, we aimed to evaluate the role of three of the most studied SNPs in the XRCC1 gene, c.-77C>T (rs3213245) p.Arg280His (rs25489) and p.Gln399Arg (rs25487) as modifiers of breast cancer risk in BRCA1 and BRCA2 mutation carriers. The study was conducted in two stages, the first analysing the three SNPs in 1277 mutation carries (701 in BRCA1 and 576 in BRCA2) from three CIMBA study centres (CNIO, ICO and MBCSG). No evidence of association was detected for c.-77C>T or p.Gln399Arg with breast cancer risk in neither BRCA1 nor BRCA2 mutation carriers (P⩾0.2). However, an association was observed between p.Arg280His and breast cancer risk for BRCA2 mutation carriers, with rare homozygotes at increased risk relative to common homozygotes (HR: 22.3, 95% CI: 14.3–34, P<0.001; Table 2). The apparent increased risk was consistent with the fact that the 280His allele decreases DNA repair capacity (Takanami et al, 2005; Pachkowski et al, 2006), however the analysis was based on a very small number (N=2) of homozygous women diagnosed at a very early age and it was therefore essential that this result be investigated in a larger sample set.
We therefore extended the analysis of the p.Arg280His-rs25489 SNP to 6219 carriers from 11 additional CIMBA study centres. Results from stage II and both stages combined are summarised in Table 2. No evidence of an association of AA vs GG homozygotes with breast cancer risk was observed for BRCA2 mutation carriers (HR: 0.73, 95% CI: 0.21–2.52, P=0.6 in stage II and HR: 1.08, 95% CI: 0.37–3.17, P=0.9 in the combined), nor for BRCA1 mutation carriers or all mutation carriers combined. We observed no evidence of between-study heterogeneity for carriers of mutations in BRCA2 (P=0.8). There was evidence of heterogeneity in the per-allele HR for BRCA1 mutation carriers (P=0.006); exclusion of subjects from potential outlier studies did not eliminated this evidence (P<0.05) and the estimated HR estimate did not change substantially. Several sensitivity analyses were carried out (see Materials and methods), but results did not change substantially and so only those from the main analysis are presented in this report.
Our results do not provide support for the hypothesis that the three most common and putatively functional SNPs in XRCC1 modify breast cancer risk for BRCA1 and BRCA2 mutation carriers. However, given the demonstrated interaction that exists between the homologous recombination and BER DNA repair pathways, additional SNPs in XRCC1 and other genes involved in BER should be assessed as risk modifiers for BRCA1/2 mutation carriers in future studies.
Change history
29 March 2012
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Antoniou A, Pharoah PD, Narod S, Risch HA, Eyfjord JE, Hopper JL, Loman N, Olsson H, Johannsson O, Borg A, Pasini B, Radice P, Manoukian S, Eccles DM, Tang N, Olah E, Anton-Culver H, Warner E, Lubinski J, Gronwald J, Gorski B, Tulinius H, Thorlacius S, Eerola H, Nevanlinna H, Syrjakoski K, Kallioniemi OP, Thompson D, Evans C, Peto J, Lalloo F, Evans DG, Easton DF (2003) Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case Series unselected for family history: a combined analysis of 22 studies. Am J Hum Genet 72: 1117–1130
Antoniou AC, Goldgar DE, Andrieu N, Chang-Claude J, Brohet R, Rookus MA, Easton DF (2005) A weighted cohort approach for analysing factors modifying disease risks in carriers of high-risk susceptibility genes. Genet Epidemiol 29: 1–11
Antoniou AC, Sinilnikova OM, McGuffog L, Healey S, Nevanlinna H, Heikkinen T, Simard J, Spurdle AB, Beesley J, Chen X, Neuhausen SL, Ding YC, Couch FJ, Wang X, Fredericksen Z, Peterlongo P, Peissel B, Bonanni B, Viel A, Bernard L, Radice P, Szabo CI, Foretova L, Zikan M, Claes K, Greene MH, Mai PL, Rennert G, Lejbkowicz F, Andrulis IL, Ozcelik H, Glendon G, Gerdes AM, Thomassen M, Sunde L, Caligo MA, Laitman Y, Kontorovich T, Cohen S, Kaufman B, Dagan E, Baruch RG, Friedman E, Harbst K, Barbany-Bustinza G, Rantala J, Ehrencrona H, Karlsson P, Domchek SM, Nathanson KL, Osorio A, Blanco I, Lasa A, Benitez J, Hamann U, Hogervorst FB, Rookus MA, Collee JM, Devilee P, Ligtenberg MJ, van der Luijt RB, Aalfs CM, Waisfisz Q, Wijnen J, van Roozendaal CE, Peock S, Cook M, Frost D, Oliver C, Platte R, Evans DG, Lalloo F, Eeles R, Izatt L, Davidson R, Chu C, Eccles D, Cole T, Hodgson S, Godwin AK, Stoppa-Lyonnet D, Buecher B, Leone M, Bressac-de Paillerets B, Remenieras A, Caron O, Lenoir GM, Sevenet N, Longy M, Ferrer SF, Prieur F, Goldgar D, Miron A, John EM, Buys SS, Daly MB, Hopper JL, Terry MB, Yassin Y, Singer C, Gschwantler-Kaulich D, Staudigl C, Hansen TO, Barkardottir RB, Kirchhoff T, Pal P, Kosarin K, Offit K, Piedmonte M, Rodriguez GC, Wakeley K, Boggess JF, Basil J, Schwartz PE, Blank SV, Toland AE, Montagna M, Casella C, Imyanitov EN, Allavena A, Schmutzler RK, Versmold B, Engel C, Meindl A, Ditsch N, Arnold N, Niederacher D, Deissler H, Fiebig B, Suttner C, Schonbuchner I, Gadzicki D, Caldes T, de la Hoya M, Pooley KA, Easton DF, Chenevix-Trench G (2009) Common variants in LSP1, 2q35 and 8q24 and breast cancer risk for BRCA1 and BRCA2 mutation carriers. Hum Mol Genet 18: 4442–4456
Antoniou AC, Sinilnikova OM, Simard J, Leone M, Dumont M, Neuhausen SL, Struewing JP, Stoppa-Lyonnet D, Barjhoux L, Hughes DJ, Coupier I, Belotti M, Lasset C, Bonadona V, Bignon YJ, Rebbeck TR, Wagner T, Lynch HT, Domchek SM, Nathanson KL, Garber JE, Weitzel J, Narod SA, Tomlinson G, Olopade OI, Godwin A, Isaacs C, Jakubowska A, Lubinski J, Gronwald J, Gorski B, Byrski T, Huzarski T, Peock S, Cook M, Baynes C, Murray A, Rogers M, Daly PA, Dorkins H, Schmutzler RK, Versmold B, Engel C, Meindl A, Arnold N, Niederacher D, Deissler H, Spurdle AB, Chen X, Waddell N, Cloonan N, Kirchhoff T, Offit K, Friedman E, Kaufmann B, Laitman Y, Galore G, Rennert G, Lejbkowicz F, Raskin L, Andrulis IL, Ilyushik E, Ozcelik H, Devilee P, Vreeswijk MP, Greene MH, Prindiville SA, Osorio A, Benitez J, Zikan M, Szabo CI, Kilpivaara O, Nevanlinna H, Hamann U, Durocher F, Arason A, Couch FJ, Easton DF, Chenevix-Trench G (2007) RAD51 135G → C modifies breast cancer risk among BRCA2 mutation carriers: results from a combined analysis of 19 studies. Am J Hum Genet 81: 1186–1200
Antoniou AC, Spurdle AB, Sinilnikova OM, Healey S, Pooley KA, Schmutzler RK, Versmold B, Engel C, Meindl A, Arnold N, Hofmann W, Sutter C, Niederacher D, Deissler H, Caldes T, Kampjarvi K, Nevanlinna H, Simard J, Beesley J, Chen X, Neuhausen SL, Rebbeck TR, Wagner T, Lynch HT, Isaacs C, Weitzel J, Ganz PA, Daly MB, Tomlinson G, Olopade OI, Blum JL, Couch FJ, Peterlongo P, Manoukian S, Barile M, Radice P, Szabo CI, Pereira LH, Greene MH, Rennert G, Lejbkowicz F, Barnett-Griness O, Andrulis IL, Ozcelik H, Gerdes AM, Caligo MA, Laitman Y, Kaufman B, Milgrom R, Friedman E, Domchek SM, Nathanson KL, Osorio A, Llort G, Milne RL, Benitez J, Hamann U, Hogervorst FB, Manders P, Ligtenberg MJ, van den Ouweland AM, Peock S, Cook M, Platte R, Evans DG, Eeles R, Pichert G, Chu C, Eccles D, Davidson R, Douglas F, Godwin AK, Barjhoux L, Mazoyer S, Sobol H, Bourdon V, Eisinger F, Chompret A, Capoulade C, Bressac-de Paillerets B, Lenoir GM, Gauthier-Villars M, Houdayer C, Stoppa-Lyonnet D, Chenevix-Trench G, Easton DF (2008) Common breast cancer-predisposition alleles are associated with breast cancer risk in BRCA1 and BRCA2 mutation carriers. Am J Hum Genet 82: 937–948
Chang JS, Wrensch MR, Hansen HM, Sison JD, Aldrich MC, Quesenberry Jr CP, Seldin MF, Kelsey KT, Wiencke JK (2009) Base excision repair genes and risk of lung cancer among San Francisco Bay Area Latinos and African-Americans. Carcinogenesis 30: 78–87
Chen S, Iversen ES, Friebel T, Finkelstein D, Weber BL, Eisen A, Peterson LE, Schildkraut JM, Isaacs C, Peshkin BN, Corio C, Leondaridis L, Tomlinson G, Dutson D, Kerber R, Amos CI, Strong LC, Berry DA, Euhus DM, Parmigiani G (2006) Characterization of BRCA1 and BRCA2 mutations in a large United States sample. J Clin Oncol 24: 863–871
Chenevix-Trench G, Milne RL, Antoniou AC, Couch FJ, Easton DF, Goldgar DE (2007) An international initiative to identify genetic modifiers of cancer risk in BRCA1 and BRCA2 mutation carriers: the Consortium of Investigators of Modifiers of BRCA1 and BRCA2 (CIMBA). Breast Cancer Res 9: 104
Doecke J, Zhao ZZ, Pandeya N, Sadeghi S, Stark M, Green AC, Hayward NK, Webb PM, Whiteman DC (2008) Polymorphisms in MGMT and DNA repair genes and the risk of esophageal adenocarcinoma. Int J Cancer 123: 174–180
Easton DF, Ford D, Bishop DT (1995) Breast and ovarian cancer incidence in BRCA1-mutation carriers. Breast Cancer Linkage Consortium. Am J Hum Genet 56: 265–271
Farmer H, McCabe N, Lord CJ, Tutt AN, Johnson DA, Richardson TB, Santarosa M, Dillon KJ, Hickson I, Knights C, Martin NM, Jackson SP, Smith GC, Ashworth A (2005) Targeting the DNA repair defect in BRCA mutant cells as a therapeutic strategy. Nature 434: 917–921
Figueroa JD, Malats N, Real FX, Silverman D, Kogevinas M, Chanock S, Welch R, Dosemeci M, Tardon A, Serra C, Carrato A, Garcia-Closas R, Castano-Vinyals G, Rothman N, Garcia-Closas M (2007) Genetic variation in the base excision repair pathway and bladder cancer risk. Hum Genet 121: 233–242
Fontana L, Bosviel R, Delort L, Guy L, Chalabi N, Kwiatkowski F, Satih S, Rabiau N, Boiteux JP, Chamoux A, Bignon YJ, Bernard-Gallon DJ (2008) DNA repair gene ERCC2, XPC, XRCC1, XRCC3 polymorphisms and associations with bladder cancer risk in a French cohort. Anticancer Res 28: 1853–1856
Ford D, Easton DF, Stratton M, Narod S, Goldgar D, Devilee P, Bishop DT, Weber B, Lenoir G, Chang-Claude J, Sobol H, Teare MD, Struewing J, Arason A, Scherneck S, Peto J, Rebbeck TR, Tonin P, Neuhausen S, Barkardottir R, Eyfjord J, Lynch H, Ponder BA, Gayther SA, Zelada-Hedman M, the Breast Cancer Linkage Consortium (1998) Genetic heterogeneity and penetrance analysis of the BRCA1 and BRCA2 genes in breast cancer families. The Breast Cancer Linkage Consortium. Am J Hum Genet 62: 676–689
Hao B, Miao X, Li Y, Zhang X, Sun T, Liang G, Zhao Y, Zhou Y, Wang H, Chen X, Zhang L, Tan W, Wei Q, Lin D, He F (2006) A novel T-77C polymorphism in DNA repair gene XRCC1 contributes to diminished promoter activity and increased risk of non-small cell lung cancer. Oncogene 25: 3613–3620
Kiyohara C, Takayama K, Nakanishi Y (2006) Association of genetic polymorphisms in the base excision repair pathway with lung cancer risk: a meta-analysis. Lung Cancer 54: 267–283
McWilliams RR, Bamlet WR, Cunningham JM, Goode EL, de Andrade M, Boardman LA, Petersen GM (2008) Polymorphisms in DNA repair genes, smoking, and pancreatic adenocarcinoma risk. Cancer Res 68: 4928–4935
Milne RL, Osorio A, Cajal TR, Vega A, Llort G, de la Hoya M, Diez O, Alonso MC, Lazaro C, Blanco I, Sanchez-de-Abajo A, Caldes T, Blanco A, Grana B, Duran M, Velasco E, Chirivella I, Cardenosa EE, Tejada MI, Beristain E, Miramar MD, Calvo MT, Martinez E, Guillen C, Salazar R, San Roman C, Antoniou AC, Urioste M, Benitez J (2008) The average cumulative risks of breast and ovarian cancer for carriers of mutations in BRCA1 and BRCA2 attending genetic counseling units in Spain. Clin Cancer Res 14: 2861–2869
Naccarati A, Pardini B, Hemminki K, Vodicka P (2007) Sporadic colorectal cancer and individual susceptibility: a review of the association studies investigating the role of DNA repair genetic polymorphisms. Mutat Res 635: 118–145
Pachkowski BF, Winkel S, Kubota Y, Swenberg JA, Millikan RC, Nakamura J (2006) XRCC1 genotype and breast cancer: functional studies and epidemiologic data show interactions between XRCC1 codon 280 His and smoking. Cancer Res 66: 2860–2868
Sterpone S, Cornetta T, Angioni A, Fiscarelli E, Lucidi V, Testa A, Cozzi R (2009) DNA damage and related modifier genes in Italian cystic fibrosis patients. Biol Res 42: 477–486
Sterpone S, Mastellone V, Padua L, Novelli F, Patrono C, Cornetta T, Giammarino D, Donato V, Testa A, Cozzi R (2010) Single-nucleotide polymorphisms in BER and HRR genes, XRCC1 haplotypes and breast cancer risk in Caucasian women. J Cancer Res Clin Oncol 136: 631–636
Takanami T, Nakamura J, Kubota Y, Horiuchi S (2005) The Arg280His polymorphism in X-ray repair cross-complementing gene 1 impairs DNA repair ability. Mutat Res 582: 135–145
Zhai XD, Mo YN, Xue XQ, Zhao GS, Gao LB, Ai HW, Ye Y (2009) XRCC1 codon 280 and ERCC2 codon 751 polymorphisms and risk of esophageal squamous cell carcinoma in a Chinese population. Bull Cancer 96: E61–E65
Acknowledgements
Spanish National Cancer Centre (CNIO): We thank RM Alonso for her excellent technical assistance. The samples studied at CNIO were recruited by the Spanish Consortium for the Study of Genetic Modifiers of BRCA1 and BRCA2. This study was partially supported by Mutua Madrileña Foundations. The research leading to these results has received funding from the Ministry of Science (FIS08-1120) and European Community’s Seventh Framework Programme under grant agreement no 223175 (HEALTH-F2-2009-223175). The Italian study (Milan Breast Cancer Study Group, MBCSG) is funded in part by grants from Fondazione Italiana per la Ricerca sul Cancro (Special Project ‘Hereditary tumors’), Associazione Italiana per la Ricerca sul Cancro (4017), Ministero della Salute (RFPS-2006-3-340203, Extraordinary National Cancer Program 2006 ‘Alleanza contro il Cancro’ and ‘Progetto Tumori Femminili’), Ministero dell’Universita’ e Ricerca (RBLAO3-BETH) and by funds from Italian citizens who allocated the 5 × 1000 share of their tax payment in support of the Fondazione IRCCS Istituto Nazionale Tumori, according to Italian laws (INT-Institutional strategic projects ‘5 × 1000’). The MBCSG acknowledges Marco Pierotti and Carla B Ripamonti of the Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy; Monica Barile and Loris Bernard of the Istituto Europeo di Oncologia, Milan, Italy. The Kathleen Cuningham Consortium for Research into Familial Breast Cancer (kConFab): We wish to thank Heather Thorne, Eveline Niedermayr, all the kConFab research nurses and staff, the heads and staff of the Family Cancer Clinics, and the Clinical Follow Up Study (funded by NHMRC grants 145684, 288704 and 454508) for their contributions to this resource, and the many families who contribute to kConFab. The kConFab is supported by grants from the National Breast Cancer Foundation, the National Health and Medical Research Council and by the Queensland Cancer Fund, the Cancer Councils of New South Wales, Victoria, Tasmania and South Australia, and the Cancer Foundation of Western Australia. ABS is an NHMRC Senior Research Fellow, and GCT is an NHMRC Senior Principal Research Fellow. The MAYO study is supported in part by National Institute of Health Grants CA116167, CA122340, CA128978, a Specialized Program of Research Excellence grant in Breast Cancer P50 CA116201, a grant from the Breast Cancer Research Foundation, and a grant from the Komen Foundation for the Cure. The PBCS is supported by a grant of the Institute for Tumors of Tuscany. The Swedish BRCA1 and BRCA2 study collaborators (SWE-BRCA): SWE-BRCA collaborators: Per Karlsson, Margareta Nordling, Annika Bergman and Zakaria Einbeigi, Gothenburg, Sahlgrenska University Hospital; Marie Stenmark-Askmalm and Sigrun Liedgren, Linköping University Hospital; Åke Borg, Niklas Loman, Håkan Olsson, Ulf Kristoffersson, Helena Jernström, Katja Harbst and Karin Henriksson, Lund University Hospital; Annika Lindblom, Brita Arver, Anna von Wachenfeldt, Annelie Liljegren, Gisela Barbany-Bustinza and Johanna Rantala, Stockholm, Karolinska University Hospital; Beatrice Melin, Henrik Grönberg, Eva-Lena Stattin and Monica Emanuelsson, Umeå University Hospital; Hans Ehrencrona, Richard Rosenquist Brandell and Niklas Dahl, Uppsala University Hospital. The UPENN study is supported by the Breast Cancer Research Foundation and the MacDonald Family Foundation. The HEBON Collaborating Centres: Coordinating center: Netherlands Cancer Institute, Amsterdam, NL: FBL Hogervorst, S Verhoef, M Verheus, LJ van ‘t Veer, FE van Leeuwen, MA Rookus; Erasmus Medical Center, Rotterdam, NL: M Collée, AMW van den Ouweland, A Jager, MJ Hooning, MMA Tilanus-Linthorst, C Seynaeve; Leiden University Medical Center, NL, Leiden: CJ van Asperen, JT Wijnen, MP Vreeswijk, RA Tollenaar, P Devilee; Radboud University Nijmegen Medical Center, Nijmegen, NL: MJ Ligtenberg, N Hoogerbrugge; University Medical Center Utrecht, Utrecht, NL: MG Ausems, RB van der Luijt; Amsterdam Medical Center, NL: CM Aalfs, TA van Os; VU University Medical Center, Amsterdam, NL: JJP Gille, Q Waisfisz, HEJ Meijers-Heijboer; University Hospital Maastricht, Maastricht, NL: EB Gomez-Garcia, CE van Roozendaal, Marinus J Blok, B Caanen; University Medical Center Groningen University, NL: JC Oosterwijk, AH van der Hout, MJ Mourits; The Netherlands Foundation for the detection of hereditary tumours, Leiden, NL: HF Vasen. The HEBON study is supported by the Dutch Cancer Society grants NKI1998-1854, NKI2004-3088 and NKI2007-3756. Epidemiological study of BRCA1 and BRCA2 mutation carriers (EMBRACE): EMBRACE is supported by Cancer Research UK Grants C1287/A10118 and C1287/A11990. Bridget Curzon is supported by Cancer Research UK Grant C8197/A10123. The Investigators at The Institute of Cancer Research and The Royal Marsden NHS Foundation Trust are supported by an NIHR grant to the Biomedical Research Centre at The Institute of Cancer Research and The Royal Marsden NHS Foundation Trust. Ros Eeeles, Elizabeth Bancroft and Lucia D’Mello are also supported by Cancer Research UK Grant C5047/A8385. D Gareth Evans and Fiona Lalloo are supported by an NIHR grant to the Biomedical Research Centre, Manchester. Douglas Easton is the PI of the study. EMBRACE Collaborating Centres are: Coordinating Centre, Cambridge: Susan Peock, Margaret Cook, Clare Oliver, Debra Frost. North of Scotland Regional Genetics Service, Aberdeen: Zosia Miedzybrodzka, Helen Gregory. Northern Ireland Regional Genetics Service, Belfast: Patrick Morrison, Lisa Jeffers. West Midlands Regional Clinical Genetics Service, Birmingham: Trevor Cole, Carole McKeown, Kai-ren Ong, Jonathan Hoffman. South West Regional Genetics Service, Bristol: Alan Donaldson. East Anglian Regional Genetics Service, Cambridge: Joan Paterson, Sarah Downing, Amy Taylor. Medical Genetics Services for Wales, Cardiff: Alexandra Murray, Mark T Rogers, Emma McCann. St James's Hospital, Dublin and National Centre for Medical Genetics, Dublin: M John Kennedy, David Barton. South East of Scotland Regional Genetics Service, Edinburgh: Mary Porteous, Sarah Drummond. Peninsula Clinical Genetics Service, Exeter: Carole Brewer, Emma Kivuva, Anne Searle, Selina Goodman, Kathryn Hill. West of Scotland Regional Genetics Service, Glasgow: Rosemarie Davidson, Victoria Murday, Nicola Bradshaw, Lesley Snadden, Mark Longmuir, Catherine Watt, Sarah Gibson. South East Thames Regional Genetics Service, Guys Hospital London: Louise Izatt, Chris Jacobs, Caroline Langman, Anna Whaite. North West Thames Regional Genetics Service, Harrow: Huw Dorkins. Leicestershire Clinical Genetics Service, Leicester: Julian Barwell. Yorkshire Regional Genetics Service, Leeds: Julian Adlard, Carol Chu, Julie Miller. Merseyside and Cheshire Clinical Genetics Service, Liverpool: Ian Ellis, Catherine Houghton. Manchester Regional Genetics Service, Manchester: D Gareth Evans, Fiona Lalloo, Jane Taylor. North East Thames Regional Genetics Service, London: Lucy Side, Alison Male, Cheryl Berlin. Nottingham Centre for Medical Genetics, Nottingham: Jacqueline Eason, Rebecca Collier. Northern Clinical Genetics Service, Newcastle: Fiona Douglas, Oonagh Claber. Oxford Regional Genetics Service, Oxford: Lisa Walker, Diane McLeod, Dorothy Halliday, Sarah Durell, Barbara Stayner. The Institute of Cancer Research and Royal Marsden NHS Foundation Trust: Ros Eeles, Susan Shanley, Nazneen Rahman, Richard Houlston, Elizabeth Bancroft, Lucia D’Mello, Elizabeth Page, Audrey Ardern-Jones, Kelly Kohut, Jennifer Wiggins, Elena Castro, Anitra Mitra, Lisa Robertson. North Trent Clinical Genetics Service, Sheffield: Jackie Cook, Oliver Quarrell, Cathryn Bardsley. South West Thames Regional Genetics Service, London: Shirley Hodgson, Sheila Goff, Glen Brice, Lizzie Winchester, Charlotte Eddy, Vishakha Tripathi, Virginia Attard. Wessex Clinical Genetics Service, Princess Anne Hospital, Southampton: Diana Eccles, Anneke Lucassen, Gillian Crawford, Donna McBride, Sarah Smalley. University of Kansas Medical Center: AK Godwin was funded by U01CA69631, 5U01CA113916 and the Eileen Stein Jacoby Fund. The HEBCS study has been financially supported by the Helsinki University Central Hospital Research Fund, Academy of Finland (132473), the Finnish Cancer Society and the Sigrid Juselius Foundation. Iceland Landspitali – University Hospital study is supported by the Landspitali University Hospital Research Fund and the Icelandic association: ‘Walking for Breast Cancer Research’. AC Antoniou is a Cancer Research UK Senior Cancer Research Fellow, L McGuffog, the CIMBA genotyping and data management are funded by Cancer Research UK.
Author information
Authors and Affiliations
Consortia
Corresponding author
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Osorio, A., Milne, R., Alonso, R. et al. Evaluation of the XRCC1 gene as a phenotypic modifier in BRCA1/2 mutation carriers. Results from the consortium of investigators of modifiers of BRCA1/BRCA2. Br J Cancer 104, 1356–1361 (2011). https://doi.org/10.1038/bjc.2011.91
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bjc.2011.91
