
Abstract
Background:
High-temperature cooked meat contains two families of carcinogens, heterocyclic amines (HCAs) and polycyclic aromatic hydrocarbons (PAHs). Given the kidneys’ role in metabolism and urinary excretion of these compounds, we investigated meat-derived mutagens, as well as meat intake and cooking methods, in a population-based case–control study conducted in metropolitan Detroit and Chicago.
Methods:
Newly diagnosed, histologically confirmed adenocarcinoma of the renal parenchyma (renal cell carcinoma (RCC)) cases (n=1192) were frequency matched on age, sex, and race to controls (n=1175). The interviewer-administered Diet History Questionnaire (DHQ) included queries for meat-cooking methods and doneness with photographic aids. Levels of meat mutagens were estimated using the DHQ in conjunction with the CHARRED database.
Results:
The risk of RCC increased with intake of barbecued meat (Ptrend=0.04) and the PAH, benzo(a)pyrene (BaP) (multivariable-adjusted odds ratio and 95% confidence interval, highest vs lowest quartile: 1.50 (1.14, 1.95), Ptrend=0.001). With increasing BaP intake, the risk of RCC was more than twofold in African Americans and current smokers (Pinteraction<0.05). We found no association for HCAs or overall meat intake.
Conclusion:
BaP intake, a PAH in barbecued meat, was positively associated with RCC. These biologically plausible findings advocate further epidemiological investigation into dietary intake of BaP and risk of RCC.
Similar content being viewed by others


Main
Renal cell carcinoma (RCC), the most common kidney neoplasm in adults, originates in the lining of the proximal convoluted tubule, where glucose, amino acids, uric acid, and inorganic salts are reabsorbed into the filtrate (Barjorin, 2007). Renal cell carcinoma is more common in men than women, and the rates remain higher in African Americans (Chow et al, 2010; Jemal et al, 2010). Despite associations with diet-related chronic conditions, such as obesity, hypertension, and diabetes, dietary risk factors for RCC are not well established (World Cancer Research Fund/American Institute for Cancer Research, 2007; Chow et al, 2010). Intake of fruits and vegetables may lower RCC risk (Rashidkhani et al, 2005; Lee et al, 2006), whereas high meat intake may increase risk (Faramawi et al, 2007; Aune et al, 2009; Dolwick Grieb et al, 2009), but the epidemiological evidence for various aspects of diet is largely inconsistent.
Cooking of meat at high temperatures may result in the formation and ingestion of carcinogenic compounds, including heterocyclic amines (HCAs) and polycyclic aromatic hydrocarbons (PAHs) (Rothman et al, 1993; Phillips, 1999; Sinha and Norat, 2002). Heterocyclic amines, the pyrolysis products of amino acids and creatine/creatinine, are formed in the meat's fatty juices upon direct contact with a high-heat cooking surface, such as during pan-frying (Sinha et al, 1998). Meat cooked above an open flame or embers, as with barbecuing or grilling, contains the highest levels of PAHs in the smoke formed as the meat's fatty juices drip onto the heat source (Kazerouni et al, 2001).
Dietary intake of HCAs and benzo(a)pyrene (BaP), a PAH found in the diet (Rothman et al, 1993; Kazerouni et al, 2001), have been linked to tumour formation at multiple organ sites in animal feeding studies (Nagao and Sugimura, 1993; Sinha and Norat, 2002). These compounds have also been associated with cancers of the colorectum (Sinha et al, 2005b; Cross et al, 2010), lung (Lam et al, 2009; Tasevska et al, 2009), pancreas (Anderson et al, 2005; Stolzenberg-Solomon et al, 2007), prostate (Cross et al, 2005), and breast (Sinha et al, 2000) in several large epidemiological investigations; however, results across studies and cancer sites are not consistent (Alaejos et al, 2008; Mignone et al, 2009; Tasevska et al, 2010; Wu et al, 2010). Despite the kidneys’ role in metabolism and urinary excretion of these compounds (Turteltaub et al, 1997; Peters et al, 2004), human investigations of meat mutagens and kidney cancer are sparse and limited by small numbers of cases (Lindblad et al, 1997; De Stefani et al, 1998; Augustsson et al, 1999), narrow range of intake (Augustsson et al, 1999), and/or lack of comprehensive assessments of cooking methods and doneness to calculate the levels of potential meat-cooking carcinogens (Wolk et al, 1996; Lindblad et al, 1997). We investigated intake of meat and meat-related mutagens in relation to RCC in a large, population-based case–control study of US men and women who completed a Diet History Questionnaire (DHQ) with a meat-cooking module. We also examined whether these associations varied by race, gender, or smoking status.
Materials and methods
The Kidney Cancer Study (United States), a population-based case–control study conducted in metropolitan Detroit and Chicago, is described elsewhere (Karami et al, 2010). Briefly, Caucasian (CA) and African American (AA) men and women between 20 and 79 years of age were eligible for the study. Cases were comprised of newly diagnosed, histologically confirmed adenocarcinoma of the renal parenchyma (RCC (ICD-O2-C64.9)). Cases were ascertained through the Metropolitan Detroit Cancer Surveillance System (Surveillance Epidemiology and End Results (SEER) program member) between February 2002 and July 2006 (CAs) or January 2007 (AAs), and through review of pathology reports for cases diagnosed in 2003 at Cook County, Chicago Hospitals. Community controls were selected from the Department of Motor Vehicle (DMV) identification records (aged 20–64 years) and Medicare beneficiary files (aged 65 years and older), and frequency-matched to cases on age (at 5-year intervals), sex, race, and centre. The sampling strategy employed to increase the number of AA participants, as well as recruitment and participation rates, is described in detail elsewhere (DiGaetano et al, 2003; Karami et al, 2010; Li et al, 2011). Briefly, of the 1918 cases identified and 2718 presumed eligible controls, 341 cases and 449 controls could not be located. Of the 1571 cases we sought to enrol, 1217 cases (77.5%) entered the study (221 declined participation and 133 were not interviewed owing to serious illness, impairment, or failure to respond to multiple contact attempts). Of the 2269 controls we attempted to recruit, 677 declined participation and 357 were unable to be interviewed; thus, 54.4% (1235 controls) participated.
Trained staff administered an in-home, computer-assisted interview to elicit information from participants on demographics, use of tobacco and alcohol, diet (described in detail below), height and weight history, family history of cancer, and medical history. All participants provided written informed consent and study centres were approved by their respective human subjects review boards.
Participants were excluded from the present diet analysis if they did not complete the DHQ (8 cases, 11 controls); reported extreme or implausible values for total non-alcohol energy intake (apparent outliers in the top and bottom 1% of the control distribution: <600 kcal or >6000 kcal; 19 cases, 18 controls); or if the interviewer noted issues with the participant's cognitive recall and/or conflicting responses to repetitive sequences (15 cases, 14 controls). This resulted in a final sample of 1175 cases and 1192 controls.
Dietary assessment
The modified DHQ collected information on usual adult diet 2 years before the reference date (date of diagnosis for cases or date of sample selection for controls) (Mares-Perlman et al, 1993; Willett, 1998; Subar et al, 2001). The DHQ was interviewer-administered and queried the frequency of intake of a wide range of foods (cereals and grains, fruits, vegetables, legumes, meats, dairy, desserts, fast foods), beverages (water, non-alcoholic, and alcoholic), and vitamin supplements. Each section included additional questions to collect details on the way the food was usually consumed (e.g., raw, cooked, canned, or pickled vegetables; chicken with or without skin; fried, baked, or mashed potatoes) and items typically added to food (e.g., milk or sugar to coffee or cereal, fat or meat used to cook or flavour greens, salad dressing, gravy, butter, syrup). For beverages, the number of glasses or cans was recorded. However, to decrease respondent burden and the potential for error, standard portion sizes were used to derive gram values for food items (Subar et al, 2000).
The following meat, poultry, and fish items were queried and mutually exclusive variables created: processed meat (red processed: bacon, sausage, ham hocks/smoked pork added to greens; and mixed processed: deli meat/cold cuts, hot dogs); red meat, not processed (beef: hamburger, ground beef/beef stew, roast beef/pot roast, beef steak; and pork: ham/ham-steak, pork chops, pork roast, pork/beef ribs); and white meat (poultry: chicken, turkey, fried chicken, ground chicken/turkey; and fish: canned/smoked/salted fish, fresh fish/seafood, fried fish). Standard fractions of meat components of mixed dishes such as pizza, pasta, and chilli/stew (USDA, 2008) were also included as a ‘red meat mix’ variable.
The meat portion of the DHQ included a meat-cooking module (Cantwell et al, 2004; Sinha et al, 2005a) with corresponding queries for cooking method (grilled or barbecued, baked or roasted, oven-broiled, breaded and fried, pan-fried without breading, boiled or stewed, microwaved, brown n’ serve, other, don’t know). Photographic models were used to help participants select a level of doneness (inside and outside) on an incremental scale (rare, medium, medium-well, well, very-well done) (Sinha and Rothman, 1997; Anderson et al, 2005). Frequency of meat intake, usual cooking method, and level of doneness were linked to the ‘computerized HCA resource for research in epidemiology of disease’ (CHARRED; http://charred.cancer.gov/) database of measured mutagenicity in cooked meats to estimate values (ng per day) of three HCAs (2-amino-1-methyl-6-phenyl-imidazo(4,5-b)pyridine (PhIP), 2-amino-3,8-dimethylimidazo(4,5-f)quinoxaline (MeIQx), 2-amino-3,4,8-trimethylimidazo(4,5-f)quinoxaline (DiMeIQx)), and one PAH (BaP) using an exposure index described in detail elsewhere (Kazerouni et al, 2001; Sinha et al, 2005a). Correlation coefficients between the DHQ with meat-cooking module and multiple food diaries ranged from 0.31 to 0.46 for chicken, red, and grilled meat intake; and ranged from 0.36 to 0.60 for meat-mutagen intake (Cantwell et al, 2004).
Statistical analysis
A set of sample weights were developed to reduce the potential for bias arising from differential sampling rates for controls and cases, from survey non-response, and from deficiencies in coverage of the population at-risk by the DMV and Medicare files used to select controls (Li et al, 2011). Sample weights for controls also included a post-stratification adjustment, so that the weighted distribution of controls across the matching variables exactly matched the weighted distribution of cases. In addition to being consistent with the objectives of the frequency matching, the post-stratification adjustment reduces the variability of the weights compared to not using this adjustment (Li et al, 2011).
Foods and nutrients were standardised (g per 1000 kcal) for total energy intake, excluding energy from alcohol (non-alcohol energy intake). All continuous exposure variables were categorised into quartiles based on the distributions among controls, with the referent group comprised of individuals in the lowest category of intake. If a variable had a large proportion (e.g., two-thirds to three-quarters) of zero values, then categories were created by setting all zero values to the referent group and categorising the non-zero values into tertiles (as shown in Table 3 for barbecued and broiled meat). To evaluate a wider range of intake and potentially skewed distributions for the meat mutagens (Augustsson et al, 1999; Sinha, 2002), we additionally investigated associations across deciles for BaP, DiMeIQx, MeIQx, and PhIP.
We estimated the risk of developing RCC by deriving adjusted odds ratios (ORs) and 95% confidence intervals (CIs) from unconditional logistic regression models using post-stratified weights. Jackknife replicate weights were created to estimate standard errors (Rust and Rao, 1996). Model covariates (categories defined in Table 1) included study site, age group, self-reported race, sex, education, smoking history as of 2 years before interview, body mass index (BMI, based on height at interview and weight 5 years before interview), history of cancer among first-degree relatives, diagnosis of hypertension 2 or more years before the reference date (self-reported), fruit and vegetable intake (MyPyramid equivalents (Friday and Bowman, 2006); modelled in quartiles), and alcohol intake (quartiles). All models included a continuous covariate for non-alcohol energy intake and were additionally adjusted for other meat variables (e.g., red meat intake adjusted for white meat intake, barbecued meat intake adjusted for intake of meat cooked by other methods, and so on). We also considered potential confounding by other dietary factors, including whole grains and fats, mutual adjustment for meat mutagens (e.g., BaP adjusted for HCAs), as well as energy adjustment, including alcohol intake. We also conducted an unweighted analysis (i.e., not weighting by the post-stratified sample weights) using standard logistic regression procedures, but none of these modifications produced results dissimilar to those presented (data not shown). Tests for trend were performed by creating a continuous variable from the median value for intake in controls within each quartile.
We evaluated effect modification by smoking status, gender, race, BMI, and history of hypertension, by including product terms of the levels of dietary intake (quartiles) and the levels of the factor (i.e., 2 for race and 3 for smoking) in the multiple logistic regression model and testing for the joint significance of the additional terms using the Wald χ2 test that is appropriate for weighted data (Korn and Graubard, 1999). Statistical tests were determined to be significant at a two-sided P<0.05. All analyses were conducted with the SAS software version 9.2 (SAS Institute Inc., Cary, NC, USA) using procedures appropriate for sample-weighted data (SAS Institute, 2008).
Results
Cases tended to be less educated than controls, and they were more likely to be obese, to have a history of hypertension, and to be a current smoker (Table 1). Distributions of demographic and lifestyle characteristics were similar by race (shown in Karami et al, 2010). Intake of red meat, barbecued meat, BaP, and alcohol were significantly higher in cases compared to controls, whereas poultry intake was significantly lower (all Pdiff <0.01; P-values not shown). By race, MeIQx was significantly higher in CA cases compared to CA controls, whereas alcohol, red, and processed meat intake was significantly higher in AA cases compared to AA controls.
Correlations between the mutually exclusive meat-related exposures investigated in the analysis are presented in Table 2. BaP was positively correlated with non-processed red meat (r=0.47) and barbecued meat (r=0.73) intake, whereas HCAs (DiMeIQx, MeIQx, and PhIP) were more strongly correlated with pan-fried meat intake (r=0.55–0.77). In this study population, majority of the BaP and HCA intake (70–90%) came from red meat sources, as compared to white meat sources (data not shown).
In multivariable-adjusted models (Table 3), we found a statistically significant excess risk of RCC for those in the highest, compared to the lowest, intake quartile of barbecued meat and BaP. When mutually adjusted for intake of the HCAs (data not shown), the OR and 95% CI for highest to lowest quartile of BaP was 1.84 (1.37, 2.49). Conversely, high intake of broiled meat, when adjusted for confounders and intake of meat cooked by other methods, was associated with lower risk of RCC. We found no association for pan-fried meat, or for baked, microwaved, and stewed meat (data not shown). Nor did we find associations for any of the HCAs. In addition to the null findings for total, red, and white meat, we found no association for intake of fish (or subgroups of fresh, fried, or canned/salted/smoked), poultry, processed, or fresh red meat (data not shown). Although much of the white meat intake in this population was cooked by methods that do not generate BaP or HCAs (e.g., baking or roasting; see Supplementary Table S1), we observed similar associations for meat mutagens from red vs white meat sources when comparing equivalent levels of intake (OR and 95% CI, per 5 ng per day of BaP intake: 1.01 (1.00–1.02) and 1.02 (0.99–1.05) from red and white meat, respectively). We found a suggestive positive association for ‘smoke-cured red meat’ (sum of bacon, sausage, and pork added to greens), a proxy for processed meats with higher BaP content (Kazerouni et al, 2001; Lee and Shim, 2007; Reinik et al, 2007): covariate-adjusted OR and 95% CI for highest vs lowest quartile (1.24 (0.95, 1.62), data not shown).
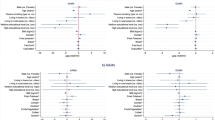
We found a statistically significant interaction by race (Table 4) for BaP (PBaP × race=0.05), as well as for broiled meat intake (Pbroil × race=0.03). For broiled meat, we observed an inverse association for the highest vs lowest quartile of intake among AAs (OR and 95% CI: 0.55 (0.35, 0.85)). Among CA participants, the association with broiled meat was attenuated (OR=0.84, 95% CI=0.62–1.15). In AAs, we observed a significant increase in RCC risk for both the third (1.77 (1.10, 2.83)) and fourth (2.00 (1.15, 3.47)) quartile of BaP intake, respectively. In CAs, an increase in risk (1.42 (1.04, 1.93)) was only detectable in the fourth quartile (median intake, 61 ng per day).
The association between BaP and RCC also differed by smoking status (Table 5; PBaP × smoke=0.02). In the third and fourth quartile of intake (median, 12 and 53 ng per day, respectively), the risk of RCC associated with BaP more than doubled in current-regular smokers. The corresponding risk among never smokers was 1.47 (0.93, 2.31) in the highest, compared to lowest, quartile. We found no evidence of effect modification by smoking status for any of the HCAs (all Pinteraction>0.8) and no other evidence of interaction between meat mutagens, or for any of the other meat exposures with race, gender, BMI, history of hypertension, or smoking status. Results did not materially differ in analyses restricted to the primary histomorphological subtype, clear cell RCC (71% of total cases).
Discussion
In this large, population-based case–control study with a detailed diet history and meat-cooking module with photographic aids, we found that estimated intake of BaP from meat, a carcinogen found in the smoke formed during high-temperature cooking such as barbecuing, was associated with a 50% increased risk of RCC in cases compared with controls. In AA participants, BaP was associated with a more than twofold increase in risk, whereas broiled meat intake was inversely associated with RCC. The positive association between BaP and RCC was also more pronounced in current-regular smokers. We did not find any significant associations with RCC across a wide range of HCA intakes.
Experimental evidence suggests that exposure to HCA and PAH metabolites, ingested in the diet and processed by the kidney through the course of metabolism, may be a biologically plausible risk factor for kidney cancer (Adamson et al, 1990; Thorgeirsson et al, 1995; Turteltaub et al, 1997; Shimada et al, 2003; Peters et al, 2004; Marie et al, 2010). The proximal convoluted tubule, where RCC forms in the epithelial lining, may be particularly susceptible to disease owing to its early exposure to toxins in the glomerular filtrate before urinary excretion (Barjorin, 2007). Nevertheless, few epidemiological studies of kidney cancer have evaluated dietary intake of these carcinogenic compounds (De Stefani et al, 1998; Augustsson et al, 1999) and we are the first to report an association for dietary intake of BaP and risk of RCC, as well as differential associations by race and smoking status. In previous epidemiological studies, BaP intake from high-temperature cooked meat has been associated with cancers of the colorectum (Gunter et al, 2005; Sinha et al, 2005b), pancreas (Anderson et al, 2005; Li et al, 2007), and lung (Lam et al, 2009). A small case–control study in Uruguay reported that barbecued meat and HCA intakes were associated with a significant increased risk of RCC (De Stefani et al, 1998). A larger, multicentre, international case–control study of RCC (Wolk et al, 1996) reported similar findings for ‘well done or charred’ usual degree of meat doneness (proxy for HCAs and/or PAHs). Two case–control studies (Wolk et al, 1996; Lindblad et al, 1997) reported a positive association for meat that was fried or sautéed, a general proxy for HCAs. Similar to our null results for pan-fried meat and HCAs, a Swedish population-based case–control study also found no association between HCAs and kidney cancer, but postulated that this may be due to low exposure or narrow range of intake (Augustsson et al, 1999). We examined more extreme levels (10th and 90th percentiles) of HCA intake and still did not find an association.
Racial differences in cooking practices, such as a well-done meat preference and thus greater exposure to HCAs among AA, have been documented (Bogen and Keating, 2001; Keating and Bogen, 2004). Although in our population AAs consumed greater amounts of pan-fried meat and HCAs than CA participants, we found no association with risk of RCC in either race. Differential findings for BaP by race do not appear to be explained by differences in overall intake, but we cannot rule out the possibility of residual confounding by other divergent risk factors in AA and CA participants. There is some evidence that genetic mutations in the CYP1A1 gene are more common in AAs (Crofts et al, 1993; Nock et al, 2007), whose product, aromatic hydrocarbon hydroxylase, catalyses the first step in the conversion of BaP to a DNA-binding carcinogen. Additional research in diverse populations is needed to clarify these findings.
In addition to dietary sources (Rothman et al, 1993; Kazerouni et al, 2001), inhalation of cigarette smoke, air pollution, and occupational exposures to combustion by-products may also contribute to BaP exposure (Butler et al, 1993; Alexandrov et al, 2010; Golka et al, 2004). As cigarette smoke contains BaP (Ding et al, 2005) and smoking is a known risk factor for kidney cancer (Chow et al, 2010), we also investigated whether smoking status modified the association between RCC and dietary intake of BaP from cooked meat. We found more pronounced risk at lower levels of intake among current-regular smokers compared to never smokers. The effect of smoking may be additive, that is, BaP in cigarette smoke plus dietary intake from meat results in higher overall BaP exposure and thus higher risk, and/or smoking may increase the formation of DNA adducts through upregulated conversion of BaP to benzo(a)pyrene-7,8-diol-9,10-epoxide via cytochrome P450 enzymes (Rubin, 2001; Alexandrov et al, 2010). In the general non-smoking population without substantial exposure to occupational hazards and severe pollution, the diet is likely to be the largest source of BaP exposure (i.e., approximately 70–96% of total exposure in non-smokers) (Lioy and Greenberg, 1990; Menzie et al, 1992; Butler et al, 1993).
Consistent with the current epidemiological literature for meat and RCC (Lee et al, 2008; Alexander and Cushing, 2009), we found no association for total meat or any individual meat types across our study population; thus, it appears that the cooking method, rather than overall meat intake, may be important. Oven-broiling generally results in the formation of little or no meat-cooking compounds (Kazerouni et al, 2001; Sinha, 2002), and in our population was associated with lower risk of RCC in AAs, as well as inversely correlated with barbecued meat intake. In a similar investigation of meat-cooking exposures and colorectal neoplasia, broiled meat intake appeared protective, whereas intake of barbecued meat and BaP was associated with higher risk (Gunter et al, 2005). In our study, intake of ‘smoke-cured’ meat, which is expected to contribute to BaP intake (Garcia Falcon et al, 1999; Kazerouni et al, 2001; Lee and Shim, 2007; Reinik et al, 2007), also showed a suggestive positive association with RCC. Red and processed meat may also be a source of N-nitroso compounds (Joosen et al, 2009), which have been shown to induce renal tumours in rodent models (Hard, 1998). Detailed analyses of these compounds, which are also found in plant foods and drinking water, are ongoing.
The interviewer-administered DHQ with meat-cooking module (Cantwell et al, 2004; Sinha et al, 2005a) was a strength of our study. Although we cannot rule out the possibility of measurement error, photographic aids were used in this study to help the participant select a level of doneness on an incremental scale. Other studies have asked participants to recall the usual appearance of cooked meat without a visual or objective reference and/or did not measure BaP. Additional strengths of our study include a wide range of intake (possibly due to the diversity of our sample), histologically confirmed RCC cases, a relatively large sample size, and adjustment for a multitude of potential confounders, including self-reported history of hypertension, BMI, and smoking status. On the other hand, data collection in this study was based entirely on self-report, and thus subject to recall bias, interviewer bias, differential reporting among cases and controls, and/or non-differential misclassification. However, given the lack of well-established dietary risk factors for RCC and the use of computer-based, structured questionnaires by trained interviewers, it is unlikely that differential recall or interviewer bias had a strong impact on our findings. We did not have the means to calculate relevant BaP intake from other foods for this population; thus, we might have underestimated and/or misclassified categories of BaP from diet in both cases and controls. Other limitations of population-based studies also apply, including selection and non-response bias, which may affect the internal and external validity of our findings. The creation of sample weights using demographic data from both respondents and non-respondents and use of weighted analytic procedures aims to reduce biases arising from low response rates among controls and differential non-response among subgroups (age, sex, race, residence) (Li et al, 2011). We cannot rule out the possibility of chance findings due to multiple comparisons. Statistically significant findings close to the nominal level (α=0.05) should be viewed with caution.
BaP, a PAH found in barbecued meat, was associated with higher risk of RCC. Beyond in vivo and animal experimental evidence, findings from occupational and environmental health studies for PAHs and cancer risk (Butler et al, 1993; Mandel et al, 1995; Pesch et al, 2000; Spinelli et al, 2006) combined with epidemiological findings for dietary BaP from meat and other cancers (Anderson et al, 2005; Sinha et al, 2005b) lend further plausibility to our results. Our findings will require replication in future studies, particularly in diet and cancer studies of prospective design with adequate assessment of meat-cooking methods. In light of our varied findings by race and smoking status, it would be useful to integrate urinary biomarkers of BaP and other PAH metabolites (Peters et al, 2004; Campo et al, 2009; Hecht et al, 2010) into aetiological studies of RCC.
Change history
29 March 2012
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Adamson RH, Snyderwine EG, Thorgeirsson UP, Schut HA, Turesky RJ, Thorgeirsson SS, Takayama S, Sugimura T (1990) Metabolic processing and carcinogenicity of heterocyclic amines in nonhuman primates. Princess Takamatsu Symp 21: 289–301
Alaejos MS, Gonzalez V, Afonso AM (2008) Exposure to heterocyclic aromatic amines from the consumption of cooked red meat and its effect on human cancer risk: a review. Food Addit Contam Part A 25: 2–24
Alexander DD, Cushing CA (2009) Quantitative assessment of red meat or processed meat consumption and kidney cancer. Cancer Detect Prev 32: 340–351
Alexandrov K, Rojas M, Satarug S (2010) The critical DNA damage by benzo(a)pyrene in lung tissues of smokers and approaches to preventing its formation. Toxicol Lett 198: 63–68
Anderson KE, Kadlubar FF, Kulldorff M, Harnack L, Gross M, Lang NP, Barber C, Rothman N, Sinha R (2005) Dietary intake of heterocyclic amines and benzo(a)pyrene: associations with pancreatic cancer. Cancer Epidemiol Biomarkers Prev 14: 2261–2265
Augustsson K, Skog K, Jagerstad M, Dickman PW, Steineck G (1999) Dietary heterocyclic amines and cancer of the colon, rectum, bladder, and kidney: a population-based study. Lancet 353: 703–707
Aune D, De Stefani E, Ronco A, Boffetta P, Deneo-Pellegrini H, Acosta G, Mendilaharsu M (2009) Meat consumption and cancer risk: a case–control study in Uruguay. Asian Pac J Cancer Prev 10: 429–436
Barjorin D (2007) Tumors of the kidney, bladder, ureters, and renal pelvis. In Cecil Medicine, Goldman L, Ausiello D (eds) Saunders Elsevier: Philadelphia, PA
Bogen KT, Keating GA (2001) US dietary exposures to heterocyclic amines. J Expo Anal Environ Epidemiol 11: 155–168
Butler JP, Post GB, Lioy PJ, Waldman JM, Greenberg A (1993) Assessment of carcinogenic risk from personal exposure to benzo(a)pyrene in the Total Human Environmental Exposure Study (THEES). Air Waste 43: 970–977
Campo L, Mercadante R, Rossella F, Fustinoni S (2009) Quantification of 13 priority polycyclic aromatic hydrocarbons in human urine by headspace solid-phase microextraction gas chromatography-isotope dilution mass spectrometry. Anal Chim Acta 631: 196–205
Cantwell M, Mittl B, Curtin J, Carroll R, Potischman N, Caporaso N, Sinha R (2004) Relative validity of a food frequency questionnaire with a meat-cooking and heterocyclic amine module. Cancer Epidemiol Biomarkers Prev 13: 293–298
Chow WH, Dong LM, Devesa SS (2010) Epidemiology and risk factors for kidney cancer. Nat Rev Urol 7: 245–257
Crofts F, Cosma GN, Currie D, Taioli E, Toniolo P, Garte SJ (1993) A novel CYP1A1 gene polymorphism in African-Americans. Carcinogenesis 14: 1729–1731
Cross AJ, Ferrucci LM, Risch A, Graubard BI, Ward MH, Park Y, Hollenbeck AR, Schatzkin A, Sinha R (2010) A large prospective study of meat consumption and colorectal cancer risk: an investigation of potential mechanisms underlying this association. Cancer Res 70: 2406–2414
Cross AJ, Peters U, Kirsh VA, Andriole GL, Reding D, Hayes RB, Sinha R (2005) A prospective study of meat and meat mutagens and prostate cancer risk. Cancer Res 65: 11779–11784
De Stefani E, Fierro L, Mendilaharsu M, Ronco A, Larrinaga MT, Balbi JC, Alonso S, Deneo-Pellegrini H (1998) Meat intake, ‘mate’ drinking and renal cell cancer in Uruguay: a case–control study. Br J Cancer 78: 1239–1243
DiGaetano R, Severynse J, Graubard B, Rao S, Wacholder S (2003) Sampling racially matched population controls for case–control studies: using geocoding of address list frames to establish strata for oversampling minorities. Federal Committee on Statistical Methodology Research Conference
Ding YS, Trommel JS, Yan XJ, Ashley D, Watson CH (2005) Determination of 14 polycyclic aromatic hydrocarbons in mainstream smoke from domestic cigarettes. Environ Sci Technol 39: 471–478
Dolwick Grieb SM, Theis RP, Burr D, Benardot D, Siddiqui T, Asal NR (2009) Food groups and renal cell carcinoma: results from a case–control study. J Am Diet Assoc 109: 656–667
Faramawi M, Johnson E, Fry M, Sall M, Yi Z (2007) Consumption of different types of meat and the risk of renal cancer: meta-analysis of case–control studies. Cancer Causes Control 18: 125–133
Friday JE, Bowman SA (2006) MyPyramid Equivalents Database for USDA Survey Food Codes, 1994–2002 Version 1.0 [Online]. USDA, ARS, Community Nutrition Research Group: Beltsville, MD
Garcia Falcon MS, Gonzalez Amigo S, Lage Yusty MA, Simal Lozano J (1999) Determination of benzo[a]pyrene in some Spanish commercial smoked products by HPLC-FL. Food Addit Contam 16: 9–14
Golka K, Wiese A, Assennato G, Bolt HM (2004) Occupational exposure and urological cancer. World J Urol 21: 382–391
Gunter MJ, Probst-Hensch NM, Cortessis VK, Kulldorff M, Haile RW, Sinha R (2005) Meat intake, cooking-related mutagens and risk of colorectal adenoma in a sigmoidoscopy-based case–control study. Carcinogenesis 26: 637–642
Hard GC (1998) Mechanisms of chemically induced renal carcinogenesis in the laboratory rodent. Toxicol Pathol 26: 104–112
Hecht SS, Carmella SG, Villalta PW, Hochalter JB (2010) Analysis of phenanthrene and benzo[a]pyrene tetraol enantiomers in human urine: relevance to the bay region diol epoxide hypothesis of benzo[a]pyrene carcinogenesis and to biomarker studies. Chem Res Toxicol 23: 900–908
Jemal A, Siegel R, Xu J, Ward E (2010) Cancer statistics, 2010. CA Cancer J Clin 60: 277–300
Joosen AMCP, Kuhnle GGC, Aspinall SM, Barrow TM, Lecommandeur E, Azqueta A, Collins AR, Bingham SA (2009) Effect of processed and red meat on endogenous nitrosation and DNA damage. Carcinogenesis 30: 1402–1407
Karami S, Schwartz K, Purdue MP, Davis FG, Ruterbusch JJ, Munuo SS, Wacholder S, Graubard BI, Colt JS, Chow WH (2010) Family history of cancer and renal cell cancer risk in Caucasians and African Americans. Br J Cancer 102: 1676–1680
Kazerouni N, Sinha R, Hsu CH, Greenberg A, Rothman N (2001) Analysis of 200 food items for benzo[a]pyrene and estimation of its intake in an epidemiologic study. Food Chem Toxicol 39: 423–436
Keating GA, Bogen KT (2004) Estimates of heterocyclic amine intake in the US population. J Chromatogr B 802: 127–133
Korn E, Graubard B (1999) Analysis of Health Surveys. Wiley: New York, NY
Lam TK, Cross AJ, Consonni D, Randi G, Bagnardi V, Bertazzi PA, Caporaso NE, Sinha R, Subar AF, Landi MT (2009) Intakes of red meat, processed meat, and meat mutagens increase lung cancer risk. Cancer Res 69: 932–939
Lee BM, Shim GA (2007) Dietary exposure estimation of benzo[a]pyrene and cancer risk assessment. J Toxicol Environ Health Part A 70: 1391–1394
Lee JE, Giovannucci E, Smith-Warner SA, Spiegelman D, Willett WC, Curhan GC (2006) Intakes of fruits, vegetables, vitamins A, C, and E, and carotenoids and risk of renal cell cancer. Cancer Epidemiol Biomarkers Prev 15: 2445–2452
Lee JE, Spiegelman D, Hunter DJ, Albanes D, Bernstein L, van den Brandt PA, Buring JE, Cho E, English DR, Freudenheim JL, Giles GG, Graham S, Horn-Ross PL, Hakansson N, Leitzmann MF, Mannisto S, McCullough ML, Miller AB, Parker AS, Rohan TE, Schatzkin A, Schouten LJ, Sweeney C, Willett WC, Wolk A, Zhang SM, Smith-Warner SA (2008) Fat, protein, and meat consumption and renal cell cancer risk: a pooled analysis of 13 prospective studies. J Natl Cancer Inst 100: 1695–1706
Li D, Day RS, Bondy ML, Sinha R, Nguyen NT, Evans DB, Abbruzzese JL, Hassan MM (2007) Dietary mutagen exposure and risk of pancreatic cancer. Cancer Epidemiol Biomarkers Prev 16: 655–661
Li Y, Graubard BI, DiGaetano R (2011) Weighting methods for population-based case–control studies with complex sampling. J R Statist Soc Ser C 60: 165–185
Lindblad P, Wolk A, Bergstrom R, Adami HO (1997) Diet and risk of renal cell cancer: a population-based case–control study. Cancer Epidemiol Biomarkers Prev 6: 215–223
Lioy PJ, Greenberg A (1990) Factors associated with human exposures to polycyclic aromatic hydrocarbons. Toxicol Ind Health 6: 209–223
Mandel JS, McLaughlin JK, Schlehofer B, Mellemgaard A, Helmert U, Lindblad P, McCredie M, Adami HO (1995) International renal-cell cancer study. IV. Occupation. Int J Cancer 61: 601–605
Mares-Perlman JA, Klein BE, Klein R, Ritter LL, Fisher MR, Freudenheim JL (1993) A Diet History Questionnaire ranks nutrient intakes in middle-aged and older men and women similarly to multiple food records. J Nutr 123: 489–501
Marie C, Bouchard M, Heredia-Ortiz R, Viau C, Maître A (2010) A toxicokinetic study to elucidate 3-hydroxybenzo(a)pyrene atypical urinary excretion profile following intravenous injection of benzo(a)pyrene in rats. J Appl Toxicol 30: 402–410
Menzie CA, Potocki B, Santodonato J (1992) Exposure to carcinogenic PAHs in the environment. Environ Sci Technol 26: 1278–1284
Mignone LI, Giovannucci E, Newcomb PA, Titus-Ernstoff L, Trentham-Dietz A, Hampton JM, Orav EJ, Willett WC, Egan KM (2009) Meat consumption, heterocyclic amines, NAT2, and the risk of breast cancer. Nutr Cancer 61: 36–46
Nagao M, Sugimura T (1993) Carcinogenic factors in food with relevance to colon cancer development. Mutat Res/Fund Mol Mech Mutagen 290: 43–51
Nock NL, Tang D, Rundle A, Neslund-Dudas C, Savera AT, Bock CH, Monaghan KG, Koprowski A, Mitrache N, Yang JJ, Rybicki BA (2007) Associations between smoking, polymorphisms in polycyclic aromatic hydrocarbon (PAH) metabolism and conjugation genes and PAH–DNA adducts in prostate tumors differ by race. Cancer Epidemiol Biomarkers Prev 16: 1236–1245
Pesch B, Haerting J, Ranft U, Klimpel A, Oelschlagel B, Schill W (2000) Occupational risk factors for renal cell carcinoma: agent-specific results from a case–control study in Germany. MURC Study Group. Multicenter urothelial and renal cancer study. Int J Epidemiol 29: 1014–1024
Peters U, Sinha R, Bell DA, Rothman N, Grant DJ, Watson MA, Kulldorff M, Brooks LR, Warren SH, DeMarini DM (2004) Urinary mutagenesis and fried red meat intake: influence of cooking temperature, phenotype, and genotype of metabolizing enzymes in a controlled feeding study. Environ Mol Mutagen 43: 53–74
Phillips DH (1999) Polycyclic aromatic hydrocarbons in the diet. Mutat Res 443: 139–147
Rashidkhani B, Lindblad P, Wolk A (2005) Fruits, vegetables and risk of renal cell carcinoma: a prospective study of Swedish women. Int J Cancer 113: 451–455
Reinik M, Tamme T, Roasto M, Juhkam K, Tenno T, Kiis A (2007) Polycyclic aromatic hydrocarbons (PAHs) in meat products and estimated PAH intake by children and the general population in Estonia. Food Addit Contam 24: 429–437
Rothman N, Poirier MC, Haas RA, Correa-Villasenor A, Ford P, Hansen JA, O’Toole T, Strickland PT (1993) Association of PAH–DNA adducts in peripheral white blood cells with dietary exposure to polyaromatic hydrocarbons. Environ Health Perspect 99: 265–267
Rubin H (2001) Synergistic mechanisms in carcinogenesis by polycyclic aromatic hydrocarbons and by tobacco smoke: a bio-historical perspective with updates. Carcinogenesis 22: 1903–1930
Rust KF, Rao JN (1996) Variance estimation for complex surveys using replication techniques. Stat Methods Med Res 5: 283–310
SAS Institute (2008) What's New in SAS 9.2. SAS Institute Inc.: Cary, NC
Shimada T, Sugie A, Shindo M, Nakajima T, Azuma E, Hashimoto M, Inoue K (2003) Tissue-specific induction of cytochromes P450 1A1 and 1B1 by polycyclic aromatic hydrocarbons and polychlorinated biphenyls in engineered C57BL/6J mice of arylhydrocarbon receptor gene. Toxicol Appl Pharmacol 187: 1–10
Sinha R (2002) An epidemiologic approach to studying heterocyclic amines. Mutat Res/Fund Mol Mech Mutagen 506–507: 197–204
Sinha R, Cross A, Curtin J, Zimmerman T, McNutt S, Risch A, Holden J (2005a) Development of a food frequency questionnaire module and databases for compounds in cooked and processed meats. Mol Nutr Food Res 49: 648–655
Sinha R, Gustafson DR, Kulldorff M, Wen WQ, Cerhan JR, Zheng W (2000) 2-Amino-1-methyl-6-phenylimidazo[4,5-b]pyridine, a carcinogen in high-temperature-cooked meat, and breast cancer risk. J Natl Cancer Inst 92: 1352–1354
Sinha R, Kulldorff M, Gunter MJ, Strickland P, Rothman N (2005b) Dietary benzo[a]pyrene intake and risk of colorectal adenoma. Cancer Epidemiol Biomarkers Prev 14: 2030–2034
Sinha R, Norat T (2002) Meat cooking and cancer risk. IARC Sci Publ 156: 181–186
Sinha R, Rothman N (1997) Exposure assessment of heterocyclic amines (HCAs) in epidemiologic studies. Mutat Res 376: 195–202
Sinha R, Rothman N, Salmon CP, Knize MG, Brown ED, Swanson CA, Rhodes D, Rossi S, Felton JS, Levander OA (1998) Heterocyclic amine content in beef cooked by different methods to varying degrees of doneness and gravy made from meat drippings. Food Chem Toxicol 36: 279–287
Spinelli JJ, Demers PA, Le ND, Friesen MD, Lorenzi MF, Fang R, Gallagher RP (2006) Cancer risk in aluminum reduction plant workers (Canada). Cancer Causes Control 17: 939–948
Stolzenberg-Solomon RZ, Cross AJ, Silverman DT, Schairer C, Thompson FE, Kipnis V, Subar AF, Hollenbeck A, Schatzkin A, Sinha R (2007) Meat and meat-mutagen intake and pancreatic cancer risk in the NIH-AARP cohort. Cancer Epidemiol Biomarkers Prev 16: 2664–2675
Subar AF, Midthune D, Kulldorff M, Brown CC, Thompson FE, Kipnis V, Schatzkin A (2000) Evaluation of alternative approaches to assign nutrient values to food groups in food frequency questionnaires. Am J Epidemiol 152: 279–286
Subar AF, Thompson FE, Kipnis V, Midthune D, Hurwitz P, McNutt S, McIntosh A, Rosenfeld S (2001) Comparative validation of the Block, Willett, and National Cancer Institute food frequency questionnaires: the Eating at America's Table Study. Am J Epidemiol 154: 1089–1099
Tasevska N, Cross AJ, Dodd KW, Ziegler RG, Caporaso NE, Sinha R, Team PP (2010) No effect of meat, meat cooking preferences, meat mutagens or heme iron on lung cancer risk in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial. Int J Cancer 128: 402–411
Tasevska N, Sinha R, Kipnis V, Subar AF, Leitzmann MF, Hollenbeck AR, Caporaso NE, Schatzkin A, Cross AJ (2009) A prospective study of meat, cooking methods, meat mutagens, heme iron, and lung cancer risks. Am J Clin Nutr 89: 1884–1894
Thorgeirsson SS, Davis CD, Schut HA, Adamson RH, Snyderwine EG (1995) Possible relationship between tissue distribution of DNA adducts and genotoxicity of food-derived heterocyclic amines. Princess Takamatsu Symp 23: 85–92
Turteltaub KW, Mauthe RJ, Dingley KH, Vogel JS, Frantz CE, Garner RC, Shen N (1997) MeIQx–DNA adduct formation in rodent and human tissues at low doses. Mutat Res/Fundam Mol Mech Mutagen 376: 243–252
USDA (2008) Food and Nutrient Database for Dietary Studies, 3.0. US Department of Agriculture, Agricultural Research Service, Food Surveys Research Group: Beltsville, MD
Willett WC (ed.) (1998) Recall of remote diet (Chapter 7). In Nutritional Epidemiology, pp 149–166. Oxford University Press: New York, NY
Wolk A, Gridley G, Niwa S, Lindblad P, McCredie M, Mellemgaard A, Mandel JS, Wahrendorf J, McLaughlin JK, Adami HO (1996) International renal cell cancer study. VII. Role of diet. Int J Cancer 65: 67–73
World Cancer Research Fund/American Institute for Cancer Research (2007) Food, Nutrition, Physical Activity, and the Prevention of Cancer: a Global Perspective. AICR: Washington, DC
Wu K, Sinha R, Holmes MD, Giovannucci E, Willett W, Cho E (2010) Meat mutagens and breast cancer in postmenopausal women – a cohort analysis. Cancer Epidemiol Biomarkers Prev 19: 1301–1310
Acknowledgements
We would like to thank Gloria Gridley, formerly of NCI's Division of Cancer Epidemiology and Genetics, for her substantial contributions to the design of the dietary questionnaire and development of the nutrient variables, and Adam Risch of Information Management Services Inc. for his technical support in computing the dietary nutrient variables. We wish to express our deep gratitude to the residents of Chicago and Detroit who participated in this study. This research was supported by the Intramural Research Program of the NIH, National Cancer Institute.
Author information
Authors and Affiliations
Corresponding author
Additional information
This work is published under the standard license to publish agreement. After 12 months the work will become freely available and the license terms will switch to a Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License.
Supplementary Information accompanies the paper on British Journal of Cancer website
Supplementary information
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Daniel, C., Schwartz, K., Colt, J. et al. Meat-cooking mutagens and risk of renal cell carcinoma. Br J Cancer 105, 1096–1104 (2011). https://doi.org/10.1038/bjc.2011.343
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bjc.2011.343
Keywords
This article is cited by
-
Current innovative approaches in reducing polycyclic aromatic hydrocarbons (PAHs) in processed meat and meat products
Chemical and Biological Technologies in Agriculture (2023)
-
Effect of smoking, hypertension and lifestyle factors on kidney cancer — perspectives for prevention and screening programmes
Nature Reviews Urology (2023)
-
Associations of exposure to polycyclic aromatic hydrocarbons and kidney stones in U.S. general population: results from the National Health and Nutrition Examination Survey 2007–2016
World Journal of Urology (2022)
-
Barbecued desi chicken: an investigation on the impact of polluted milieu upon formation and ingestion of polycyclic aromatic hydrocarbons (PAHs) in commercial versus laboratory barbecued organs along with stochastic cancer risk assessments in people from an industrial district of Punjab, Pakistan
Environmental Science and Pollution Research (2021)
-
The RPTEC/TERT1 Cell Line as an Improved Tool for In Vitro Nephrotoxicity Assessments
Biological Trace Element Research (2015)
