
On completion of this CPD paper, the participant should achieve the following:

-
Discuss the rationale for a comprehensive approach to dental patient examination
-
Enhanced working knowledge of head and neck anatomy
-
Discuss current risk factors for oral cancer
-
Enhanced awareness of the most common sites for oral cancer
-
Identify oral lesions of concern and accurately describe and document them
-
Knowledge of the appropriate action to take if a lesion is found
-
Educate your patients in self-examination techniques.
Introduction
Oral cancer kills one person every hour,1 and oral cancer malpractice claims against dental professionals are increasing. With the increasing incidence of oral and oropharyngeal cancers due to changing risk factors, the role of the dental professional must go beyond examination of the dentition and periodontium. We also need to examine the head and neck, and all of the oral tissues. Early detection and treatment of oral cancer is crucial, as progression is rapid in the oral tissues due to the rich blood supply to the head and neck. Our goal is to discover oral cancers early, before patients present with symptoms.
Risk factors for oral cancer, and oro-pharyngeal cancer:2
-
Historically that has been males over 50, who have used tobacco or are heavy alcohol users. Tobacco use is associated with about 75% of oral cancer cases
-
When an individual is both a heavy smoker and drinker, the risk is greatly increased compared to a heavy smoker, or a heavy drinker alone
-
Patients are at a higher risk for oral squamous cell carcinoma after stem cell transplantation, this is related to immune suppression, and oral graft versus host disease
-
In some Asian cultures chewing betel paan is known to be a strong risk factor for developing oral cancer
-
Research also suggests that a diet low in fruit and vegetables could be a risk factor
-
A slightly higher rate of squamous cell carcinoma (0.2%-3.3%) has been found in patients who have oral lichen planus, in particular the atrophic, plaque and erosive forms (the non-reticular varieties)
-
Sunlight exposure is a risk factor for lip cancer, especially the lower lip.
Changing risk factors
Infection with the human papilloma virus (HPV), particularly types 16 and 18, is a known risk factor and independent causative factor for oral cancer.3 Non-smoking patients between 20 and 50 years old are the fastest growing segment of the oral cancer population: recent research indicates that HPV is the primary risk factor in this new population of oral cancer victims. Between 1988 and 2004, the incidence of HPV-related oropharyngeal cancers increased 225%.4
With early diagnosis the five year survival rates for oral cancer can be 80-90%.5 Unfortunately, five year survival rates have generally remained at about 56%, due to late diagnosis. In the USA, 66% of all oral cancers are being diagnosed at stage III or IV.6
Common sites
Seventy-five percent of all head and neck cancers begin in the oral cavity (Figs 1-4). According to the National Cancer Institute's Surveillance, Epidemiology, and Ends Results (SEER) programme in the USA, 30% of oral cancers originate in the tongue, 17% in the lip, and 14% in the floor of the mouth. Oropharyngeal cancer related to HPV mostly occurs on the tonsil and tonsillar pillars, base of the tongue, and the oropharynx.

Examples of squamous cell carcinoma Images courtesy of Dr Fayette Williams DDS MD
Types of oral cancer
Around 90% of oral cancers are squamous cell carcinomas (SCC).
Rare forms of oral cancer include oral malignant melanoma, mucoepidermoid carcinoma, and adenoid cystic carcinoma.
Stages used to describe cancer of the lip and oral cavity:
Stage I The cancer is less than 2 cm in size, and has not spread to lymph nodes in the area.
Stage II The cancer is between 2-4 cm in size, and has not spread to lymph nodes in the area.
Stage III Either of the following:
-
The cancer is more than 4 cm in size
-
The cancer is any size but has spread to only one lymph node on the same side of the neck as the cancer. The lymph node that contains cancer measures less than 3 cm.
Stage IV Any of the following may be true:
-
The cancer has spread to tissues around the lip and oral cavity. The lymph nodes in the area may or may not contain cancer
-
The cancer is any size and has spread to more than one lymph node, or to any lymph node that measures more than 6 cm
-
The cancer has spread to other parts of the body.
Recurrent disease means that the cancer has recurred after it has been treated. It may recur in the lip and oral cavity or in another part of the body.
Treatment options
Surgical excision combined with radiation therapy, or with chemotherapy and radiation therapy. Reconstructive surgery is required after removal of advanced tumours (Fig. 5).

Images courtesy of Dr Fayette Williams DDS MD. Dr Williams explains:
‘This is one of the bigger tongue cancers I've seen. Unfortunately many people wait until it's too late to do anything simple. This lady's entire tongue was cancerous and it was eating into her right mandible. I did a total glossectomy, partial mandibulectomy, and bilateral neck dissection. Her cancer was so big that I did a “mandibular swing” to open her mandible up like a book to get access to the base of tongue area down by her larynx. Her tongue was reconstructed with an anterolateral thigh free flap. The skin and muscle from her leg is isolated on a pedicle of the artery and vein that supplies the graft. The vessels are clamped and re-anastomosed to vessels in her neck under a microscope using 9-0 nylon sutures. This is a transplant within her own body so that the new graft is viable and living just like it was at her leg so that it withstands radiation therapy very well.’
The role of the dental hygienist
The dental hygienist plays an important role in the preliminary observation and documentation of oral pathologies. The UK dental hygiene scope of practice includes recognition of oral lesions.7 In North America performing a head and neck and intra-oral examination is the standard of care for the dental hygienist. The American Academy of Periodontology's (AAP) updated position statement summarises the essentials of a comprehensive periodontal evaluation; this includes extraoral and intraoral examinations to detect nonperiodontal oral disease.8
General appraisal
Assessment begins as soon as we greet our patient, before they even sit in our chair. We should observe the following:
-
Gait and posture
-
General appearance and cleanliness
-
Respiration
-
Signs of confusion
-
Changes in voice - hoarse? Nasal?
-
Hands: eg colour of fingertips
-
Facial symmetry, swelling
-
Skin colour and texture
-
Eyes.
The medical history is reviewed for known risk factors for oral cancer, history of cancer, medications, and systemic diseases. Oral cancer screening can be done in less than four minutes.
Examination techniques
Visual inspection, and bimanual, digital, bidigital, and bilateral palpation techniques are used to examine the head and neck and intra-oral tissues for lesions and swelling.
Extra-oral examination of the mandible, parotid gland, thyroid gland, larynx, temporomandibular joint, and the lymph nodes of the head and neck (Fig. 6).

(c)EMIS 2011 as distributed at http://www.patient.co.uk/diagram/Lymph-nodes-head-and-neck.htm, used with permission.
Lymph nodes
-
Pre-auricular (parotid nodes)
-
Post-auricular
-
Occipital
-
Submandibular
-
Submental
-
Posterior and superior cervical
-
Supraclavicular.
11 steps of intra-oral examination
-
1
Lips - vermilion border and commissures
-
2
Labial mucosa and fraenum
-
3
Alveolar ridges, gingiva
-
4
Buccal mucosa, parotid duct
-
5
Retromolar pads
-
6
Maxillary tuberosity
-
7
Tongue - ventral surface (underside), floor of mouth, submandibular and sublingual salivary glands
-
8
Dorsum, base and lateral borders of tongue
-
9
Hard and soft palate
-
10
Uvula, tonsillar pillars
-
11
Tonsils, posterior wall of pharynx.
When a suspicious area is identified, the dental professional needs to determine how long it has been present. If any of the following signs or symptoms persist for more than two weeks, they need to be investigated.9
Oral lesions of concern, and other signs 10
-
Ulcers or other lesions that cannot be related to trauma or infection
-
Leukoplakia (white lesions); this is the most common precancerous lesion, particularly on the floor of the mouth or ventral (under) surface of the tongue
-
Erythroplakia (red lesions) could also be precursors to cancer
-
Erythroleukoplakia (combined red and white lesions). Lesions with a red component have greater potential for becoming cancerous
-
Palatal soft-tissue masses, and mucocele-like lesions in locations other than the lower lip, floor of mouth, or ventral surface of the anterior tongue
-
Lumps or thickening in the oral soft tissues
-
Pigmented lesions
-
Swellings.
Symptoms usually noted in the later stages
-
Difficulty moving the jaw or tongue
-
A sore throat or a feeling that something is caught in the throat
-
Difficulty chewing or swallowing
-
Pain or numbness of the tongue or other area of the mouth (paraesthesia)
-
Chronic hoarseness
-
Swelling of the jaw that causes dentures to fit poorly or become uncomfortable
-
Persistent earache.
Action
-
1
Document and describe the patient's known risk factors, and description of the lesion(s) (Fig. 7). A photograph can also be taken.
-
History: duration, symptoms
-
Location, number of lesions, size, margin configuration (distinct, or irregular)
-
Colour: normal, red, white, yellow, pigmented
-
Surface texture: smooth, hyperkeratinised, ulcerated, erosive, verrucous, or papillary
-
Consistency: firm (indurated) or soft
-
Attachment: broad base, (sessile), on a narrow stalk (pedunculated)
-
Contour: raised (nodular) or flat (macular)
-
Mobility: movable, or fixed.
Figure 7 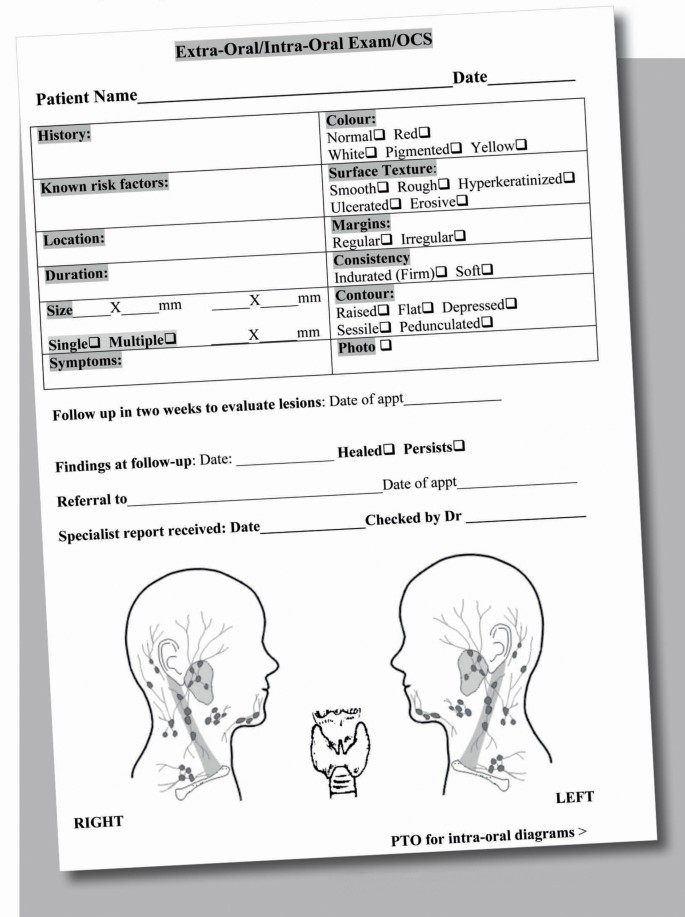
A form to document the findings of oral cancer screening
-
-
2
Evaluate in two weeks: many benign lesions mimic oral cancer.
-
3
If it has healed, document this, and continue with regular oral cancer screenings at recalls.
-
4
If it is still present at the two-week. evaluation, refer to an oral pathologist or oral surgeon for further examination and biopsy.

Self-examination
Oral cancer self-examination is recommended by the American Association of Oral and Maxillofacial Surgeons. Patients should be educated to observe for signs and symptoms between dental visits. They should perform a head and neck and oral self-examination every month.
Conclusion
Because we see our patients quite frequently for regular oral care, dentists and dental care professionals are in a crucial position to make a significant difference in the early detection of oral cancer. We should also educate our patients to be partners in monitoring and maintaining their oral health. Our combined vigilance contributes to timely diagnosis and less disfiguring treatment, with improved survival rates and quality of life for our patients. Make oral cancer screening a routine part of your patient care.
Part 2
In part two of this series, we will discuss adjunctive technologies for oral cancer screening, plus evolving techniques for diagnosis, and treatment of oral cancer.
Useful resources
This self-study course includes an instructional DVD, a mail-in test, and a wall chart demonstrating examination techniques.
YouTube medical school videos of examination techniques. https://www.youtube.com/watch?v=GQe0fwhdrdo
This site has free online CE courses on oral pathology.
Drbicuspid oral cancer and diagnostics insider is an e-newsletter, providing literature on the latest research. https://www.drbicuspid.com/index.aspx?sec=sup&sub=orc
Mouth Cancer Action Month
A month-long campaign dedicated to raising awareness of the disease www.mouthcancer.org
Canadian Dental Hygienists Association Oral Cancer Awareness online course, ‘4 Life Saving Minutes: The Extraoral and Intraoral Examination’, with a demonstration video.
Oral Cancer Foundation http://oralcancerfoundation.org/facts/index.htm
Dr Randy Otterholt's website-download oral pathology forms www.drotterholt.com/downloads.html
What to do if a lesion is found
Dental professionals need to track any lesion or deviation until it disappears. If it persists after two weeks and the diagnosis is unknown, it must be biopsied.
Biopsy is the gold standard for definitive diagnosis of oral lesions.
References
US Government Surveillance, Epidemiology, and End Results (SEER) report on the incidence of oral cancers divided into Age, Sex, Location Etc. http://oralcancerfoundation.org/facts/index.htm
National Institute of Dental and Craniofacial Research. Detecting oral cancer: a guide for health care professionals. http://www.nidcr.nih.gov/OralHealth/Topics/OralCancer/DetectingOralCancer.htm
Fakhry C, Gillison M L . Clinical implications of HPV in head and neck cancers. J Clin Oncol 2006; 24: 2606–2611.
Chaturvedi A K, Engels E A, Anderson W F, Gillison M L . Incidence trends for human papillovirus-related and -unrelated oral squamous cell carcinomas in the United States. J Clin Oncol 2008; 26: 612–619.
Gloeckler Ries L A, Miller B A, Hankey B F, Kosary C L, Harras A, Edwards B K (eds). SEER cancer statistics review, 1973-1991. Bethesda, Md: US Department of Health and Human Services, Public Health Service, National Cancer Institute, 1994. Report no. NIH-94-2789.
Neville B W, Day T A . Oral cancer and precancerous lesions. CA Cancer J Clin 2002; 52: 195–215.
General Dental Council. Standards for dental professionals. http://www.gdc-uk.org/dentalprofessionals/standards
Comprehensive periodontal therapy: a statement by the American Academy of Periodontology. J Periodontol 2011; 82: 943–949.
Koerner K R . Evaluation and treatment by general dentists of oral soft-tissue lesions. Dent Today 2006; 25: 90–95.
Kratochvil J . Oral lesions of concern. pp 8–9. Oregon/SW Washington: Doctor of Dentistry, March 2002.
Rights and permissions
About this article

Cite this article
Douglas, L. Making oral cancer screening a routine part of your patient care Part 1. BDJ Team 1, 15066 (2015). https://doi.org/10.1038/bdjteam.2015.66
Published:
DOI: https://doi.org/10.1038/bdjteam.2015.66
