
Key Points
-
DAA is the most reliable method of assessing the age of children and emerging adults.
-
DAA is widely used by lawyers and immigration officers for international adoptions where the birth date is not known or is unreliable.
-
DAA is achieved using the mathematical techniques of meta-analysis which integrates the known ages from teeth at different tooth developmental stages.
-
The DAA database provides the basis for the computation which can be used by clinicians. Contact any of the authors.
Abstract
Introduction Methods of dental age assessment (DAA) give a wide margin of error and, because third molars are usually excluded, prevent estimation around the age of 18 years. This study extends the use of defined tooth development stages (TDSs) to include third molars.
Subjects and methods Re-use of dental panoramic tomographs (DPTs) and other X-rays taken for clinical use comprised the sample of 1,547 subjects. The radiographic images were then captured in digital format. The TDSs were assessed and the estimated mean age and its standard error were calculated for each TDS. The mathematical technique of meta-analysis was used to provide an estimate of the mean age, with 99% confidence interval, of a new 'test' subject. To assess the accuracy of the method, each of these mean values was then compared with the gold standard of chronological age.
Results On average, estimated dental age (DA) over-estimated chronological age (CA) by 0.29 years, approximately 3½ months. The maximum likely difference between the estimated DA and CA was 1.65 years.
Conclusion Estimation of dental age using well defined TDSs, extended to include third molars and combined with the statistical technique of meta-analysis, provides investigators with a rapid and accurate estimation of age.
Similar content being viewed by others


Introduction
Background
Assessment of tooth development to estimate the age of living subjects has a long history. In industrial sociology, the presence of the first permanent molar was a sign that a child had attained six years of age and such children were condemned to working in the coal mines of the 19th century industrial revolution in England.1 Tooth eruption is still a guide to a child's age both in social and clinical contexts.2 Recently, tooth development data from radiographs have been used in the estimation of the biological age of children adopted from overseas where there is unreliable, or nonexistent documentation of the birth date. In addition, an increasingly common request is to assess the age of young asylum seekers deemed to be over 18 years of age by the Immigration Bureau of the United Kingdom. The estimated dental age (DA) of an individual, obtained from the stages of dental development present in the individual, is taken as the estimate of chronological age (CA).
The availability of X-rays has facilitated visualisation of identifiable development stages of dental maturity for each tooth.3 Radiological methodology was further improved with the development of dental panoramic tomographs (DPTs) which give reasonably good images of all the teeth, especially the lowers, both erupted and unerupted. This was an important step forward as it enabled clinicians to grade the development of each of the 16 tooth morphology types (TMTs) into one of a number of easily recognisable and clearly defined tooth development stages (TDSs).4 It was possible to provide summary data such as the mean and standard deviation and range of age values for each tooth stage. However, a shortcoming of many of the papers was the lack of clarity of the precise method for arriving at the dental age of the subject. The main exception to this was the detailed and systematic work carried out in Canada.5
Tooth development stages
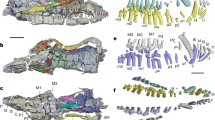
The radiographic appearance of the development of each tooth follows a regular pattern (Fig. 1). The first problem is to decide on the number of stages of development to be used for DAA. The number of stages varies between 4 and 32 stages.4,5,6,7,8,9,10,11,12,13 On practical grounds, choice of the number of stages is a compromise between using a small number of stages that are easily identified and using a large number of stages that are less reliable. A more precise estimate of DA should be obtained by using a larger number of stages but, because of the difficulty of identifying them reliably, the precision of the estimate will be reduced and the age assessment may be less accurate than if a smaller number of stages is used. An acceptable compromise appears to be the eight stage system described by Demirjian.5 Investigation of reproducibility has shown that the eight stage system gives reliable inter-rater agreement for all TDSs.14,15 Only the first part of the Demirjian technique5 viz the descriptions of the TDSs and the application of this approach to the teeth in the upper arch as well as the lower arch is used in the present study.

The tooth development stages as described by Demirjian5
Tooth data integration
The important information from each tooth is the age of attainment of each developmental stage (Fig. 1). Preliminary analysis of the data shows that for all stages except H, the age for attainment of any TDS approximately follows a normal distribution. This has the advantage that summary data for each and all of the TDSs present on a radiograph can easily be used to give an estimate of the DA of the subject. To estimate DA, clinicians have looked at the mean age of attainment of each TDS present on an individual's radiograph and 'averaged' them to give the estimated mean DA for that individual. The degree of dispersion of the ages from the database for each TDS has usually been ignored when the overall mean is calculated and so the estimated mean age is imprecise.
The purpose of the present study was to utilise the mathematical techniques of meta-analysis for DAA using the database derived from a multi-ethnic population and to evaluate the accuracy of this method of estimating DA by comparing it to CA which, because of the reliability of birth records, is effectively a gold standard.
Patients, materials and methods
Radiographs
The protocol for the study received ethical approval from the University College Hospitals NHS Trust – reference 03/E023. The data for this study were obtained by re-use of dental panoramic tomographs (DPTs). All subjects were physically healthy; those with conditions that might have affected maturation were excluded. Chronological ages ranged from 1.8 years to 26.1 years. In addition, lateral oblique jaw views and intra-oral radiographs when available, were also used. Radiographs obtained from consecutive patients attending the Eastman Dental Hospital between January 2004 and July 2006 for clinical purposes were examined and, if of good quality, the parents and/or patient were approached and asked if the radiograph could be included in the database for research purposes. A total of 1,547 radiographs were used, and the information obtained from them comprised the database.
Tooth development stages (TDSs)
The assessment of tooth development stages was carried out using the method for TDSs described and defined in 1973.5 The criteria for TDSs were applied to all teeth on the left side of the maxilla and mandible, a total of 16 unique tooth morphology types (TMTs).
Statistical analysis
Inter- and intra-rater agreement of TDSs
A set of 10 randomly chosen DPTs from the database, each with 16 TMTs, was used to assess inter- and intra-rater agreement of the TDSs for all the TMTs. Two raters were used to assess inter-rater agreement; the time interval between the two 'blind' assessments for intra-rater agreement was one week. The degree of agreement was calculated using Cohen's Kappa and assessed according to the categories suggested by Landis and Koch.17
The database
The chronological age and TDS of each TMT for every child in the database was stored in Microsoft Access and was exported to Excel which was used to estimate the mean age and standard error for each TDS; the distribution of the ages for each TDS was tested for normality using the Shapiro Wilk test.18
Meta-analysis for DAA
Meta-analysis is a quantitative procedure that is used in statistical methodology to combine and summarise the results of several studies that address a particular research hypothesis.16 In the context of DAA, the meta-analysis approach provides an estimate of the expected DA in a subject by calculating a weighted mean of the mean ages of the TDSs in that subject, with each weight being proportional to the standard error of the mean age for that TDS. A random effects model has been used for the calculation: it assumes that, in addition to the random variation associated with each TDS estimate, there is heterogenicity among the TDS results and it incorporates this source of variation into the calculation. That is to say that in this study it is the mathematical techniques of meta-analysis that are used, with each TDS analogous to the individual studies used in conventional meta-analysis. The radiograph of an individual test subject, not part of the database, was examined and the TDSs for all developing teeth noted. This excludes all teeth at stage H, which denotes apex closed. For every usable TDS for that subject, the estimated mean age and its standard error (derived from the whole dataset) were copied into Stata and a meta-analysis performed.19 The estimated overall mean age from this analysis, together with its associated upper and lower 99% confidence limits, was used as the DAA for that subject.
Testing the method for accuracy
A consecutive sample of DPT and lateral oblique radiographs was selected. Parents (and patients over 12 years of age) were asked for permission to re-use the X-ray for the study. A total of 50 X-rays, which did not form part of the database, were used as a test dataset. These patients were seen over the four month period from January 2005 to June 2005. Meta-analysis was performed, using the results from the TDSs of teeth that were still developing on each X-ray, to estimate the DA with 99% confidence interval of that subject (Table 1). The patient shown in Figures 2 and 3 and Table 1 provides a worked example for one of the cases used in the 'accuracy' part of the study. Stata was used to evaluate the accuracy of the DA estimation by comparing the DA estimated age for each child to her/his gold standard of CA using the method of Bland and Altman.20 Lin's concordance correlation coefficient, which combines measures of both precision and accuracy to determine how far the observed data deviate from the line of perfect concordance (ie the line through the origin at 45 degrees on a square scatter plot when CA is plotted against DA), was calculated.21

Dental panoramic tomograph of child ID No. 04082523, initials DS. Chronological age = 12.62 years

The combined estimated mean dental age for this subject is indicated by the dotted line and the 99% confidence interval by the horizontal limits of the diamond
Results
The Kappa value for intra-rater agreement for examiner 1 was 0.9024 (almost perfect), for examiner 2 it was 0.8417 (almost perfect) and for inter-rater agreement between examiner 1 and examiner 2 was 0.80829 (substantial).
For the TDS example used (LL8E), the Shapiro Wilk test gave a p-value of 0.08 which indicated that it was reasonable to assume a normal distribution of the ages from the dataset for this TDS. This is a common finding for TDSs in this dataset.22
Figure 2 shows the DPT of a typical child subject, ID No. 04082523, initials DS. Table 1 contains the estimated mean age, with estimated standard error, for each TDS for that subject, and Figure 3 shows the meta-analysis forest plot and results for that subject. The estimated dental age of this child whose CA is 12.62 years is obtained by assigning the DA of 12.66 years as the estimated age with the precision of this estimate given by the 99% confidence interval of 11.96 to 13.36 years.
When assessing the agreement between CA and the estimated DA in the test dataset from 50 children using the Bland and Altman method,20 the differences between CA and the estimated DA were randomly distributed around the mean difference of 0.29 years (SD 0.843 years), with the estimated DA generally greater than CA. A paired t-test performed on these data gave p = 0.04, indicating that there was a suggestion of a systematic difference or bias between the pairs of ages. However, Lin's concordance coefficient was 0.95 (95% confidence interval 0.92-0.97), which is very close to the upper limit of 1.0 when there is perfect concordance.21 The British Standards reproducibility coefficient was approximately equal to 1.96 × (SD of the differences) = 1.96 × 0.843 = 1.65; this indicates that the maximum likely difference between a pair of ages (estimated DA and CA) was approximately 1.7 years.
Discussion
The use of dental development as a method of assessing age is increasingly used in both criminal14 and civil proceedings.23 The close genetic control of dental development means that conditions inhibiting growth and development have only a minimal affect on dental maturation.24,25,26 Thus, developing teeth provide a continuous and steady record of the tempo of accumulated growth from the prenatal onset of tooth mineralisation to the young adult, when the apex of the third permanent molar roots close. All dental age assessment studies on living subjects are designed to tease out this information within the ethical restraints of clinical research.
The exclusion of teeth that have closed apices is at present justified because it is claimed to be impossible to estimate the time when the apex closes.15 The use of meta-analysis is a practical way of calculating the average of the means of all the developing teeth in a single subject. It also provides the lower and upper limits of the 99% confidence interval for the mean (Fig. 3). This approach assumes that the subject who is the object of enquiry has teeth that are growing at an average rate and that the age assessed is that of the average individual. A further difficulty with the present paper is the lack of differentiation between females and males, and between ethnic groups. This will form an important part of ongoing research when factors such as gender, ethnicity and influences on maturation will be explored in detail. The justification for this early publication utilising meta-analysis is the impressive closeness, on average, of the estimated DA to the CA shown in this study. Other investigators are encouraged to repeat and extend this work to determine whether or not there is a general applicability of the method.
In summary, the database with the TDS of each of 16 TMTs of 1,547 subjects of known CA was used to determine the estimated age of an individual subject of unknown birth date by collating the data using the mathematical techniques of meta-analysis. Employing this procedure on a consecutive sample of 50 child subjects, each with the gold standard of verifiable date of birth, on average the dental age (DA) over estimated chronological age (CA) by 0.29 years, approximately 3½ months, although the difference between a child's estimated and chronological age could be as great as 1.65 years. The methodological refinement described in this paper provides greater accuracy for estimating chronological age from tooth development than was possible previously.
References
Saunders E. The teeth a test of age, considered with reference to the factory children: addressed to members of both Houses of Parliament. 1837 ed. pp 1–2. London: H. Renshaw, 1837.
Ekstrand K R, Christiansen J, Christiansen M E C. Time and duration of eruption of first and second permanent molars: a longitudinal investigation. Community Dent Oral Epidemiol 2003; 31: 344–350.
Fanning E A. A longitudinal study of tooth formation and resorption. N Z Dent J 1961; 57: 202–217.
Gustafson G, Koch G. Age estimation up to 16 years of age based on dental development. Proc Finn Dent Soc 1974; 25: 297–306.
Demirjian A, Goldstein H, Tanner J M. A new system of dental age assessment. Hum Biol 1973; 45: 221–227.
Rosen A A, Baumwell J. Chronological development of the dentition of medically indigent children: a new perspective. J Dent Child 1981; 48: 437–442.
Bolanos M V, Moussa H, Manrique M C, Bolanos M J. Radiographic evaluation of third molar development in Spanish children and young people. Forensic Sci Int 2003; 133: 212–219.
Haavikko K. The formation and the alveolar and clinical eruption of the permanent teeth; an orthopantomographic study. Suom Hammaslaak Toim 1970; 66: 104–170.
Demirjian A, Goldstein H. New systems for dental maturity based on seven and four teeth. Ann Hum Biol 1976; 3: 411–412.
Kullman L, Johanson G, Akesson L. Root development of the lower third molar and its relation to chronological age. Swed Dent J 1992; 16: 161–167.
Kullman L. Accuracy of two dental and one skeletal age estimation method in Swedish adolescents. Forensic Sci Int 1995; 75: 225–236.
Willershausen B, Loffler N, Schulze R. Analysis of 1202 orthopantograms to evaluate the potential of forensic age determination based on third molar developmental stages. Eur J Med Res 2001; 6: 377–384.
Gat H, Sarnat H, Bjorvatn K, Dayan D. Dental age evaluation: a new six developmental stage method. Clin Prev Dent 1984; 6: 18–21.
Olze A, Bilang D, Schmidt S et al. Validation of common classification systems for assessing the mineralization of third molars. Int J Legal Med 2004; 119: 22–26.
Maber M, Liversidge H M, Hector M P. Accuracy of age estimation of radiographic methods using developing teeth. Forensic Sci Int 2006; 159S: S86–S73.
Leandro G. Meta-analysis in medical research. Oxford: BMJ Books, Blackwell Publishing, 2005.
Landis J R, Koch G G. The measurement of observer agreement for categorical data. Biometrics 1977; 33: 159–174.
Shapiro S S, Wilk M B. An analysis of variance test for normality (complete samples). Biometrika 1965; 52: 591–611.
Stata corporation. Stata user's guide release 9. (Version 8.0). 2005.
Bland J M, Altman D G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1: 307–310.
Lin L. A concordance correlation coefficient to evaluate reproducibility. Biometrics 1989; 45: 255–268.
Boonpitaksathit J. Development of reference standards for age assessment in Caucasians using third molar development. London: University College London, 2005. MSc Thesis.
Schmeling A, Reisinger W, Loreck D et al. Effects of ethnicity on skeletal maturation: consequences for forensic age estimations. Int J Legal Med 2000; 13: 135–137.
Jaffe E, Roberts G J, Chantler C, Carter J E. Dental maturity in children with chronic renal failure assessed from dental panoramic tomographs. J Int Assoc Dent Child 1990; 20: 54–58.
Shah H, McDonald F, Lucas V S et al. A cephalometric analysis of patients with recessive dystrophic epidermolysis bullosa. Angle Orthod 2002; 72: 55–60.
Kostara A, Roberts G, Gelbier M. Dental maturity in children with dystrophic epidermolysis bullosa. Pediatr Dent 2000; 22: 385–388.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed paper
Rights and permissions
About this article
Cite this article
Roberts, G., Parekh, S., Petrie, A. et al. Dental age assessment (DAA): a simple method for children and emerging adults. Br Dent J 204, E7 (2008). https://doi.org/10.1038/bdj.2008.21
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bdj.2008.21
This article is cited by
-
Deep learning methods for fully automated dental age estimation on orthopantomograms
Clinical Oral Investigations (2024)
-
An automatic methodology for full dentition maturity staging from OPG images using deep learning
Applied Intelligence (2023)
-
Radiographic dental age estimation applying and comparing Demirjian’s seven (1973) and four (1976) teeth methods
Forensic Science, Medicine and Pathology (2023)
-
Ultrasonic bone age fractionates cognitive abilities in adolescence
Scientific Reports (2022)
-
A large sample-sized study on dental development of children treated at the Central Dental Clinic (OCEx) of the Brazilian Army
Clinical Oral Investigations (2022)
