
Abstract
Aim:
To investigate the QT/QTc effects of orally administered moxifloxacin in healthy Chinese volunteers.
Methods:
This was a single-blinded, randomized, single-dose, placebo-controlled, two-period cross-over study. A total of 24 healthy Chinese volunteers were enrolled, randomly assigned to two groups: one group received moxifloxacin (400 mg, po) followed by placebo with a 7-d interval, another group received placebo followed by moxifloxacin with a 7-d interval. On the days of dosing, 12-lead 24 h Holter ECGs were recorded and evaluated by an ECG laboratory blind to the treatments. Blood samples were collected to determine plasma concentrations of moxifloxacin.
Results:
The orally administered moxifloxacin significantly prolonged the mean QTc at all time points except 0.5 h post-dose. The largest time-matched difference in the QTcI was 8.35 ms (90% CI: 5.43, 11.27) at 4 h post-dose. The peak effect on QTcF was 9.35 ms (90% CI: 6.36, 12.34) at 3 h post-dose. A pharmacokinetic-QTc model suggested a 2.084 ms increase in the QTc interval for every 1000 ng/mL increase in plasma concentration of moxifloxacin. In addition, the orally administered moxifloxacin was well tolerated by the subjects.
Conclusion:
Orally administered moxifloxacin significantly prolongs QTc, which supports its use as a positive control in ICH-E14 TQT studies in Chinese volunteers.
Similar content being viewed by others
Introduction
Drugs that block the rapidly activated delayed rectifier potassium current (IKr) and induce a delay in cardiac repolarization may create an electrophysiological environment that favors the development of cardiac arrhythmias, including Torsades de pointes (TdP)1. The recent high-profile non-approvals and withdrawals of newly approved drugs due to adverse cardiac effects, primarily QT prolongation and TdP2, have triggered public concerns, increased regulatory scrutiny and resulted in new guidelines for the pharmaceutical development of new drugs3. The International Conference on Harmonization (ICH) guidelines, topic E14 (ICH-E14)4, is primarily concerned with the investigation of the effect of new drugs on cardiac repolarization by analyzing the QT interval obtained from surface electrocardiography. The highlight of the ICH-E14 guidelines is the requirement for a well-designed, appropriately powered and well-executed 'Thorough QT/QTc (TQT) Study'. These guidelines have been implemented in Europe, the United States and Japan5. However, in China a “thorough” QTc study has not been required for the registration of new drugs, and no relevant TQT studies with Chinese volunteers have been published.
One of the key elements of a TQT study is the need for both placebo and positive controls. The latter serves to ease regulatory concerns of 'assay sensitivity' by demonstrating that the particular study was capable of detecting a QTc prolongation relative to the baseline and placebo. According to the ICH guidelines, the sensitivity target of a TQT study is defined as a mean increase in the QTc interval of approximately 5 ms and an upper limit of 10 ms for the 95% one-sided confidence interval (CI) of the mean QTc effect4. The use of moxifloxacin as a positive control can demonstrate a QTc prolongation at a minimum of one time point with a low one-sided 95% confidence interval greater than 5 ms6. Moxifloxacin is a broad spectrum fluoroquinolone antibiotic with a well-documented and consistent QT prolongation effect7 and a favorable cardiovascular safety profile8, and it has become the positive control of choice for TQT studies.
The primary objective of this study was to investigate the QT/QTc effects of moxifloxacin in healthy Chinese volunteers and relate these effects to previous studies in Caucasian subjects.
Materials and methods
This study was approved by the Independent Ethics Committee (IEC) of Shanghai Xuhui Central Hospital (Approval No 2012-07) and was conducted in accordance with the principles of the Declaration of Helsinki (2008 version), Good Clinical Practice guidelines and other applicable regulatory requirements. All subjects were informed by a clinical investigator of the study aim, procedures, and risks. Every subject gave written informed consent to participate in the study.
Subjects
Subjects were informed of the risks and benefits of the study before enrolement and submitted a written informed consent. Healthy, non-smoking Chinese male volunteers were required to be 18–45 years of age with a body mass index between 18 and 32 kg/m2.
Volunteers were required to have no clinically significant medical history and normal results for blood chemistry, hematology, urinalysis, vital signs and serology for hepatitis and human immunodeficiency virus (HIV). Four weeks prior to the start of the study, volunteers ceased the use of any medications that could interfere with the procedures or interpretation of data or compromise the subject's safety.
Volunteers with a history of additional risk factors for Torsade de pointes, eg, heart failure, hypokalemia, a history or family history of Long QT Syndrome or a QTc interval >450 ms, were not eligible to participate in the trial. Volunteers were excluded if their ECG data met any of the following conditions: PR>200 ms, QRS≥120 ms, QTc≥450 ms, or a resting heart rate <50 bpm or >100 bpm.
Volunteers were instructed to avoid new prescriptions, over-the-counter (OTC) and alternative/complementary medications without advance permission from the principal investigator.
Study drug
This study used the moxifloxacin 400 mg/tablet called Avelox®. It was produced by Bayer in Germany with a batch number of BJ05693. Placebo tablets were prepared by packing edible starch into capsules. Moxifloxacin tablets were repacked in the same capsules to match the appearance and weight of the placebo.
Study design
This was a single-blind, single-dose, randomized, placebo-controlled, two-period crossover study. A statistician provided a computer-generated randomization table. All eligible subjects were assigned randomization numbers and divided into two groups at d −1 in the order of subject registration. One group received placebo followed by moxifloxacin, and another group received moxifloxacin followed by placebo with a 7-d washout. A time-matched baseline (TMB) day (d 1) was included prior to Period 1. There was no untreated baseline day prior to Period 2. The dosing of Period 1 occurred on d 2 and the dosing of Period 2 began on Day 9 with a 7-d washout interval between periods (Table 1). On the TMB day, ECGs were recorded at times that corresponded to the scheduled time point of each dosing day. The Holter recorder was activated exactly 30 min before the planned time points.
Standardized meals were provided 4 and 10 h after dosing (and after any assessments scheduled at the same time point). For each of the treatment periods, the subjects were admitted to the clinical research center the evening prior to the first day of assessments and were discharged from the Clinical Research Unit after completing the 24-h post-dose procedures. For all subjects, blood samples were taken at 15 min pre-dose and at 0.5, 1, 1.5, 2, 2.5, 3, 4, 6, 8, 10, 12, and 24 h post-dose on the dosing day of both periods. Samples were used to determine the plasma concentration of moxifloxacin. During and between the periods, meals, fluid intake and the surrounding environment was kept as controlled and consistent as possible.
ECG recording
Digital 12-lead Holter ECGs were recorded at the Clinical Research Unit (Xu Hui Central Hospital, Shanghai, China) using a H12+ (1000Hz) continuous ECG recorder (Mortara Instrument Inc, Milwaukee, WI, USA). The ECG signal for each 24-h period for each subject was recorded on a high-density compact flash memory card.
The Holter recorder was activated at least 15 min before the planned dose time on d 1. The subjects were asked to rest quietly in a supine position for 15 min before and 5 min after each protocol-defined ECG time point. Measurements were taken at the following time points: 15 min pre-dose and 0.5, 1, 1.5, 2, 2.5, 3, 4, 6, 8, 10, 12, and 24 h post-dose on d 1, d 2, and d 9. A single 12-lead ECG was printed and reviewed by an investigator at 2, 4, 6, and 24 h after dose administration for an evaluation of safety.
ECG analysis and interpretation
The memory cards containing the digital ECG data were sent to the central ECG laboratory (CoreLab Partners Inc, Shanghai, China) for analysis. For each time point, 3 digital 12-lead ECGs were extracted as triplicate ECG records. The 3 ECGs were centered on the nominal time point of the protocol, typically within a 2-min window on either side of the central (nominal) time point. If the targeted ECG time points contained artifacts or were of poor quality, an alternative trace consisting of 10 s of standard 12-lead ECG data was extracted within an extended window of up to 5 min on either side of the nominal time point.
For each 12-lead ECG, three consecutive magnified PQRST complexes and their preceding RR intervals were manually measured on screen using electronic calipers. Measurements were performed from lead V3 (preferred) or lead II (back up), and the same lead was used for each subject wherever possible. ECG interval measurements were performed by a group of physician cardiovascular specialists (CoreLab Partners Inc, Shanghai, China) using a proprietary and validated electronic caliper system applied on a computer screen (WebHeartTM). In compliance with current industry and regulatory standards, a single individual reviewed all of the ECGs of a single subject4. All measurements were subjected to a quality control review and validated by a senior, experienced physician cardiovascular specialist. At the core ECG laboratory, the extracted digital 12-lead ECGs were identified to the reviewer only by a unique ECG ID number in order to maintain a fully blinded analysis methodology.
Pharmacokinetic assessments
To assess the plasma concentration of moxifloxacin, blood samples of 3 mL were drawn from a suitable forearm vein on Day 2 and Day 9 during the ECG recordings. The collected blood samples were centrifuged at 3000 r/min for 5 min at room temperature. The separated plasma was stored at −20 °C.
A liquid chromatography tandem mass spectrometry (LC-MS/MS) method for determination of moxifloxacin in human plasma was established and validated. The analytical method for the plasma consisted of the following reagents and procedures: 100 L human plasma, 10 μL 25% acetonitrile solution, 10 μL internal standard (IS) working solution, and 200 μL acetonitrile solution were mixed by shaking in a 1.5 mL polypropylene tube for 30 s and centrifuged at 15 000×g for 3 min. The supernatant was diluted with an equal volume of water in sample vials, and 5 μL of the dilution was injected into the LC-MS/MS (Applied Biosystems API 5500, CA, USA).
The lowest and highest limits of quantification were 40 and 10000 ng/mL, respectively. The accuracy ranged from 87.3% to 103.3%, and the within- and between- precision was high (coefficient of variation <7%).
Safety assessments
Safety assessments included physical examinations, vital signs, resting 12-lead ECGs, 24 h heart rhythm Holter monitoring, safety clinical laboratory tests (biochemistry, hematology and urinalysis) and adverse event (AE) monitoring.
Statistical analysis
3 QT corrections were considered in this analysis:
the Fridericia9 correction, QTcF=QT/RR1/3;
an individual correction, QTcI10,11=QT/RRβ, where β is the slope of the regression of ln(QT) on ln(RR) for individual subjects using the baseline and placebo data only (individual ECGs, not triplicate means);
a study-specific correction, QTcSS12=QT/RRλ, where λ is the median value of the β values for the individual subjects as defined for QTcI.
Cross-over analyses of the data were done separately at each time point using an analysis of variance model including factors for treatment (moxifloxacin or placebo), sequence, period and subject. A two-sided 90% CI was derived for the QTc difference (moxifloxacin minus placebo) at each time point. Assay sensitivity was deemed appropriate if the lower 95% one-sided limit of the CI of the QTc difference between moxifloxacin and placebo was ≥5 ms.
A linear modeling approach was used to quantify the relationship between the plasma concentration of drug and the change in the QTc interval (time-matched difference between moxifloxacin and placebo). All statistical analyses were performed using STATA V10SE software (StataCorp LP, College Station, Texas, USA).
Results
Subject demographics and disposition
A total of 57 volunteers were screened. Twenty-four volunteers were enrolled and randomized to either the moxifloxacin/placebo or the placebo/moxifloxacin sequence group. All of the subjects were healthy male Chinese volunteers with a mean age (SD) of 25.1 (4.4) years, a mean weight of 65.7 (8.8) kg and a mean BMI of 22.2 (2.4) kg/m2. There were no subject withdrawals from the study. The data from all randomized subjects were included in the analysis.
Comparison of QT correction methods
Individual subject regressions slopes of ln(QT) on ln(RR) for drug-free data ranged between 0.109 and 0.371 with a median value of 0.253. Thus, the study-specific correction for this study was calculated as QTcSS=QT/RR0.253.
The regression slopes for ln(QTcF) on ln(RR) were negative for all subjects except two, and the 95% confidence intervals for both the mean and the median slope excluded zero, indicating that the Fridericia correction does not completely remove the influence of heart rate on the QTc value for these subjects.
The mean (across time points) estimated standard deviations of the differences between 2 (triplicate mean) observations in the same subject was derived from the analysis of variance and were calculated as 7.70 ms for QTcI, 7.93 ms for QTcSS and 8.56 ms for QTcF. These data suggest that 75 ECGs per regression provides a QTcI that may be a more reliable correction method than QTcSS; however, this conclusion does not necessarily hold with fewer ECGs for each regression. The QTcI was selected as the primary correction for this study.
Effect of moxifloxacin on the change in QTc interval from base-line
Table 1 and Figure 1 show the placebo-adjusted moxifloxacin QTc change from baseline (CFB). Overall, there is an increase in QTcI at all time points beginning at approximately 2 ms at the 0.5 h time point. This increase rose between 5.88 and 8.35 ms between the 1.5 and 10 h time points and subsequently decreased to approximately 4 ms at the 12 and 24 h time points. The lower two-sided 90% confidence limit (equivalent to the lower one-sided 95% limit) reached above 5 ms at 2 time points only (3 and 4 h). The effects are statistically significant at all time points except 0.5 h. Statistically significant period effects were also observed at certain time points.

The placebo-adjusted QTcI change from baseline (CFB) following oral administration of 400 mg moxifloxacin in 24 healthy Chinese subjects. Data were subjected to an analysis of variance. The error bars represent 90% (two-sided) confidence intervals.
Although the QTcI was the primary correction for this study, QTcF is a common correction method; therefore, a summary of the QTcF data has been included in Table 2. As with QTcI, the estimated QTcF effects are positive at all time points after drug administration. The lower limit of the 90% CI of the difference in QTcF time-matched changes from baseline between moxifloxacin and the placebo groups was >5 ms at 4 time points (2.5, 3, 4, and 8 h). The peak effect on QTcF was 9.35 ms at 3 h post-dose.
Heart rate, PR, and QRS
Table 2 shows the placebo-adjusted mean differences in CFB for heart rate and PR. For heart rate, the mean changes were generally small (always <5 bpm) and were positive or negative at various time points. Statistically significant changes (decreases) were observed at 2 time points (6 and 24 h). The 6 h time point also showed a significant period effect.
For the PR interval, an analysis of variance showed that the treatment effect was negative at all time points except for the 24 h observation. The difference rarely exceeded 3 ms, but it was statistically significant at 6 and 8 h post-dose. No period effects were detected.
For the QRS interval, the analysis of variance confirmed the general absence of any treatment or period effects.
Outlier analysis
Four (triplicate mean) ECGs had a change from baseline >30 ms, including 3 from the moxifloxacin group and one from the placebo group. There were no instances of changes from baseline exceeding 60 ms. No subject had an absolute QTcI interval >450 ms.
Pharmacokinetics of moxifloxacin
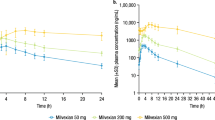
The pharmacokinetic parameters of moxifloxacin were estimated using standard non-compartmental methods with Drug and Statistics software version 2.1 (University of Science and Technology, Hefei, China). The pharmacokinetic profile of moxifloxacin is summarized in Table 3. The mean plasma moxifloxacin concentration versus time profile is presented in Figure 2. Following a single oral administration of 400 mg moxifloxacin, moxifloxacin was rapidly absorbed and showed a mean Tmax of 2.33 h. The mean maximum plasma concentration (Cmax) and mean exposure (AUC0–24) were 3.13 μg/mL and 31.97 μg·h·mL−1, respectively (Table 3).

The mean plasma concentration versus time following the oral administration of 400 mg moxifloxacin in 24 healthy Chinese subjects. The error bars denote±1 SD.
PK/QTcI analysis
The concentration-response relationship was assessed by comparing the concentration of moxifloxacin (range: 0–3925 ng/mL) with the placebo-adjusted QTcI CFB (Figure 3) using a linear mixed-effect model. The estimated slope was 0.00208 ms/(ng/mL) (95% confidence interval 0.00129, 0.00288), suggesting that for every 1000 ng/mL increase in moxifloxacin concentration within this range, there is an increase of ∼2.084 ms in the QTcI interval.

The observed data and predicted placebo-corrected QTcI CFB mean values of the plasma concentration following oral administration of 400 mg moxifloxacin in 24 healthy Chinese subjects. Vertical lines indicate the mean Cmax. CFB, change from baseline.
Safety and tolerability
A total of 4 AEs were reported during the study. All AEs were considered to be mild. Two of the AEs were electrode pad allergies, which were considered unrelated to moxifloxacin. The other 2 AEs were diarrhea, which occurred in the same subject after both the moxifloxacin and placebo administration. No serious adverse events were reported. Clinically significant changes in laboratory tests, vital signs, or electrocardiogram safety parameters were not observed. Overall, moxifloxacin was well tolerated by healthy subjects in this study.
Discussion
For this study population, the Fridericia QT correction did not adequately remove the effect of heart rate on the QTc interval. While both QTcI and QTcSS are considered appropriate for this study, the QTcI was selected as the QT correction because of the large number of drug-free ECGs available per subject and the robust individual QT:RR slope.
The analysis of variance indicated a significant effect of moxifloxacin on QTcI prolongation with a peak effect of 8.35 ms at the 4 h time point. The 95% lower one-sided confidence limit at this time point was 5.43 ms. Thus, the results of this study meet the criteria established in the ICH-E14 guidelines4 and the E14 Q&A document5 for the confirmation of assay sensitivity. However, the prolongation of QTc in this study exceeds these criteria by a small margin.
Previous studies involving Caucasian subjects showed that moxifloxacin affects the QTc to a similar magnitude13. Florian et al14 reported a pooled analysis of 20 Thorough QT studies submitted to the US FDA. The authors reported that exposure in Asians was slightly higher than in Caucasians (2.63 vs 2.473 μg/mL, respectively); however, no significant race effects in any of the PK or concentration–QTc parameters were found. In our study, the moxifloxacin exposure (Cmax 3.13 μg/mL) was higher than that reported by Florian et al; however, the maximum QTc effect was not increased. Florian et al reported an estimated mean (90% CI) slope of 3.1 (2.8–3.3) ms per μg/mL moxifloxacin, which corresponded to an overall ddQTcF of 10.9 ms at a moxifloxacin concentration of 2.9 μg/mL14. In our study, the mean (90% CI) slope was 2.92 (2.04, 3.79) ms per μg/mL moxifloxacin, which corresponded to a mean ddQTcF effect of 10.6 ms at the moxifloxacin Cmax(3.13 μg /mL).
These data support the conclusion that despite a higher exposure, our study population appears to have a similar moxifloxacin QTcF effect to that reported by Florian et al for Caucasian subjects. Thus, these results are consistent with Florian's conclusion that there is no significant difference in the concentration: QTcF ratio between Chinese and Caucasian subjects.
However, some studies involving Caucasian subjects showed larger QTcF effects15,16,17. Therefore, further studies are required to determine ethnicity-specific effects, especially prospectively designed direct comparisons of moxifloxacin-induced QT prolongation in Asians versus Caucasians.
Author contribution
Qian CHEN, Hua-hua PU, and Chen YU designed the research; Qian CHEN, Yan-mei LIU, Yun LIU, and Chao-ying HU conducted the research; Wei WANG was responsible for clinical observations; Gang-yi LIU measured the concentration of moxifloxacin; Onglee WENG provided the central review of the ECG data; Dennis CHANTER performed the statistical analysis; Qian CHEN and Yan-mei LIU wrote the paper; Jing-ying JIA critically revised the manuscript; and Boaz MENDZELEVSKI provided the ECG study report and assisted with the writing of the manuscript.
References
Yan GX, Lankipalli RS, Burke JF, Musco S, Kowey PR . Ventricular repolarization components on the electrocardiogram: cellular basis and clinical significance. J Am Coll Cardiol 2003; 42: 401–9.
Roden DM . Drug-induced prolongation of the QT interval. N Engl J Med 2004; 350: 1013–22.
Strnadova C . The assessment of QT/QTc interval prolongation in clinical trials: a regulatory perspective. Drug Information J 2005; 39: 407–33.
International Conference on Harmonisation (ICH). ICH topic E14. The clinical evaluation of QT/QTc interval prolongation and proarrhythmic potential for non-antiarrhythmic drugs (Step 4). 12 May 2005. Available from: http://www.ich.org/fileadmin/Public_Web_Site/ICH_Products/Guidelines/Efficacy/E14/E14_Guideline.pdf (last accessed on 10 September 2012).
E14 implementation working group: ICH E14 guideline: the clinical evaluation of QT/QTc interval prolongation and proarrhythmic potential for non-antiarrhythmic drugs questions & answers (R1). 5 April 2012. available from: http://www.ich.org/fileadmin/Public_Web_Site/ICH_Products/Guidelines/Efficacy/E14/E14_Q_As_R1_step4.pdf (last accessed on 10 September 2012).
Darpo B . The thorough QT/QTc study 4 years after the implementation of the ICH E14 guidance. Br J Pharmacol 2010; 159: 49–57.
Tsikouris JP, Peeters MJ, Cox CD, Meyerrose GE, Seifert CF . Effects of three fluoroquinolones on QT analysis after standard treatment courses. Ann Noninvasive Electrocardiol 2006; 11: 52–6.
Van BF, Tulkens PM . Safety profile of the respiratory fluoroquinolone moxifloxacin: comparison with other fluoroquinolones and other antibacterial classes. Drug Saf 2009; 32: 359–78.
Fridericia LS . Die Systolendauer im Elektrokardiogramm bei normalen Menschen und bei Herzkranken. Acta Med Scand 1920; 53: 469–86.
Malik M . Problems of heart rate correction in assessment of drug-induced QT interval prolongation. J Cardiovasc Electrophysiol 2001; 12: 411–20.
Couderc JP, Xiaojuan X, Zareba W, Moss AJ . Assessment of the stability of the individual-based correction of QT interval for heart rate. Ann Noninvasive Electrocardiol 2005; 10: 25–34.
Van de Water A, Verheyen J, Xhonneux R, Reneman RS . An improved method to correct the QT interval of the electrocardiogram for changes in heart rate. J Pharmacol Methods 1989; 22: 207–17.
Hug B, Abbas R, Leister C, Burns J, Sonnichsen D . A single-dose, crossover, placebo- and moxifloxacin-controlled study to assess the effects of neratinib (HKI-272) on cardiac repolarization in healthy adult subjects. Clin Cancer Res 2010; 16: 4016–23.
Florian JA, Tornøe CW, Brundage R, Parekh A, Garnett CE . Population pharmacokinetic and concentration — QTc models for moxifloxacin: pooled analysis of 20 thorough QT studies. J Clin Pharmacol 2011; 51: 1152–62.
Khindri S, Sabo R, Harris S, Woessner R, Jennings S, Drollmann AF . Cardiac safety of indacaterol in healthy subjects: a randomized, multidose, placebo- and positive-controlled, parallel-group thorough QT study. BMC Pulm Med 2011; 26: 11: 31.
Dixon R, Job S, Oliver R, Tompson D, Wright JG, Maltby K, et al. Lamotrigine does not prolong QTc in a thorough QT/QTc study in healthy subjects. Br J Clin Pharmacol 2008; 66: 396–404.
Bloomfield DM, Kost JT, Ghosh K, Hreniuk K, Hickey LA, Guitierrez MJ, et al. The effect of moxifloxacin on QTc and implications for the design of thorough QT studies. Clin Pharmacol Ther 2008; 84: 475–80.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Chen, Q., Liu, Ym., Liu, Y. et al. Orally administered moxifloxacin prolongs QTc in healthy Chinese volunteers: a randomized, single-blind, crossover study. Acta Pharmacol Sin 36, 448–453 (2015). https://doi.org/10.1038/aps.2014.153
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/aps.2014.153
Keywords
This article is cited by
-
Effect of hyperglycaemia in combination with moxifloxacin on cardiac repolarization in male and female patients with type I diabetes
Clinical Research in Cardiology (2022)
-
Establishing assay sensitivity in QT studies: experience with the use of moxifloxacin in an early phase clinical pharmacology study and comparison with its effect in a thorough QT study
European Journal of Clinical Pharmacology (2015)
