
ABSTRACT
Gastric cancer is believed to result in part from the accumulation of multiple genetic alterations leading to oncogene overexpression and tumor suppressor loss. Epigenetic alterations as a distinct and crucial mechanism to silence a variety of methylated tissue-specific and imprinted genes, have been extensively studied in gastric carcinoma and play important roles in gastric carcinogenesis. This review will briefly discuss the basic aspects of DNA methylation and CpG island methylation, in particular the epigenetic alterations of certain critical genes implicated in gastric carcinogenesis and its relevance of clinical implications.
Similar content being viewed by others


INTRODUCTION
The incidence of gastric cancer has declined; however, it continues to be the second most common malignant neoplasms across the world and the second leading cause of cancer death 1. Epigenetics has an important role in biological research and affects many different areas of study including cancer biology 2, 3, viral latency 4, 5, 6, 7, activity of mobile elements 8, somatic gene therapy 9, 10, 11, 12, 13, 14, cloning and transgenic technologies, genomic imprinting 15, 16, and developmental abnormalities 15, 16. Epigenetic silencing of tumor-related genes due to CpG island methylation has been recently reported in gastric carcinoma 17. CpG islands are 0.5 to 2 kb regions rich in cytosine-guanine dinucleotides and are present in the 5′ promoter region of approximately 40-50% of human genes 18. Methylation of cytosines within CpG islands is associated with loss of gene expression by repression of transcription and is observed in tumorigenesis, as well as in physiological conditions such as X chromosome inactivation and aging 19, 20, 21, 22, 23, 24.
Gastric carcinoma can arise either from precursor lesions or de novo. It has been demonstrated that some gastric carcinoma may arise from gastric adenomas or flat dysplasias, similar to the consequence of colorectal adenoma derived from adenocarcinoma 25, 26, 27, 28. The cumulative prevalence of malignant transformation of gastric dysplasia/adenoma has been reported to be greater than 10% in long-term follow-up studies 29, 30. Epigenetic alterations have been acknowledged as an important mechanism contributing to early gastric carcinogenesis. Previous studies have characterized epigenetic abnormalities in intestinal metaplasia (IM) and adenoma, which are precursors of invasive adenocarcinoma 31, 32.
DNA METHYLATION IN CANCER
DNA methylation has become the topic of intense investigation in cancer cells. As compared with normal cells, the malignant cells show major disruptions in their DNA methylation patterns 32. The tumor cells are characterized by significant modifications of DNA methylation system including general genome demethylation, increase in DNA methyltransferase activity, and local hypermethylation 34, 35. These modifications seem to be contradictory, since it seems difficult to explain the increase in DNA methyltransferase activity with local hypermethylation of the genome and overall demethylation on the remaining genome. This contradiction is further clarified by better understanding of the DNA methylation system. The demethylation has been estimated to involve almost exclusively the “dispersed” CpG (∼80% of total content, and they are methylated in normal cells). In contrast, local hypermethylation occurs on the CpG islands (about 20% of total content, and are not methylated in normal cells excluding certain exceptions) does not compensate the demethylation of “dispersed” CpG to give general genome demethylation. In tumor cells the reciprocal relations between the methylation levels of the CpG islands and of “dispersed” CpG, are also preserved. The increased activity of DNA methyltransferase frequently seen in tumor cells can be one of the factors responsible for the aberrant methylation of CpG islands.
Methylation of tumor suppressor genes
Inactivation of tumor suppressor genes by DNA methylation in promoter region plays an important role in carcinogenesis. The tumor suppressor genes that undergo aberrant CpG island methylation in human cancer can affect important cellular pathways including cell cycle regulation and proliferation. For example, in p16INK4a/Rb/cdk4 pathway, the cell-cycle inhibitor p16INK4a is methylated in various human primary tumors and cell lines 36, 37, allowing the cancer cells to escape senescence and to proliferate Rb itself can also be occasionally inactivated by aberrant methylation 38, 39. APC/β-catenin/E-cadherin pathway has been altered in a variety of human cancers. APC gene is commonly mutated in sporadic colon cancer but the role of the APC mutation in other tumor systems is not clear. Recently, it is been shown that aberrant methylation of APC is a common phenomenon in other aerodigestive tract neoplasms 40 and that E-cadherin promoter hypermethylation is important for the cancer biology of breast and other tumor types 41, 42.
Methylation in DNA mismatch repair gene
DNA mismatch is in the crossroad of all other cellular pathways. DNA methylation is one of the major players in causing alterations of DNA mismatch repair genes. Methylation-mediated silencing of the mismatch DNA repair gene hMLH1 in sporadic cases of colorectal, endometrial, and gastric cancers are responsible for the high level of microsatellite instability in tumors 43, 44, 45, 46, 47. The promoter hypermethylation of MGMT 48 that prevents the removal of groups at the O6 position of the guanine is associated with particular type of K-ras and p53 mutations 49, 50; and the somatic inactivation of BRCA1 by aberrant methylation altering its role in the repair of DNA double-strand breaks in breast and ovarian tumors 51.
Two types of DNA methylation
Not all of the DNA methylation are tumor specific. In colon tissues, studies have shown DNA methylation in certain genes such as ERα, N33 and MYOD are age-related, and this type of methylation is classified as Type A methylation. In contrast, tumor-specific methylation such as p16 and hMLH1 is classified as Type C methylation 17. A similar distinction between age-related and tumor-specific methylation has also been shown in gastric cancer 52, 53. In stomach, age-related Type A methylation genes include E-cadherin and APC 32, 53. In addition, Waki et al found that methylation of DAP-kinase, like that of E-cadherin, was also age-related. The methylation of DAP-kinase in non-neoplastic epithelia frequently appears at around age 45 54.
The significance of the detection of the methylated gene can depend on the position of the CpG sites examined. Methylation of hMLH1 gene, which was thought to be cancer-specific 17, was found to be a common age-related event in normal colonic mucosa, when the entire hMLH1 promoter ∼700 bp region was analyzed 55. Partial methylation on hMLH1 promoter region is frequently present in normal colonic mucosa, especially in older patients. The hMLH1 gene will ultimately shut down when the methylation spreads to reach a threshold 55. Therefore, these contradictory results might have been due to analysis of different CpG sites 17, 55. In addition, it has recently been reported that DAP-kinase methylation was present in virtually every tumor and normal gastric and colorectal sample when the edge of CpG islands was examined, although it turned out to be a rather infrequent, cancer-specific phenomenon when the central region of the CpG islands was analyzed 56.
CpG island methylator phenotype
Tumors with concurrent methylation in multiple genes or loci have been defined as CpG island methylation phenotype-high (CIMP-H) in colorectal and gastric cancers 17, 52. The mechanism of concurrent hypermethylation of multiple genes remains obscure. Apparently, the increase in DNA methyltransferase activity plays an important role. Transfection of a cloned human DNMT1 gene into immortalized human fibroblasts leads to the aberrant methylation of CpG islands in promoter regions of several genes, including E-cadherin and HIC1, but CpG islands associated with other genes (for example, p16INK4a) are not altered in methylation state, although DNMT1 is expressed constantly 57. Therefore, it is evident that the increase in DNMT1 activity can play a significant role in the selective aberrant methylation of CpG islands, but not in total CpG island methylation.
CIMP-H affects only a subset of tumors and a limited number of genes. The defect that leads to CIMP-H could be either aberrant de novo methylation (through a mutation in DNA-methyltransferase for example) or loss of protection against de novo methylation through the loss of a trans-activating factor 58, 59, 60. These CIMP-H tumors may then develop through a pathway that heavily relies on this methylation defect, whereas others rarely show tumor suppressor gene methylation. Aberrant methylation often occurs in CpG islands outside of promoter regions in which it may not affect gene transcription 61. An important question is whether the concordant methylation described here provides a growth advantage to affect cells or whether it just accompanies tumor development. Additional studies are necessary to clarify whether the genes methylated in cancer simply reflect the genome wide methylation defect or whether stochastic methylation of each CpG island results from selective pressures.
EPIGENETIC ALTERATIONS IN EARLY GASTRIC TUMORIGENESIS
There are two major histological types of gastric adenocarcinoma (intestinal and diffuse) according to the Lauren's classification 62. The pathogenesis and genetic alterations for these two distinct types of adenocarcinoma are also different 63, 64, 65. The most frequent gastric malignancy is the intestinal type, which is often preceded by sequential steps of precancerous changes, including atrophic gastritis, intestinal metaplasia, and either dysplasia or adenoma. In contrast, the diffuse type of gastric carcinoma tends to arise de novo and is infrequently associated with dysplasia or adenoma 66, 67, 68, 69. The sequential accumulation of alternations of APC and K-ras genes, characteristic of the colorectal adenoma-carcinoma sequence, however, does not occur frequently between adenoma and intestinal type adenocarcinoma of the stomach 27, 70, 71, 72, 73, 74, 75, 76, 77. There are two lines of evidence indicating that not all gastric dysplastic lesions are precursor lesions for gastric carcinoma. First, gastric dysplasia can undergo spontaneous regression clinically, especially low-grade dysplastic lesions, and only 11–40% of adenoma/dysplasia progress to carcinoma 29, 78, 79, 80, 81. Secondly, APC mutations have been reported to occur more frequently in gastric adenomas than in gastric adenocarcinomas 75, 76, 77, 81.
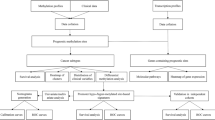
The status of methylation in multiple genes or loci has been studied extensively in early gastric tumorigenesis following the stepwise morphologic changes as summarized in Fig. 1 and Tab. 1. Methylation of tumor suppressor genes are frequently present in the non-neoplastic gastric mucosa including chronic gastritis and intestinal metaplasia (IM). Kang et al 32 determined the methylation frequency of 12 genes, including APC, COX-2, DAP-kinase, E-cadherin, GSTP1, hMLH1, MGMT, p16, p14, RASSF1A, THBS1, and TIMP3, by methylation-specific PCR in this progression sequence. In this study five different classes of methylation behaviors were found: (1) genes only methylated in carcinoma such as GSTP1 and RASSF1A; (2) genes showing low methylation frequency in chronic gastritis, IM, and gastric adenoma but significantly higher methylation frequency in carcinoma such as COX-2, hMLH1, and p16; (3) a gene with low and similar methylation frequency in four-step lesions such as MGMT, (4) genes with high and similar methylation frequency in four-step lesions such as APC and E-cadherin, and (5) genes showing an increasing tendency of the methylation frequency along the progression such as DAP-kinase, p14, THBS1, and TIMP-3. A similar result has also been shown by other studies. To et al showed three differential methylation patterns: methylation was more frequent in cancer than in IM (DAP-kinase, p14, p15 and p16); comparable frequencies of methylation in cancer and IM (E-cadherin and hMLH1); and no methylation (GSTP1) 82. Among these genes evaluated, it appears that at least methylation of APC and E-cadherin are not tumor specific but rather an age-related phenomenon (Type A methylation gene for stomach). Therefore, it is crucial to include control non-neoplastic gastric mucosa; in methylation study of gastric precursor lesions and carcinomas. It is however, difficult to classify genes such as DAP-kinase, THBS1 and TIMP-3 in which methylation is frequently detected in non-neoplastic mucosa and precursor lesions but a higher frequency of methlyation is present in carcinoma stage based on Type A or Type C methlyation gene classification (Fig. 1).

Epigenetic alterations in the multistep gastric carcinogenesis pathway following the chronic gastritis-intestinal metaplasia-adenoma/dysplasia-adenocarcinoma sequence. Methylation of APC and E-cadherin genes occur frequently in normal gastric mucosa and chronic gastritis, and uniformly through the sequence is classified as Type A (age-related) methylation genes. The remaining genes are classified as Type C (tumor-specific) methylation genes. Genes such as DAP-kinase, MGMT, TIMP3 and THBS1 are frequently methylated in intestinal metaplasia stage, but the methylation frequency is higher in precursor lesions or adenocarcinoma, therefore also classified as Type C methylation genes. Gastric carcinoma can be further subclassified based on the extent of methylation; CIMP-high (CIMP-H) with concurrent methylation of multiple genes in ≥50% of assessed genes, CIMP-low (CIMP-L) with methylation in <50% of assessed genes, or CIMP-negative (CIMP-N) with no methylated genes. In tumor with CIMP-H, methylation of hMLH1 gene is also associated with microsatellite instability-high (MSI-H) phenotype.
Concurrent methylation of multiple tumor-related genes has been detected in 20% of normal tissues adjacent to gastric carcinoma by Leung et al 83. We have also shown concurrent methylation (CIMP-H) in 15% of IM but not in chronic gastritis or normal gastric mucosa using a panel of six genes/loci including p16, hMLH1 and four CpG islands (MINT1, MINT2, MINT25 and MINT31) 81. MINT loci were methylated in 6–21% of normal mucosa, and in 10–41% of IM. In particular, methylation of MINT25 was more frequent in normal/chronic gastritis mucosa contiguous with neoplasms and in IM than in noncontiguous normal/chronic gastritis mucosa. The mean methylation index and frequency of CIMP-H increased following the normal/chronic gastritis, IM, adenoma/dysplasia and early adenocarcinoma sequence indicating accumulation of methylation events may play an important role in early gastric tumorigenesis (Fig. 2) 81.

The frequency of concurrent methylation in multiple genes/loci (CIMP-H) increased with the histological progression from normal (NM)/chronic gastritis (CG), to Intestinal metaplasia (IM), adenomas or dysplasias, and early adenocarcinomas. The majorities of the non-neoplastic mucosa (NM, CG and IM) are CIMP-L or CIMP-N.
There are two morphologically distinct gastric precancerous lesions: adenoma (polypoid dysplastic mucosal lesion) and flat dysplasia. Genetic and epigenetic alterations separating these two distinct morphological precancerous lesions remain unclear. We have shown that there was no difference in the frequency of individual gene/loci or in frequency of CIMP-H between flat dysplasias (50%) and polypoid adenomas (51%) 81. Interestingly, we have found that methylation of p16 gene was more frequent in adenocarcinoma-associated dysplasia/adenoma and adenocarcinomas as compared to adenoma/dysplasia unassociated with adenocarcinoma, indicating methylation of p16 gene may contribute to the malignant transformation of gastric precursor lesions 81.
EPIGENETIC ALTERATIONS IN GASTRIC CARCINOMA
The roles of epigenetic alterations in the pathogenesis of gastric carcinomas have been recently elucidated. Toyota et al first demonstrated that about one-half of all gastric cancers had frequent methylation in multiple genes/loci including p16, hMLH1 and multiple tumor specific CpG islands (MINT1, MINT2, MINT12, MINT25, and MINT31) that seemed to be methylated de novo during cancer progression and play an important role in gastric carcinogenesis 52. Subsequently, numerous other genes with methylation have been found in gastric carcinomas as shown in Fig. 1 and Tab. 1.
Similar to colorectal cancer, the presence of methylation of hMLH1 gene is strongly associated with loss of hMLH1 protein expression and MSI-H phenotype in gastric carcinomas 52, 81, 83. In contrast to gastric carcinoma, methylation of hMLH1 genes in gastric precursor lesions appears to be less frequently associated with MSI-H phenotype and loss of hMLH1 protein expression 81. The reason for this discrepancy is not clear, but it is possible that hMLH1 methylation precede the loss of protein expression.
Genetic alteration of E-cadherin gene has been frequently detected in gastric carcinomas, especially for diffuse type adenocarcinoma. Tamura et al reported that E-cadherin promoter hypermethylation was seen in 27 (51%) of 53 primary gastric carcinomas, including 15 (83%) of 18 undifferentiated (diffuse) type, and E-cadherin promoter hypermethylation was seen at similar frequencies in both early and advanced cases 84. However, the presence of E-cadherin gene methylation in non-neoplastic gastric mucosa makes difficult to determine its role in gastric carcinogenesis.
In gastric cancer, CIMP-H has been described in 41% of the tumors by Toyota et al 52. We have also detected CIMP-H in 31% of the gastric carcinomas using a similar panel of genes/loci 85. Etoh et al have shown that increased DNMT1 protein expression correlated significantly with DNA methylation of multiple CpG islands in poorly differentiated gastric cancers, suggested that DNMT1 may play a significant role in the development of poorly differentiated gastric cancers by inducing frequent DNA methylation of multiple CpG islands 86.
CLINICAL IMPLICATIONS
The clinical significance of presence of epigenetic alterations in gastric cancer remains unclear. It would be important to know whether the presence or absence of certain epigenetic changes affects the prognosis. This would also help in modifying initial patient treatment options and monitoring response to therapy. It is particularly important to identify any specific epigenetic alterations in gastric precursor lesions for predicting malignant transformation since not all the gastric precursor lesions carry the same malignant transforming potential. Epigenetic silencing of a tumor suppressor gene could be the rate-limiting step that initiates the series of events leading to an invasive malignant tumor. Methylation of p16 gene appears to be a promising candidate to serve this purpose as shown in our study 81 and supported in a population-based study by Sun et al that aberrant methylation of p16 promoter CpG islands might be useful to predict the malignant potential of dysplasia identified specifically in gastric biopsies 87.
The prognosis of methylation of single genes/loci is unclear in gastric cancer, but it has been reported that methylation of MGMT gene was associated with advance stage and poor prognosis 88. We have recently shown that concordant methylation of multiple gene/loci (CIMP-H) is associated with better survival but is not an independent predictor of prognosis in resected gastric cancer 85. The sensitivity and specificity of DNA methylation markers in cancer diagnosis depends on several factors, including the type of cancer and the gene to be studied, the type of body fluid to be used, and the techniques involved. The assay needs to be standardized and shown to be useful in a prospective fashion before it can become clinically useful. A more comprehensive methylation profiling for gastric cancer will be needed to achieve this goal.
References
Nardone G . Molecular basis of gastric carcinogenesis. Aliment Pharmacol Ther 2003; 17:75–81.
Baylin SB . Tying it all together: epigenetics, genetics, cell cycle, and cancer. Science 1997; 277:1948–9.
Jones PA, Baylin SB . The fundamental role of epigenetic events in cancer. Nat Rev Genet 2002; 3:415–28.
Takacs M, Salamon D, Myohanen S, et al. Epigenetics of latent Epstein-Barr virus genomes: high resolution methylation analysis of the bidirectional promoter region of latent membrane protein 1 and 2B genes. Biol Chem 2001; 382:699–705.
Tierney RJ, Kirby HE, Nagra JK, et al. Methylation of transcription factor binding sites in the Epstein-Barr virus latent cycle promoter Wp coincides with promoter down-regulation during virus-induced B-cell transformation. J Virol 2000; 74:10468–79.
Robertson KD . The role of DNA methylation in modulating Epstein-Barr virus gene expression. Curr Top Microbiol Immunol 2000; 249:21–34.
Tao Q, Swinnen LJ, Yang J, et al. Methylation status of the Epstein-Barr virus major latent promoter C in iatrogenic B cell lymphoproliferative disease: application of PCR-based analysis. Am J Pathol 1999; 155:619–25.
Hagan CR, Rudin CM . Mobile genetic element activation and genotoxic cancer therapy: potential clinical implications. Am J Pharmacogenomics 2002; 2:25–35.
Nelson WG, De Marzo AM, Deweese TL, et al. Preneoplastic prostate lesions: an opportunity for prostate cancer prevention. Ann N Y Acad Sci 2001; 952:135–44.
Rideout WM III, Eggan K, Jaenisch R . Nuclear cloning and epigenetic reprogramming of the genome. Science 2001; 293:1093–8.
Nelson WG, De Marzo AM, DeWeese TL . The molecular pathogenesis of prostate cancer: implications for prostate cancer prevention. Urology 2001; 57(Suppl 1):39–45.
Howell CY, Bestor TH, Ding F, et al. Genomic imprinting disrupted by a maternal effect mutation in the Dnmt1 gene. Cell 2001; 104:829–38.
El-Osta A, Wolffe AP . DNA methylation and histone deacetylation in the control of gene expression: basic biochemistry to human development and disease. Gene Expr 2000; 9:63–75.
Zuccotti M, Garagna S, Redi CA . Nuclear transfer, genome reprogramming and novel opportunities in cell therapy. J Endocrinol Invest 2000; 23:623–9.
Feinberg AP . Cancer epigenetics takes center stage. Proc Natl Acad Sci USA 2001; 98:392–4.
Feinberg AP . DNA methylation, genomic imprinting and cancer. Curr Top Microbiol Immunol 2000; 249:87–99.
Toyota M, Ahuja N, Ohe-Toyota M, et al. CpG island methylator phenotype in colorectal cancer. Proc Natl Acad Sci U S A 1999; 96:8681–6.
Momparler RL, Bovenzi V . DNA methylation and cancer. J Cell Physiol 2000; 183:145–154.
Jones PA, Laird PW . Cancer epigenetics comes of age. Nat Genet 1999; 21:163–7.
Li E, Beard C, Jaenisch R . Role for DNA methylation in genomic imprinting. Nature 1993; 366:362–5.
Panning B, Jaenisch R . RNA and the epigenetic regulation of X chromosome inactivation. Cell 1998; 93:305–8.
Baylin SB, Herman JG . DNA hypermethylation in tumorigenesis: epigenetics joins genetics. Trends Genet 2000; 16:168–74.
Toyota M, Issa JP . The role of DNA hypermethylation in human neoplasia. Electrophoresis 2000; 21:329–33.
Wajed SA, Laird PW, DeMeester TR . DNA methylation: an alternative pathway to cancer. Ann Surg 2001; 234:10–20.
Correa P . Human gastric carcinogenesis: a multistep and multifactorial process-first American cancer society award lecture on cancer epidemiology and prevention. Cancer Res 1992; 52:6735–40.
Correa P, Shiao YH . Phenotypic and genotypic events in gastric carcinogenesis. Cancer Res 1994; 54:1941s–3s.
Maesawa C, Tamura G, Suzuki Y, et al. The sequential accumulation of genetic alterations characteristic of the colorectal adenoma-carcinoma sequence does not occur between gastric adenoma and adenocarcinoma. J. Pathol 1995; 176:249–58.
Stadtlander CT, Waterbor JW . Molecular epidemiology, pathogenesis and prevention of gastric cancer. Carcinogenesis 1999; 20:2195–208.
Kolodziejczyk P, Yao T, Oya M, et al. Long-term follow-up study of patients with gastric adenomas with malignant transformation An immunohistochemical and histochemical analysis. Cancer 1994; 74:2896–907.
Orlowska J, Jarosz D, Pachlewski J, et al. Malignant transformation of benign epitherial gastric polyps. Am J Gastroenterol 1995; 90:2152–9.
Kang GH, Shim YH, Jung HY, et al. CpG island methylation in premalignant stages of gastric carcinoma. Cancer Res 2001; 61:2847–51.
Kang GH, Lee S, Kim JS, Jung HY . Profile of aberrant CpG island methylation along multistep gastric carcinogenesis. Lab Invest 2003; 83:519–26.
Baylin SB, Herman JG, Graff JR, et al. Alterations in DNA ethylation: a fundamental aspect of neoplasia. Adv Cancer Res 1998; 72:141–96.
Jones PA . DNA methylation errors and cancer. Cancer Res 1996; 56:2463–7.
Laird PW, Jaenisch R . DNA methylation and cancer. Hum Mol Genet 1994; 3:1487–95.
Herman JG, Merlo A, Mao L, et al. Inactivation of the CDKN2/ p16/MTS1 gene is frequently associated with aberrant DNA methylation in all common human cancers. Cancer Res 1995; 55:4525–30.
Merlo A, Herman JG, Mao L, et al. 5k CpG island methylation is associated with transcriptional silencing of the tumour suppressor p16/CDKN2/MTS1 in human cancers. Nature Med 1995; 1:686–92.
Sakai T, Toguchida J, Ohtani N, et al. Allele-specific hypermethylation of the retinoblastoma tumor-suppressor gene. Am J Hum Genet 1991; 48:880–8.
Greger V, Passarge E, Hopping W, et al. Epigenetic changes may contribute to the formation and spontaneous regression of retinoblastoma. Hum Genet 1989; 83:155–8.
Esteller M, Sparks A, Toyota M . Analysis of adenomatous polyposis coli promoter hypermethylation in human cancer. Cancer Res 2000; 60:4366–71.
Esteller M, Corn PG, Baylin SB, et al. A gene hypermethylation profile of human cancer. Cancer Res 2001; 61:3225–9.
Graff JR, Herman JG, Lapidus RG, et al. E-cadherin expression is silenced by DNA hypermethylation in human breast and prostate carcinomas. Cancer Res 1995; 55:5195–9.
Kane MF, Loda M, Gaida GM, et al. Methylation of the hMLH1 promoter correlates with lack of expression of hMLH1 in sporadic colon tumors and mismatch repair-defective human tumor cell lines. Cancer Res 1997; 57:808–11.
Herman JG, Umar A, Polyak K, et al. Incidence and functional consequences of hMLH1 promoter hypermethylation in colorectal carcinoma. Proc Natl Acad Sci U S A 1998; 95:6870–5.
Esteller M, Levine R, Baylin SB, et al. MLH1 promoter hypermethylation is associated with the microsatellite instability phenotype in sporadic endometrial carcinomas. Oncogene 1998; 17:2413–7.
Esteller M, Catasus L, Matias-Guiu X, et al. hMLH1 promoter hypermethylation is an early event in human endometrial tumorigenesis. Am J Pathol 1999; 155:1767–72.
Fleisher AS, Esteller M, Wang S, et al. Hypermethylation of the hMLH1 gene promoter in human gastric cancers with microsatellite instability. Cancer Res 1999; 59:1090–5.
Esteller M, Hamilton SR, Burger PC, et al. Inactivation of the DNA repair gene O6-methylguanine-DNA methyltransferase by promoter hypermethylation is a common event in primary human neoplasia. Cancer Res 1999; 59:793–7.
Esteller M, Toyota M, Sanchez-Cespedes M, et al. Inactivation of the DNA repair gene O6-methylguanine-DNA methyltransferase by promoter hypermethylation is associated with G to A mutations in K-ras in colorectal tumorigenesis. Cancer Res 2000; 60:2368–71.
Esteller M, Risques RA, Toyota M, et al. Promoter hypermethylation of the DNA repair gene O6-methylguanine-DNA methyltransferase is associated with the presence of G : C to A : T transition mutations in p53 in human colorectal tumorigenesis. Cancer Res 2001; 61:4689–92.
Esteller M, Silva JM, Dominguez G, et al. Promoter hypermethylation and BRCA1 inactivation in sporadic breast and ovarian tumors. J Natl Cancer Inst 2000; 92:564–9.
Toyota M, Ahuja N, Suzuki H, et al. Aberrant methylation in gastric cancer associated with the CpG island methylator phenotype. Cancer Res 1999; 59:5438–42.
Kang GH, Lee HJ, Hwang KS, et al. Aberrant CpG island hypermethylation of chronic gastritis, in relation to aging, gender, intestinal metaplasia, and chronic inflammation. Am J Pathol 2003; 163:551–6.
Waki T, Tamura G, Sato M, et al. Promoter methylation status of DAP-kinase and RUNX3 genes in neoplastic and non-neoplastic gastric epithelia. Cancer Sci. 2003; 94:360–4.
Nakagawa H, Nuovo GJ, Zervos EE, et al. Age-related hypermethylation of the 5′ region of MLH1 in normal colonic mucosa is associated with microsatellite-unstable colorectal cancer development. Cancer Res 2001; 61:6991–5.
Satoh A, Toyota M, Itoh F, et al. DNA methylation and histone deacetylation associated with silencing DAPkinase gene expression in colorectal and gastric cancers. Br J Cancer 2002; 86:1817–23.
Vertino PM, Yen RW . De novo methylation of CpG island sequences in human fibroblasts overexpressing DNA (cytosine-5-)-methyltransferase. Mol Cell Biol 1996; 16:4555–65.
Macleod D, Charlton J, Mullins J, et al. Sp1 sites in the mouse aprt gene promoter are required to prevent methylation of the CpG island. Genes 1994; 8:2282–92.
Chen FY, Harris LC, Remack JS, et al. Cytoplasmic sequestration of an O6-methylguanine-DNA methyltransferase enhancer binding protein in DNA repair-deficient human cells. Proc Nat Acad Sci USA. 1997; 94:4348–53.
Mummaneni P, Yates P, Simpson J, et al. The primary function of a redundant Sp1 binding site in the mouse aprt gene promoter is to block epigenetic gene inactivation. Nucleic Acids Res 1998; 26:5163–9.
Liang G, Salem CE, Yu MC, et al. DNA methylation differences associated with tumor tissues identified by genome scanning analysis. Genomics 1998; 53:260–8.
Lauren P . The two histological main types of gastric carcinoma: diffuse and so-called intestinal-type carcinoma. Acta Pathol Microbiol Scand 1965; 64:31–49.
Stadtlander CT, Waterbor JW . Molecular epidemiology, pathogenesis and prevention of gastric cancer. Carcinogenesis 1999; 20:2195–208.
Tahara E, Semba S, Tahara H . Molecular biological observations in gastric cancer. Semin Oncol 1996; 23:307–15.
Chan AO, Luk JM, Hui WM, et al. Molecular biology of gastric carcinoma: from laboratory to bedside. J Gastroenterol Hepatol 1999; 14:150–60.
Correa P . Human gastric carcinogenesis: a multistep and multifactorial process—first american cancer society award lecture on cancer epidemiology and prevention. Cancer Res 1992; 52:6735–40.
Correa P, Shiao YH . Phenotypic and genotypic events in gastric carcinogenesis. Cancer Res 1994; 54:(Suppl):1941s–3s.
Correa P . A human model of gastric carcinogenesis. Cancer Res 1988; 48:3554–60.
Solcia E, Fiocca R, Luinetti O, et al. Intestinal and diffuse gastric cancers arise in a different background of Helicobacter pylori gastritis through different gene involvement. Am J Surg Pathol 1996; 20:(Suppl 1):S8–S22.
Horii A, Nakatsuru S, Miyoshi Y, et al. The APC gene, responsible for familial adenomatous polyposis, is mutated in human gastric cancer. Cancer Res 1992; 52:3231–3.
Nishimura K, Yokozaki H, Jaruma K, et al. Alternations of the APC gene in carcinoma cell lines and precancerous lesions of the stomach. Int J Oncol 1995; 7:587–92.
Arber N, Shapira I, Ratan J, et al. Activation of c-K-ras mutations in human gastrointestinal tumors. Gastroenterology 2000; 18:1045–50.
Kihana T, Tsuda H, Hirota T, et al. Point mutation of c-Ki-ras oncogene in gastric adenoma and adenocarcinoma with tubular differentiation. Jpn J Cancer Res 1991; 82:308–14.
Lee KH, Lee JS, Suh C, et al. Clinicopathologic significance of the K-ras gene codon 12 point mutation in stomach cancer. An analysis of 140 cases. Cancer 1995; 75:2794–801.
Nakatsuru S, Yanagisawa A, Furukawa Y, et al. Somatic mutations of the APC gene in precancerous lesion of the stomach. Hum Mol Genet 1993; 2:1463–5.
Tamura G, Maesawa C, Suzuki Y, et al. Mutations of the APC gene occur during early stages of gastric adenoma development. Cancer Res 1994; 54:1149–51.
Rugge M, Farinati F, Di Mario F, et al. Gastric epithelial dysplasia: a prospective multicenter follow-up study from the Interdisciplinary Group on Gastric Epithelial Dysplasia Multicenter Study. Hum Pathol 1991; 22:1002–8.
Rugge M, Farinati F, Baffa R, et al. Gastric epithelial dysplasia in the natural history of gastric cancer: a multicenter prospective follow-up study. Interdisciplinary Group on Gastric Epithelial Dysplasia. Gastroenterology 1994; 107:288–96.
Orlowska J, Jarosz D, Pachlewski J, et al. Malignant transformation of benign epithelial gastric polyps. Am J Gastroenterol 1995; 90:2152–9.
Kamiya T, Morishita T, Asakura H, et al. Long-term follow-up study on gastric adenoma and its relation to gastric protruded carcinoma. Cancer 1982; 50:2496–503.
Lee JH, Park SJ, Abraham SC, et al. Frequent CpG island methylation in precursor lesions and early gastric adenocarcinomas. Oncogene 2004; 23:4646–54.
To KF, Leung WK, Lee TL, et al. Promoter hypermethylation of tumor-related genes in gastric intestinal metaplasia of patients with and without gastric cancer. Int J Cancer 2002; 102:623–8.
Leung WK, Yu J, Ng EK, et al. Concurrent hypermethylation of multiple tumor-related genes in gastric carcinoma and adjacent normal tissues. Cancer 2001; 91:2294–301.
Tamura G, Yin J, Wang S, et al. E-Cadherin gene promoter hypermethylation in primary human gastric carcinomas. J Natl Cancer Inst 2000; 92:569–73.
An C, Choi IS, Yao JC, et al. Prognostic significance of CpG island methylator phenotype and microsatellite instability in gastric carcinoma. Clin Cancer Res 2005; 11:656–63.
Etoh T, Kanai Y, Ushijima S, et al. Increased DNA methyltransferase 1 (DNMT1) protein expression correlates significantly with poorer tumor differentiation and frequent DNA hypermethylation of multiple CpG islands in gastric cancers. Am J Pathol 2004; 164:689–99.
Sun Y, Deng D, You WC, et al. Methylation of p16 CpG islands associated with malignant transformation of gastric dysplasia in a population-based study. Clin Cancer Res 2004; 10:5087–93.
Park TJ, Cho YK Pail WK, et al. Methylation of O6-methyl guanine-DNA methyltransferase gene is associated significantly with K-ras mutation, lymph node invasion, tumor staging, and disease free survival in patients with gastric carcinoma. Cancer 2001; 92:2760–8.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
CHOI, IS., WU, TT. Epigenetic alterations in gastric carcinogenesis. Cell Res 15, 247–254 (2005). https://doi.org/10.1038/sj.cr.7290293
Issue Date:
DOI: https://doi.org/10.1038/sj.cr.7290293
Keywords
This article is cited by
-
E3 ubiquitin ligase RNF180 prevents excessive PCDH10 methylation to suppress the proliferation and metastasis of gastric cancer cells by promoting ubiquitination of DNMT1
Clinical Epigenetics (2023)
-
Gamma-glutamyltransferase 7 suppresses gastric cancer by cooperating with RAB7 to induce mitophagy
Oncogene (2022)
-
Mir-20a-5p induced WTX deficiency promotes gastric cancer progressions through regulating PI3K/AKT signaling pathway
Journal of Experimental & Clinical Cancer Research (2020)
-
Comparison of CDH1 Gene Hypermethylation Status in Blood and Serum among Gastric Cancer Patients
Pathology & Oncology Research (2020)
-
eIF4EBP3 was downregulated by methylation and acted as a tumor suppressor by targeting eIF4E/β-catenin in gastric cancer
Gastric Cancer (2020)
