
Abstract
Purpose
To assess the long-term outcomes from cataract surgery on self-rated health, and health-related quality of life (HRQOL) in a population-based older sample.
Methods
Participants of the Blue Mountains Eye Study at the baseline (n=3654), 5 (n=2335), and 10-year follow-up (n=1952) were interviewed and examined. Questionnaires included an assessment of self-rated health and HRQOL using the 36-item Short-Form Health Survey (SF-36). Incident cataract surgery was defined if participants had cataract surgery since baseline, and confirmed via lens photographic grading.
Results
There was no statistically significant difference in the proportions of participants who experienced a change in self-rated health between those who had incident cataract surgery (14.1% improvement; 29.1% deterioration) and non-surgical subjects (16.7% improvement; 27.0% deterioration). We found no association between incident cataract surgery and the odds for 10-year change in self-rated health, after multivariate adjustment. In contrast, participants who had incident cataract surgery had a significant improvement in the mean scores of ‘mental health’ domain of HRQOL (+1.60 vs−2.04, P=0.02) and in the mental component score (+1.43 vs−0.82, P=0.02) than participants who did not undergo surgery. Cataract surgery during follow-up had no significant influence on change in mean scores of other domains or in their physical component score of the SF-36 (−2.57 in participants who had incident surgery vs−2.29 in non-surgical participants, P=0.78).
Conclusions
We confirmed long-term improvement following cataract surgery in the mental but not in the physical domain of the SF-36 or in answers to a specific self-rated health question.
Similar content being viewed by others

Introduction
Positive cataract surgery outcome is indicated by improvement in visual function, visual acuity (VA), and in vision-related quality of life and have been well documented in clinical patients shortly after either first or second eye cataract surgery.1, 2 There are few reports, however, on long-term cataract surgery outcomes.
Self-rated health is a strong predictor of mortality.3, 4, 5 Reduced self-rated health and health-related quality of life (HRQOL) have both been associated with visual impairment,6, 7, 8 and visual impairment has consistently been documented to be associated with increased mortality in older persons.9, 10, 11 It is unclear whether the visual impairment–mortality association operates via poor self-rated health and whether cataract surgery to improve visual impairment results in improvements in self-rated health, and HRQOL in the long term. To the authors' knowledge, no population-based study has reported long-term cataract surgery outcomes on self-rated health and HRQOL. In this study, we sought to examine the relationship between changes in self-rated health and HRQOL after cataract surgery in the Blue Mountains Eye Study (BMES) cohort, after 10-year follow-up.
Materials and methods
The BMES is a population-based cohort study of common age-related eye diseases in older persons. Research was conducted according to the recommendations of the Declaration of Helsinki and was approved by the Western Sydney Area Human Research Ethics Committee.
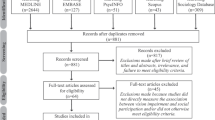
In 1991, a private door-to-door census identified 4433 eligible non-institutionalized permanent residents aged 49+ years living in a defined area, west of Sydney, Australia. During 1992–94 (BMES I), 3654 participants were examined (82.4% response). At 5-year follow-up examinations (1997–99, BMES II), 2335 (75.1% of survivors) were re-examined. Characteristics of participants in BMES I and II have been detailed previously.12 At 10-year follow-up examinations (2002–04, BMES III), 1952 (76.5% survivors) were re-examined. The details for the loss to follow-up between these examinations are provided in the flow diagram (Figure 1).

Number of participants at the baseline, 5- and 10-year follow-up examinations.
Participants were invited to attend a comprehensive eye examination that included measurement of presenting and best corrected VA using a Log MAR chart, after subjective refraction.12 For each eye, VA was recorded as the number of letters read correctly from 0 (<6/60) to 70 (6/3). The presence of cataract was assessed in each eye. Incident cataract surgery was confirmed by history and documented from slit-lamp (SL-7E photoslitlamp, Topcon Optical, Tokyo, Japan) and retroillumination (CT-R camera, Neitz Instruments, Tokyo, Japan) lens photographs.13
Standard questionnaires were administered by trained interviewers when participants attended the eye examinations. These included information on history of angina, acute myocardial infarct, hypertension, stroke, diabetes, cancer, arthritis, gout, thyroid conditions, falls, walking disability, hearing impairment, limitations in performing activities of daily living, and reliance on community services14 or any hospital admission within the last 12 months.15 Participants were questioned whether they rented or owned their own home, if they lived alone and which educational level had been achieved.
Self-rated health was assessed by asking a standard question with four possible answers: ‘For someone of your age, how would you rate your overall health – Would you say it is: excellent, good, fair, or poor?’ Change (decline or improvement) in self-rated health was defined if overall health rankings differed by one or more steps at 10-year follow-up.
The self-administered SF-36 (Short Form 36) was incorporated into the BMES II and III questionnaires only, and was mailed to participants after appointments were made. This instrument contains 36 items measuring eight domains of health and well-being: ‘physical functioning’, ‘role limitations due to physical problems’, ‘bodily pain’, ‘general health perceptions’, ‘vitality’, ‘social functioning’, ‘role limitations due to emotional problems’, and ‘mental health’. The Australian-adapted version was used in this study.16 Each domain was scored from 0 (worst possible health state) to 100 (best possible health state) by coding, summating, and transforming these relevant item scores according to the SF-36 manual.17 Physical and mental component scores (PCS and MCS, respectively) were summary measures derived using factor analysis and Australian-normalised scores (mean=50, SD=10).18, 19
We used the Statistical Analysis System (SAS V9.13; Cary, NC, USA), for analyses. Multivariable logistic regression analyses were performed to assess a change in self-rated health (dependent variable) for surgical and non-surgical participants during the 10-year follow-up period (explanatory variable). We adjusted for factors known to influence self-rated health: initially adjusting for age and sex, with further multivariable adjustment for the presence of at least two new conditions since the baseline examination, whether participants lived alone, home ownership, number of chronic conditions at baseline,20 recent admissions to hospital in the last 12 months,15 and presenting VA in the better eye at baseline. Participants (n=428) who rated their self-rated health as excellent were excluded when assessing improvement, and 29 who rated their self-rated health as poor were excluded when assessing deterioration. Participants (n=106) who had incomplete VA data or had cataract surgery before baseline were excluded from the analyses on self-rated health change. Odds ratios (OR) and 95% confidence intervals (CI) are presented. We used analysis of covariance (generalized linear model) to calculate mean changes in the SF-36 scores (dependent variable) between participants who had or did not have cataract surgery during the 5-year period between BMES II and III (explanatory variable). Negative scores in the changes indicated deterioration and positive scores indicated an improvement in HRQOL. Multivariate-adjusted mean differences in SF-36 scores were compared between participants who had cataract surgery (first eye, second eye or any) and those who did not have cataract surgery. Adjusted mean differences and P values for trend (Ptrend) are presented.
Results
Self-rated health
Participants had a mean age of 62.6 years at baseline (range 49–89 years) and 59.5% were women. There was no statistically significant difference in the proportions of participants whose self-rated health either improved or deteriorated by one or more steps between participants who had undergone (n=306, 14.1% improved; 29.1% deteriorated) and had not undergone cataract surgery (n=1540, 16.7% improved; 27.0% deteriorated) since the baseline examination; after adjusting initially for age and sex only, and additionally for other factors associated with self-rated health. Table 1 shows the OR for 10-year improvement or deterioration in self-rated health according to incident cataract surgery from BMES I to III.
SF-36 and HRQOL
Participants had a mean age of 67.4 years at baseline (range 54–94 years) and 58.8% were women. Increasing age was strongly associated with poorer SF-36 profiles. This age-related trend for worsening scores was demonstrated for all domains, including PCS and MCS, except for the ‘bodily pain’ and ‘social functioning’ categories (P<0.05, data not shown).
Table 2 shows the multivariate-adjusted difference in mean scores for the eight domains, PCS and MCS of the SF-36 between participants who had no incident cataract surgery, and those who had incident cataract surgery either on their first or second eye, during the 5-year interval between BMES II and III. There was a significant improvement in the ‘mental health’ domain among cataract surgical participants than non-surgical participants (+1.60 vs −2.04, P=0.02) and in the MCS (+1.43 vs −0.82, P=0.02). In addition, score improvements were significantly greater in the ‘mental health’ domain (+2.15 vs +0.79, Ptrend=0.01) and in the MCS (+1.61 vs +1.19, Ptrend=0.02) for participants who had second eye surgery compared to those who had first eye surgery.
Cataract surgery during the follow-up period had no significant influence on changes in scores of other domains or on the PCS of the SF-36, when comparing post BMES II surgical and non-surgical participants (−2.57 vs −2.29, P=0.78). Similarly, there was no difference in the changes in mean PCS scores between participants who had undergone second eye surgery and those who had first eye surgery (−2.59 vs −2.53, Ptrend=0.78).
Discussion
In this study, we assessed the long-term impact of cataract surgery on self-rated health and HRQOL in a population-based older sample. We could not identify a significant impact of cataract surgery on long-term changes in self-rated health. However, we found a positive impact of cataract surgery on the ‘mental health’ domain and the MCS of SF-36 HRQOL scores, components that were detrimentally influenced by increasingly severe visual impairment.21 We found no significant impact of cataract surgery on the remaining domains or on the PCS.
Global self-rated health is a multidimensional, conceptual measure, influenced by age, gender, race, education, and chronic disease.22, 23, 24 We have previously reported a cross-sectional association between low vision and low self-rated health,8 but could not demonstrate a longitudinal effect of change in vision on subsequent change in self-rated health.21 Our failure in this study to document a parallel association of cataract surgery (to improve vision) with temporal changes in self-rated health could be due to a relatively low impact from reduced vision (and hence restoration by cataract surgery) on the ranking of global perception of health in older persons, compared to other age-related chronic conditions.
The SF-36 is a generic, multidimensional questionnaire that has been used broadly across various populations, treatment groups, and diseases including a wide range of ophthalmic conditions.25, 26, 27 Generic health outcome measures are considered not to be as sensitive to changes in vision-related function as vision-function-specific questionnaires.26, 27 However, the SF-36 has been shown to discriminate well between older persons with and without a number of health conditions including increasingly severe non-correctable visual impairment in the BMES,21, 28 making this instrument appropriate for the purposes of this report.29 In the BMES population, we found that the mental domains were more largely affected by visual impairment than the physical domains.21, 28 When age- and sex-adjusted PCS and MCS scores were compared using World Health Organisation disability weights, the impact of visual impairment on the mental domain was greater than that from many other medical conditions.21 Changes in SF-36 scores that differ between groups by two or more points on the scale of 0 to 100 have been shown to be socially or clinically meaningful.30 Our findings of a statistically significant improvement in the mental domains, namely the ‘mental health’ and MCS score after cataract surgery, are in keeping with our previous findings,21, 28 and suggests that surgical correction of visual impairment improves HRQOL in the long term.
Our findings have two important implications. First, if we assign equal weighting for the physical and the mental components in the calculation of disability weights, the improvement in HRQOL after cataract surgery is comparable to interventions aimed at improving HRQOL for other major medical conditions, despite differences in the domains from which these weights were derived. Second, we found that an improvement in ‘mental health’ was more than double in participants who had second eye cataract surgery compared to those who had only first eye surgery. This trend was also present, though modest, for the MCS. These findings are consistent with studies reporting a range of visual and functional benefits from second eye cataract surgery.31, 32, 33 Talbot and Perkins33 reported that the proportion of older people satisfying driving licence requirements improved from 52 to 86% after second eye surgery.
Strengths of this study include its population-based sample, a long-term follow-up period with repeated HRQOL measures collected over time and the relatively high completion rate of the SF-36 questionnaire (89.9%) by participants.28 Although our findings are relatively consistent with previous findings from clinic-based samples, the possibility of incomplete adjustment of confounding factors and chance findings are limitations.
In summary, we provide evidence from an older population-based sample to support the notion that cataract surgery performed in one or both eyes provides long-term benefits in the mental domain of HRQOL in older persons, presumably secondary to the correction of visual impairment.
References
Steinberg EP, Tielsch JM, Schein OD, Javitt JC, Sharkey P, Cassard SD et al. National study of cataract surgery outcomes. Variation in 4-month postoperative outcomes as reflected in multiple outcome measures. Ophthalmology 1994; 101: 1131–1140.
Brenner MH, Curbow B, Javitt JC, Legro MW, Sommer A . Vision change and quality of life in the elderly. Response to cataract surgery and treatment of other chronic ocular conditions. Arch Ophthalmol 1993; 111: 680–685.
Mossey JM, Shapiro E . Self-rated health: a predictor of mortality among the elderly. Am J Public Health 1982; 72: 800–808.
Idler EL, Benyamini Y . Self-rated health and mortality: a review of twenty-seven community studies. J Health Soc Behav 1997; 38: 21–37.
Kaplan GA, Camacho T . Perceived health and mortality: a nine-year follow-up of the human population laboratory cohort. Am J Epidemiol 1983; 117: 292–304.
Wang JJ, Mitchell P, Simpson JM, Cumming RG, Smith W . Visual impairment, age-related cataract and mortality. Arch Ophthalmol 2001; 119: 1186–1190.
Taylor HR, McCarty CA, Nanjan MB . Vision impairment predicts five-year mortality. Trans Am Ophthalmol Soc 2000; 98: 91–96.
Wang JJ, Mitchell P, Smith W . Vision and low self-rated health: the Blue Mountains Eye Study. Invest Ophthalmol Vis Sci 2000; 41: 49–54.
Klein R, Klein BE, Moss SE . Age-related eye disease and survival. The Beaver Dam Eye Study. Arch Ophthalmol 1995; 113: 333–339.
McCarty CA, Nanjan MB, Taylor HR . Vision impairment predicts 5 year mortality. Br J Ophthalmol 2001; 85: 322–326.
Knudtson MD, Klein BE, Klein R . Age-related eye disease, visual impairment, and survival: the Beaver Dam Eye Study. Arch Ophthalmol 2006; 124: 243–249.
Attebo K, Mitchell P, Smith W . Visual acuity and the causes of visual loss in Australia. The Blue Mountains Eye Study. Ophthalmology 1996; 103: 357–364.
Mitchell P, Cumming RG, Attebo K, Panchapakesan J . Prevalence of cataract in Australia: the Blue Mountains Eye Study. Ophthalmology 1997; 104: 581–588.
Wang JJ, Mitchell P, Smith W, Cumming RG, Attebo K . Impact of visual impairment on use of community support services by elderly persons: the Blue Mountains Eye Study. Invest Ophthalmol Vis Sci 1999; 40: 12–19.
Kim SH, Wolde-Tsadik G, Reuben DB . Predictors of perceived health in hospitalized older persons: a cross-sectional and longitudinal study. J Am Geriatr Soc 1997; 45: 420–426.
Sanson-Fisher RW, Perkins JJ . Adaptation and validation of the SF-36 Health Survey for use in Australia. J Clin Epidemiol 1998; 51: 961–967.
Ware JE, Snow KK, Kosinski M, Gande B . SF-36 health survey. Manual and interpretation guide. The Health Institute, New England Medical Center: Boston, MA, 1993.
Ware JE, Kosinski M, Keller SD . SF-36 Physical and Mental Health Summary Scales. The Health Institute, New England Medical Center: Boston, MA, 1994.
ABS. National Health Survey. SF-36 Population Norms. Australia (4399.0). ABS: Canberra, 1997.
Rodin J, McAvay G . Determinants of change in perceived health in a longitudinal study of older adults. J Gerontol 1992; 47: 373–384.
Chia EM, Wang JJ, Rochtchina E, Smith W, Cumming RG, Mitchell P . Impact of bilateral visual impairment on health-related quality of life: the Blue Mountains Eye Study. Invest Ophthalmol Vis Sci 2004; 45: 71–76.
Krause NM, Jay GM . What do global self-rated health items measure? Med Care 1994; 32: 930–942.
Smith AM, Shelley JM, Dennerstein L . Self-rated health: biological continuum or social discontinuity? Soc Sci Med 1994; 39: 77–83.
Shadbolt B . Some correlates of self-rated health for Australian women. Am J Public Health 1997; 87: 951–956.
Ware JE Jr, Sherbourne CD . The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 1992; 30: 473–483.
Scott IU, Smiddy WE, Schiffman J, Feuer WJ, Pappas CJ . Quality of life of low-vision patients and the impact of low-vision services. Am J Ophthalmol 1999; 128: 54–62.
Parrish RK, Gedde SJ, Scott IU, Feuer WJ, Schiffman JC, Mangione CM et al. Visual function and quality of life among patients with glaucoma. Arch Ophthalmol 1997; 115: 1447–1455.
Chia EM, Mitchell P, Rochtchina E, Foran S, Wang JJ . Unilateral visual impairment and health related quality of life: the Blue Mountains Eye Study. Br J Ophthalmol 2003; 87: 392–395.
McCallum J . The New ‘SF-36’ Health Status Measure: Australian Validity Tests 1-11. National Centre for Epidemiology and Population Health, The Australian National University: Canberra, 2002.
Bacon CG, Giovannucci E, Testa M, Glass TA, Kawachi I . The association of treatment-related symptoms with quality-of-life outcomes for localized prostate carcinoma patients. Cancer 2002; 94: 862–871.
Javitt JC, Steinberg EP, Sharkey P, Schein OD, Tielsch JM, Diener M et al. Cataract surgery in one eye or both. A billion dollar per year issue. Ophthalmology 1995; 102: 1583–1592.
Laidlaw DA, Harrad RA, Hopper CD, Whitaker A, Donovan JL, Brookes ST et al. Randomised trial of effectiveness of second eye cataract surgery. Lancet 1998; 352: 925–929.
Talbot EM, Perkins A . The benefit of second eye cataract surgery. Eye 1998; 12 (Part 6): 983–989.
Author information
Authors and Affiliations
Corresponding author
Additional information
Proprietary interest: none for all authors
Rights and permissions
About this article
Cite this article
Chandrasekaran, S., Wang, J., Rochtchina, E. et al. Change in health-related quality of life after cataract surgery in a population-based sample. Eye 22, 479–484 (2008). https://doi.org/10.1038/sj.eye.6702854
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6702854
Keywords
This article is cited by
-
A longitudinal analysis of factors associated with age-related cataract among older Australian women: a cohort study of 7851 older Australian women 79–90 years
Irish Journal of Medical Science (1971 -) (2023)
-
Application of Andersen–Newman model to assess cataract surgery uptake among older Australian women: findings from the Australian Longitudinal Study on Women’s Health (ALSWH)
Aging Clinical and Experimental Research (2022)
-
Correlation among Lens Opacities Classification System III grading, the 25-item National Eye Institute Visual Functioning Questionnaire, and Visual Function Index-14 for age-related cataract assessment
International Ophthalmology (2020)
-
Catquest-9SF questionnaire: validation of Malay and Chinese-language versions using Rasch analysis
Health and Quality of Life Outcomes (2018)
-
Cataract
Nature Reviews Disease Primers (2015)
