
Abstract
Purpose
Ocular perfusion abnormalities have been proposed in the pathogenesis of age-related macular degeneration (AMD) with differences in pulsatile ocular blood flow (POBF) in eyes with asymmetric AMD in Japanese and Taiwanese patients. The purpose of our study was to observe POBF difference in the fellow eyes of Caucasians with asymmetric AMD.
Methods
This was a cross-sectional study comparing POBF in three groups of patients with asymmetric AMD in the fellow eyes: Group 1 (n=21) with drusen and active choroidal neovascularisation (CNV); Group 2 (n=18) with drusen and disciform scar; Group 3 (n=8) with CNV and disciform scar. The POBF was adjusted for intraocular pressure (IOP), pulse rate (PR), and axial length using multiple regression analysis. Generalised estimation equation model was used to include both eyes in each group.
Results
The geometric mean (95% confidence interval) POBF values were as follows: Group 1with drusen 1097.9 μl/min (957.0, 1259.7) in one eye and the fellow eye with CNV 1090.1 μl/min (932.3, 1274.7); Group2 with drusen 946.0 μl/min (794.2, 1126.7) and disciform scar 966.2 μl/min (780.3, 1196.4); Group3 with CNV 877.1 μl/min (628.3, 1224.6) and disciform scar 767.2 μl/min (530.5, 1109.7). Adjusting for differences in axial length, pulse rate and intraocular pressure, no statistically significant difference in POBF was found between fellow eyes in the same subject.
Conclusions
POBF is not different between fellow eyes of Caucasian patients with asymmetric AMD.
Similar content being viewed by others


Introduction
Age-related macular degeneration (AMD) is the leading cause of severe visual loss in patients above the age of 50 years in industrialised countries. 1, 2, 3 It is a heterogenous disorder and is broadly classified into nonexudative or dry type, and exudative or wet type. Despite its high prevalence and public health impact, the aetiology of AMD remains largely unknown. Various studies have investigated the possible aetiological mechanisms of pathogenesis of AMD, suggesting genetic predisposition,4, 5, 6 retinal pigment epithelial (RPE) senescence,7, 8 oxidative stress,9 local inflammation or immunological stimuli,10, 11 and haemodynamic abnormalities.12, 13
Ocular perfusion abnormalities in relation to AMD have been studied in the past using various techniques. Pulsatile ocular blood flow (POBF) reflects the total pulsatile component of ocular blood flow. The pulsatile component of the total blood flow ranges from 50 to 80%.14 As most of the ocular blood volume is present in the choroid, the retina contributes very little to the pulsatile component, which is thought to mainly represent the choroidal circulation. It is measured by a pneumotonometer based on a pressure volume relationship as demonstrated originally by the Langham OBF System.15 This provides a noninvasive, reliable, reproducible, and inexpensive method of calculating the average POBF from the IOP. POBF may be influenced by various factors such as age, sex, blood pressure, scleral rigidity, refractive error, and axial length. However, a recent study evaluating these factors found axial length to be the only statistically significant factor influencing POBF in normal subjects.16
A group-wise comparison between exudative AMD, nonexudative AMD and age-matched controls in a Japanese cohort showed significant decrease in POBF in exudative AMD.17 In addition, significant difference in POBF was found between eyes in asymmetric AMD in a Taiwanese group.18 The POBF was found to be higher in eyes with choroidal neovascularisation (CNV) than in fellow eyes with drusen, suggesting a role for haemodynamic abnormalities in the development and progression of AMD. However, it is well documented that there are racial variations in the risk factors19 and prevalence20, 21 of AMD. The aim of our study was to determine whether ocular blood flow disturbances in fellow eyes with asymmetric AMD, using the POBF method, in Caucasian subjects play a significant role in a racially different sample population, and to correlate these changes with disease activity.
Materials and methods
Methods
The study subjects underwent assessment of best corrected logmar visual acuity, slit-lamp biomicroscopy, fundus photography, fluorescein angiography, and axial length measurements using the IOL Master (Zeiss) based on the principle of laser interferometry.
POBF was measured using the OBF Analyser (Ocular Blood Flow Analyser, Dicon Diagnostics, Paradigm, USA). Subjects were assessed in the sitting position by the same examiner who was masked to the diagnosis in each eye. The measurements were taken with a mounted probe after instillation of topical anaesthetic (0.5% proxymetacaine). POBF values were calculated and expressed as a mean of measurements taken from five representative pulses.
This study was ethically approved by the Central Office for Research and Ethics Committees (COREC), UK. All procedures adhered to the tenets of the Declaration of Helsinki.
Patients
The inclusion criteria were as follows: age ≥50 years; Caucasian; evidence of asymmetric AMD. Exudative AMD included active CNV and disciform scar. The International Classification and Grading of AMD nomenclature22 was used for the definition of active CNV, disciform scar, and age-related maculopathy (stage 2a–3 as per Rotterdam study criteria).23 The CNV lesions were defined as classic, occult, or mixed as per TAP study criteria.24
Grading of the digital colour photographs and fluorescein angiograms was performed by two independent graders from King's College Hospital. Double grading for intraobserver and interobserver variability was performed. Discrepancies were resolved by the senior author.
The patients were divided into three groups based on the findings of slit-lamp biomicroscopy, fundus photography, and fluorescein angiography:
-
a)
Group 1, patients with early age-related maculopathy (ARM) that is, drusen in one eye and active CNV in the fellow eye.
-
b)
Group 2, ARM (drusen) in one eye and disciform scar in the fellow eye.
-
c)
Group 3, active CNV in one eye and disciform scar in the fellow eye.
Exclusion criteria were as follows: high myopia, history of any associated ocular conditions such as coexistent glaucoma, diabetic retinopathy, vascular disorders including hypertensive retinopathy, and veno-occlusive disease.
Statistical analysis
There was good intergrader agreement as assessed by Cohen's kappa statistics (κ=0.8). The distribution of POBF values was assessed and found to be positively skewed. Log transformation normalised the data (Shapiro Wilks test for normality P=0.37). Geometric means and confidence intervals (CI) were calculated. Paired Student's t-test was used to compare differences in geometric means of POBF between fellow eyes of the same subject. Multivariate linear regression analysis with log transformed POBF as the dependant variable was used to adjust for differences in axial length, IOP, and PR. To allow for dependence in the data because of the study of two eyes in one subject, a generalised estimation equation model of variance analysis was used. Tests are two-sided with CI quoted at 95%.
Results
In total, 47 subjects with asymmetric AMD in the fellow eye were included in the study. The demographic details of subjects are given in Table 1. No statistically significant difference in age or sex was noted between the groups.
The geometric mean POBF (CI) in the three groups is shown in Table 2. After adjusting for the differences in IOP, PR, and axial length, there was no statistically significant difference between fellow eyes in the three groups. Although the active CNV lesions were defined as classic, occult, or mixed, further subgroup analysis did not show a statistically significant difference in POBF between these three subgroups.
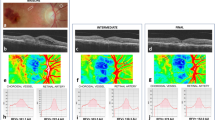
Figures 1, 2 and 3 show POBF values in the fellow eyes in each of the three groups with asymmetric AMD.

Pulsatile ocular blood flow in patients with drusen and CNV.

Pulsatile ocular blood flow in patients with drusen and disciform lesions.

Pulsatile ocular blood flow in patients with CNV and disciform lesions.
Discussion
The results of our study show that there is no significant difference in POBF between fellow eyes in asymmetric AMD. We were particularly interested in the Groups 1 and 2 as a difference in POBF between fellow eyes in these groups would aid in early detection of cases with an increased risk for developing CNV. When looking at the unadjusted values, differences in Group 3 achieved statistical significance. However, this difference was not significant after differences in IOP, PR, and axial length were taken into account. The major drawback is relatively few numbers in this particular group. However, this group has little implication for clinical usefulness in terms of disease management as both eyes had progressed to the advanced stage of the disease. Therefore, despite small patient numbers, further recruitment for study purposes was not deemed appropriate.
Two studies have investigated ocular haemodynamic abnormalities in AMD using the POBF technique. The results of both these studies are difficult to compare. Mori et al17 compared POBF between single eyes of Japanese subjects with exudative AMD (11 eyes) , nonexudative AMD (10 eyes), and age-matched healthy controls (69 eyes). The results were expressed as median, with POBF being significantly lower in exudative as than in nonexudative AMD (P=0.02) and healthy controls (P=0.01). No significant difference was noted between nonexudative AMD and controls.
Whereas this study made a group-wise interindividual comparison, Chen et al18 used a paired sample comparison and investigated POBF difference in a Taiwanese cohort with asymmetric AMD between fellow eyes of the same subject, thus eliminating high interindividual variation in POBF.25 As the methodology was similar to this study, it enabled us to compare the blood flow characteristics in the two racial groups: Caucasians vs Taiwanese. In the Taiwanese cohort, the mean value of POBF, after adjusting for IOP and PR, was significantly lower in the eyes with drusen than in fellow eyes with CNV but higher than that in fellow eyes with disciform scar. However, despite the methodology of this study being similar to ours, no correction of POBF for axial length was made. Although the comparison of these two studies seems reasonable at first, this limitation must be taken into account before the interpretation of results. The results are also in contrast to the findings of our study in which the mean POBF, although not statistically significant, was found to be higher in eyes with drusen than in fellow eyes with CNV, but lower than that in fellow eyes with disciform scar. There may not actually be a difference between the Chen study and this one, given the difference in analysis in the studies (axial length correction).
Interestingly, several epidemiological studies26 have observed significant variation in the prevalence of AMD among different racial/ethnic groups and in different parts of the world. Oshima et al reported a lower prevalence of early and late stage ARM among Japanese than among Caucasians, whereas late stage ARM was found to be more common among Japanese than among Afro-Caribbeans. Another study by Uyama et al evaluated the incidence of CNV and predisposing findings for the development of CNV in the second eye of Japanese patients with unilateral exudative AMD. There was a variation in the prevalence of soft drusen and pigmentary change, and a low incidence of the development of CNV in the fellow eye as compared to that in the white population. This may explain the difference in our results as the Taiwanese group had lower mean POBF in the drusen eyes as than in the fellow eyes with CNV. This is in contrast to a higher mean POBF found in Caucasian eyes with drusen than in fellow eyes with CNV. This would arguably be in keeping with the observation of a higher incidence of the development of CNV in the second eyes of Caucasians as observed by previous studies.
Previous studies have suggested morphological changes in the choroidal vasculature with a reduction in blood flow, in subjects with various stages of AMD, with most of them suggesting focal choroidal perfusion abnormalities in both non-neovascular and neovascular AMD. Whereas 37% decrease in subfoveal choroidal blood flow compared to that of a control group has been demonstrated in non-neovascular AMD using laser Doppler flowmetry (LDF),12 studies on neovascular AMD by Schmetterer et al,27 have shown lower topical fundus pulsation amplitudes in patients with CNV using the laser interferometric method.27 The authors postulated this to be because of focal choroidal perfusion abnormalities. A recent study also suggested a decreasing trend in the choroidal blood flow with increasing severity of the disease. Grunwald28 compared foveolar choroidal blood flow in three groups according to increasing risk for the development of CNV. Group 1 drusen >63 μ in the study eye and no CNV in the fellow eye; Group 2 drusen >63 μ and RPE hypertrophy in the study eye and no CNV in the fellow eye; Group 3 eyes with CNV in the fellow eye. Subfoveal choroidal blood flow was assessed using the laser Doppler flowmeter. A systematic decrease in choroidal circulatory parameters was observed with an increase in severity of AMD features associated with a risk for development of CNV. This study again looked at focal changes in the foveolar blood flow.
As mentioned previously, POBF reflects the total pulsatile component of ocular blood flow and most of this blood volume is present mainly in the choroid. Therefore, the POBF technique estimates the average global choroidal blood flow. As our study used this technique, a plausible explanation for similar POBF values in fellow eyes with asymmetric AMD may be that global alterations in ocular perfusion in AMD may not be significant in the pathogenesis and progression of this severely sight threatening disease.
Conclusion
The result of our study demonstrated no significant difference of POBF in the fellow eyes of Caucasian patients with asymmetric AMD, particularly with early ARM in one eye and exudative AMD in the fellow eye. Further studies on POBF comparing racial groups and use of techniques aimed at assessing focal choroidal blood flow may help improve our understanding of ocular haemodynamic abnormalities and their implications in the development and progression of AMD.
References
Klein R, Klein BE, Tomany SC, Meuer SM, Huang GH . Ten-year incidence and progression of age-related maculopathy: The Beaver Dam eye study. Ophthalmology 2002; 109(10): 1767–1779.
van Leeuwen R, Klaver CC, Vingerling JR, Hofman A, de Jong PT . The risk and natural course of age-related maculopathy: follow-up at 6 1/2 years in the Rotterdam study. [erratum appears in Arch Ophthalmol. 2003; 121(7): 955]. Arch Ophthalmol 2003; 121(4): 519–526.
Wang JJ, Foran S, Smith W, Mitchell P . Risk of age-related macular degeneration in eyes with macular drusen or hyperpigmentation: the Blue Mountains Eye Study cohort. Arch Ophthalmol 2003; 121(5): 658–663.
Heiba IM, Elston RC, Klein BE, Klein R . Sibling correlations and segregation analysis of age-related maculopathy: the Beaver Dam Eye Study. [erratum appears in Genet Epidemiol 1994; 11(6): 571]. Genet Epidemiol 1994; 11(1): 51–67.
Klein ML, Schultz DW, Edwards A, Matise TC, Rust K, Berselli CB et al. Age-related macular degeneration. Clinical features in a large family and linkage to chromosome 1q. Arch Ophthalmol 1998; 116(8): 1082–1088.
Allikmets R . Further evidence for an association of ABCR alleles with age-related macular degeneration. The International ABCR Screening Consortium. Am J Hum Genet 2000; 67(2): 487–491.
Eagle Jr RC . Mechanisms of maculopathy. Ophthalmology 1984; 91(6): 613–625.
Young RW . Pathophysiology of age-related macular degeneration. Surv Ophthalmol 1987; 31(5): 291–306.
Beatty S, Koh H, Phil M, Henson D, Boulton M . The role of oxidative stress in the pathogenesis of age-related macular degeneration. Surv Ophthalmol 2000; 45(2): 115–134.
Hageman GS, Luthert PJ, Victor Chong NH, Johnson LV, Anderson DH, Mullins RF . An integrated hypothesis that considers drusen as biomarkers of immune-mediated processes at the RPE-Bruch's membrane interface in aging and age-related macular degeneration. Prog Ret Eye Res 2001; 20(6): 705–732.
Penfold PL, Madigan MC, Gillies MC, Provis JM . Immunological and aetiological aspects of macular degeneration. Prog Ret Eye Res 2001; 20(3): 385–414.
Grunwald JE HS, DuPont J, Maguire MG, Fine SL, Brucker AJ, Maguire AM et al. Foveolar choroidal blood flow in age-related macular degeneration. Invest Ophthalmol Vis Sci 1998; 39(2): 385–390.
Friedman E . A haemodynamic model of the pathogenesis of age-related macular degeneration. Am J Ophthalmol 1997; 124(5): 677–682.
Langham ME, Farrell RA, O'Brien V, Silver DM, Schilder P . Blood flow in the human eye. Acta Ophthalmol Suppl 1989; 191: 9–13.
Silver DM, Farrell RA, Langham ME, O'Brien V, Schilder P . Estimation of pulsatile ocular blood flow from intraocular pressure. Acta Ophthalmol Suppl 1989; 191: 25–29.
Mori F, Konno S, Hikichi T, Yamaguchi Y, Ishiko S, Yoshida A . Factors affecting pulsatile ocular blood flow in normal subjects. Br J Ophthalmol 2001; 85(5): 529–530.
Mori F, Konno S, Hikichi T, Yamaguchi Y, Ishiko S, Yoshida A . Pulsatile ocular blood flow study: decreases in exudative age related macular degeneration. Br J Ophthalmol 2001; 85(5): 531–533.
Chen SJ, Cheng CY, Lee AF, Lee FL, Chou JC, Hsu WM et al. Pulsatile ocular blood flow in asymmetric exudative age related macular degeneration. Br J Ophthalmol 2001; 85(12): 1411–1415.
Miyazaki M, Nakamura H, Kubo M, Kiyohara Y, Oshima Y, Ishibashi T et al. Risk factors for age related maculopathy in a Japanese population: the Hisayama study. Br J Ophthalmol 2003; 87(4): 469–472.
Oshima Y, Ishibashi T, Murata T, Tahara Y, Kiyohara Y, Kubota T . Prevalence of age related maculopathy in a representative Japanese population: the Hisayama study. Br J Ophthalmol 2001; 85(10): 1153–1157.
Yuzawa M, Tamakoshi A, Kawamura T, Ohno Y, Uyama M, Honda T . Report on the nationwide epidemiological survey of exudative age-related macular degeneration in Japan. Int Ophthalmol 1997; 21(1): 1–3.
Bird AC, Bressler NM, Bressler SB, Chisholm IH, Coscas G, Davis MD et al. An international classification and grading system for age-related maculopathy and age-related macular degeneration. The International ARM Epidemiological Study Group. Surv Ophthalmol 1995; 39(5): 367–374.
Klaver CC, Assink JJ, van Leeuwen R, Wolfs RC, Vingerling JR, Stijnen T et al. Incidence and progression rates of age-related maculopathy: the Rotterdam Study. Invest Ophthalmol Vis Sci 2001; 42(10): 2237–2241.
Blinder KJ, Bradley S, Bressler NM, Bressler SB, Donati G, Hao Y et al. Effect of lesion size, visual acuity, and lesion composition on visual acuity change with and without verteporfin therapy for choroidal neovascularization secondary to age-related macular degeneration: TAP and VIP report no. 1. Am J Ophthalmol 2003; 136(3): 407–418.
Yang YC, Hulbert MF, Batterbury M, Clearkin LG . Pulsatile ocular blood flow measurements in healthy eyes: reproducibility and reference values. J Glaucoma 1997; 6(3): 175–179.
Klein R, Peto T, Bird A, Vannewkirk MR . The epidemiology of age-related macular degeneration. Am J Ophthalmol 2004; 137(3): 486–495.
Schmetterer LKA, Findl O, Breiteneder H, Eichler HG, Wolzt M . Topical fundus pulsation measurements in age-related macular degeneration. Graefes Arch Clin Exp Ophthalmol 1998; 236(3): 160–163.
Grunwald JE, Metelitsina TI, Dupont JC, Ying GS, Maguire MG . Reduced foveolar choroidal blood flow in eyes with increasing AMD severity. Invest Ophthalmol Vis Sci 2005; 46(3): 1033–1038.
Acknowledgements
The authors did not receive any additional financial support from public or private sources.
The authors have no proprietary interest in this study.
Author information
Authors and Affiliations
Corresponding author
Additional information
This work has been presented as a poster at the European association for Vision and Eye Research, Vilamoura, Portugal in September 2004
Rights and permissions
About this article
Cite this article
Sandhu, R., Sivaprasad, S., Shah, S. et al. Pulsatile ocular blood flow in asymmetric age-related macular degeneration. Eye 21, 506–511 (2007). https://doi.org/10.1038/sj.eye.6702242
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6702242
Keywords
This article is cited by
-
Ocular pulse amplitude and retinal vessel caliber changes after intravitreal ranibizumab
International Ophthalmology (2015)
