
Abstract
Purpose
To determine the association between hospital and surgeon volume with the incidence of postoperative endophthalmitis.
Methods
A prospective cohort study was conducted to analyse the national health insurance claims data of those patients receiving cataract surgery in 2000 in Taiwan. A total of 108 705 patients who received cataract surgery by 1004 surgeons at 494 hospitals were followed to the end of 2002. Stepwise Cox regression was used to analyse the effects of hospital and surgeon volume of cataract surgery on postoperative endophthalmitis after adjustment for patient's age, gender, education, ophthalmic comorbidities, general comorbidities, and surgical factors including operative methods, different types of intraocular lenses, and surgeon's age.
Results
The 2-year incidence of postoperative endophthalmitis at high-volume hospitals (0.90%) was lower than low-volume hospitals (1.16%). The incidence of postoperative endophthalmitis by high-volume surgeons (0.59%) was lower than those by middle-high-volume (0.73%), middle-low-volume (0.80%), or low-volume surgeons (1.16%). After controlling for case mix, the risk of postoperative endophthalmitis of the low-volume hospitals (hazard ratio (HR)=1.39) was higher than that of the high-volume hospitals. The risk of postoperative endophthalmitis of low-volume surgeons (HR=1.67) was higher than that of the high-volume surgeons.
Conclusions
The provider volume (hospital and surgeon volume) is associated with the risk of postoperative endophthalmitis. The patients who receive cataract surgery at low-volume hospitals or by low-volume surgeons have significantly higher risk of postoperative endophthalmitis than at high-volume hospitals or by high-volume surgeons. Provider volume can be considered in further postoperative endophthalmitis study as a risk factor.
Similar content being viewed by others

Introduction
Although cataract surgery is the most effective, common, and safe ophthalmic procedure to treat cataract,1, 2, 3 the complications of cataract surgery may result in blindness and thus ruin the patient's quality of life. For the safety of patients, it is very important to monitor and improve the quality of cataract surgery.
Many studies have shown that, in the past two decades, the hospital and surgeon volume are closely associated with better surgical outcome with lower postoperative complications or mortalities, such as paediatric cardiac surgery,4 repair of abdominal aortic aneurysm,5 coronary artery bypass graft surgery,6 ventriculo-peritoneal shunt procedures,7 total hip replacement surgery,8 and colon cancer surgery.9 However, only few studies reported the relationship between provider volume and the incidence of postoperative endophthalmitis.10 Therefore, this study was designed to investigate the association of provider volume with postoperative endophthalmitis after controlling the confounding factors by using nationwide data.
Materials and methods
Database and patients
The data of this study were obtained from the Bureau of National Health Insurance (BNHI) programme, which started on 1 March 1995 to meet the demand for public health care. The programme covers about 21 million people, which is 96.16% of the whole population in Taiwan. All medical institutions must submit their medical charges in standard claim documents consisting of a computerised form carrying each beneficiary's unique identification number, age, sex, date of admission, date of discharge, date of outpatient visit, discharge status, and amount reimbursed. The claim form includes up to five diagnoses for in-patient and three diagnoses for outpatient, and up to five operation codes for in-patient and one operation code for outpatient following the International Classification of Diseases, Ninth Revision, clinical modification (ICD-9 CM). The database also includes the codes for treatment procedures, such as methods of operation and anaesthesia, and types of implanted intraocular lenses (IOLs). Data from death registration were used to obtain information on deaths. Data from permanent resident registration were used to obtain information on education level. Information on contracted medical facilities (public or private hospitals) and surgeon factors (age and sex) was obtained from the government's Department of Health.
Patients recruited in this study were those that received cataract surgery during the period from 1 January to 31 December 2000. All cases with the cataract case payment system code (97605K, 97606A, 97607B, 97608C, 97601K, 97602A, 97603B) and payment code for cataract surgery (86008C) indicative of having undergone cataract surgery were identified. Patients who had undergone cataract surgery combined with other intraocular procedures including corneal transplant, glaucoma filtering surgery, vitreous or retinal operations, suture for corneal and/or scleral lacerations, and removal of eyeballs were excluded. In total, 108 705 patients were continually followed until the end of 2002.
The identification of postoperative endophthalmitis was based on the diagnosis code of endophthalmitis as in Morlet's study9 (ICD-9 CM code 360.00∼360.04, 360.11∼360.19) at the same admission for index cataract surgery, at subsequent admission, or at outpatient visits. If the patients underwent any intraocular surgery unrelated to the treatment of endophthalmitis after cataract surgery, they would be withdrawn from follow-up (censored) to avoid incorrect attribution of complication to the index cataract surgery. If the patients had died before the end of the follow-up, they were withdrawn from the study on the date of their death.
Ophthalmic and medical comorbidities were identified by the diagnosis codes (principle and secondary) from the medical records 6 months before the index cataract surgery. The ophthalmic comorbidities included glaucoma, choroid disorders, uveitis, ocular trauma, dry eye, keratitis, background diabetic retinopathy, proliferative diabetic retinopathy, and nonsenile cataract. The medical comorbidities included diabetes, hypertension, lung diseases (chronic obstructive lung disease, asthma, external agent-induced lung diseases), inflammatory arthropathies, severe psychotic disorders (organic psychotic conditions and other psychoses), and mild psychiatric disorders (neurotic disorders, personality disorders, and other nonpsychotic mental psychoses).
Surgical methods were identified by ICD-9 CM code as in Javitt's report,11 including extracapsular cataract extraction (ECCE), intracapsular cataract extraction (ICCE), phacoemulsification (PE), and other methods. A cataract surgery has two surgical codes; one is the extraction code (ICD-9CM code 13.1∼13.6, 13.8, 13.9) and the other is the implantation code (ICD-9CM code 13.7). As the claim data have only one operation code for outpatient cataract surgery, patients' operative method can be identified when this one code is extraction code. Anaesthesia method of cataract surgery was identified by procedure code and divided as general anaesthesia (GA) and local anaesthesia (LA). The LA included retrobulbar, peribulbar, topical anaesthesia, and other anaesthesia methods. Types of IOL were grouped into PMMA (polymethylmethacrylate), heparin surface modification PMMA (HSM PMMA), acrylic, and silicone.
Statistical analysis
We divided the patients into four near equal size groups according to the hospital's annual volume of cataract surgery: high-volume hospital (quartile 4, as reference group), middle-high-volume hospital (quartile 3), middle-low-volume hospital (quartiles 2), and low-volume hospital (quartile 1). The patients were also divided into four near equal size groups according to the surgeon's annual volume of cataract surgery: high-volume surgeon (quartile 4, as reference group), middle-high-volume surgeon (quartile 3), middle-low-volume surgeon (quartiles 2), and low-volume surgeon (quartile 1). The possible risk factors such as patient's factors (age, gender, education, ophthalmic comorbidities, and medical comorbidities), surgical factors (site of operation, methods of operation, material of intraocular lenses), hospital factors (ownership status), and surgeon factors (age of surgeon) that related to the incidence of endophthalmitis were controlled in this study.
The number and percentage of 2-year postoperative endophthalmitis were calculated and divided into different volume groups. χ2 test was used to evaluate the differences among these four volume groups. Stepwise Cox regression analysis was applied to analyse the relationship between postoperative endophthalmitis and surgical volume. The hospital and surgeon volumes were analysed with separate regression models due to the positive association between these two volume strata.
All the analysis was conducted using SAS (Statistical Analysis Systems, Cary, NC, USA) software version 8.02.
Results
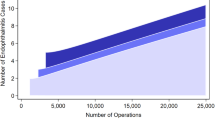
A total of 108 705 patients who received cataract surgery performed by 1004 surgeons at 494 separate hospitals during 2000 were studied (Table 1). The mean numbers and range of operations per year for each volume strata were shown, respectively.
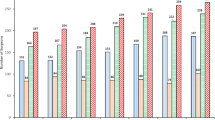
The characteristics of patient factors and surgical factors are shown in Table 2. Totally, 45.9% of patients were male and 54.0% of patients were female. The sex, age, and education distributions, age of surgeon, surgical methods and anaesthesia, and types of IOL were different in the four volume strata among hospital volume and surgeon volume (all P<0.001). The surgical methods included phacoemusification (13.2%), ECCE (41.8%), and ICCE (5.7%). Majority of the patients (69.4%) received PMMA IOLs, and fewer patients received acrylic (5.7%), HSM PMMA (5.2%), and silicone IOLs (4.4%). Most (99.5%) of the patients received LA. In total, 88.1% of all patients received outpatient cataract surgery and 11.9% received in-patient cataract surgery. More patients (28.6%) received in-patients cataract surgery in high-volume hospitals than middle-high-volume (8.2%), middle-low-volume (4.3%), and low-volume hospitals (7.1%). However, those operated by high-volume surgeons had less in-patient surgery (2.2%). Among 1004 surgeons, 80.72% of surgeons working in low-volume hospitals belonged to the low-volume surgeon group. Middle-high-volume and middle-low-volume hospitals have more high-volume surgeons (Table 3). There were also significant differences in ophthalmic and medical comorbidities among the four hospital and surgeon volume strata (Table 4).
The overall incidence of postoperative endophthalmitis was 0.71% at 1 year and 0.84% at 2 years (Table 5). The 2-year incidence of postoperative endophthalmitis by hospital volume was 1.16% for low-volume hospitals, 0.67% for middle-low-volume hospitals, 0.61% for middle-high-volume hospitals, and 0.9% for high-volume hospitals (P<0.0001). The incidence of postoperative endophthalmitis by low-volume surgeons was 1.16, 0.80% for middle-low-volume surgeons, 0.73% for middle-high-volume, and 0.59% for high-volume surgeons. A statistically significant association was noted between provider volume and postoperative endophthalmitis.
After adjusting the potential risk factors by using stepwise Cox regression, we found that the risks of postoperative endophthalmitis of the low-volume hospitals (hazard ratio (HR)=1.39, P=0.0069) and low-volume surgeons (HR=1.67, P<0.0001) were statistically significantly higher than high-volume hospitals and high-volume surgeons, respectively (Table 5).
Discussion
Although previous studies showed that incidence of postoperative endophthalmitis was associated with case mix such as patients demographic characteristics,12, 13 ophthalmic comorbidities,14 medical comorbidities1, 12 including diabetes mellitus, immune deficiency, patients surgical factors such as surgical methods11, 13, 15 and different kinds of IOL implantation,16, 17 the hospital and surgeon volume associated with the incidence of postoperative endophthalmitis was seldom evaluated or even revealed without controlling other confounders.10
The lower risk of postoperative endophthalmitis in the high hospital volume group may be due to the bigger proportion of younger patients (≤50 years old, 5.7%) than the other hospital volume groups (≤50 years old, 2.7–3.7%) (Table 2). In total, 64.3% of younger patients (≤50 years old) and 20% of older patients (>50 years old) have the education more than junior high school. The younger patients' (≤50 years old) education is significantly more than the older patients (>50 years old) (P<0.0001). These young educated patients may be more compliant to the medication. They may tend to look for the high-volume hospital for operation and believe high-volume hospitals with better outcome. On the other hand, the proportion of senior surgeons (≥46 years old) in the high hospital volume group was bigger than the average of hospital volume groups (21.8 vs 18.2%). This phenomenon of bigger proportion of senior surgeons was also found in the high surgeon volume group (26.3 vs 18.2%) (Table 2). The lower risk of postoperative endophthalmitis in the high surgeon volume group may be due to the less proportion of patients (9.1%) who received operation by the doctors younger than 35 years old than in other surgeon volume groups (19.4–27.3%) (Table 2).
In the Cox regression, the HR of postoperative endophthalmitis of patients receiving cataract surgery by the low-volume hospitals (HR=1.39, P<0.0069) and surgeons (HR=1.67, P<0.0001) was still higher than the high-volume hospitals and surgeons, respectively (Table 5). The risk of endophthalmitis of patients being operated by a surgeon younger than 35 years old was also higher than (HR=1.29, P<0.0147) the senior surgeons group. Therefore, more senior surgeons in the high hospital volume group may represent greater experience, more familiarity with the surgery and less complication. The provider volume (hospital and surgeon volume) plays an important role in the risk of postoperative endophthalmitis.
The surgical method had been shown to associate with the incidence of postoperative endophthalmitis in the previous literatures.11, 13, 15 Before adjusting the parameters of surgical methods and the type of IOL, these parameters looked in the study may have influence on the incidence of endophthalmitis in Table 2. After adjusting the parameters by stepwise Cox regression, the hospital and surgeon volume did have influences on the risk of postoperative endophthalmitis (Table 5). Surgical methods including ICCE, ECCE, and PE were not significant in the Cox regression model (all P>0.05) in this study.
Although there was no previous study mentioning the association between surgeon volume and postoperative endophthalmitis, the significant negative association (Spearman's ρ=−0.63, P<0.01) between surgeon volume and intraoperative complications in Habib's study18 when they pooled 6 years and six doctors' data together could support our findings. However, concerning the association between intraoperative complications and surgeon volume of only one year, Habib's study showed no statistical significance. In our study, because we used the nationwide database with combined 1004 surgeons, statistically significant associations could be more apparent.
As far as ophthalmology is concerned, there have been only two studies that have looked into the possibility of a relation between variations in cataract clinical practice and outcome. Schein et al19 conducted a prospective cohort study of 772 patients undergoing first eye cataract extraction. Habib's study reviewed all cataract surgery performed from 1996 to 2001 by six consultant surgeons. Both Habib' study and Schein's study were from a single hospital, which reduces some of the variations in practice/environment that occur with multiple sites. Using one site does however raise the question regarding the national or international generalisation of the finding. This study was from administration data that can avoid this problem.
Administrative data have been used in recent years for a variety of purposes to study the differences in hospitalisation and surgical utilisation, to investigate the relationship between these differences and appropriateness of procedures, standards, and the quality of care for the selection of operations.20 In our study, claim data from universal coverage in Taiwan offer the opportunity to identify samples that are free from selection bias and are of sufficient size to document rare outcomes, and are helpful in assessing operation quality postdischarge. However, there are limitations in administrative data. First, the precision of the codes themselves and the accuracy with which they are recorded limit the nature of studies that may be undertaken successfully;21 the consistency rate between patient records and claim data is around 95% in a medical centre in Taiwan. Second, it is hard to differentiate from claim data whether a specific disease code was present prior to surgery or presented as a complication of treatment. Third, there may be the absence of some diagnoses because of the limitation of only five diagnoses in the NHI in-patient database. Fourth, the causal link between surgical volume and ophthalmology is not addressed in this study. Do higher volume surgeons and hospitals have better results because their experience has enabled them to improve their performance (the ‘practice makes perfect’ hypothesis)? Or, do patients and referring physicians know who the superior providers are and gravitate to them, thus increasing the volumes of the best providers (the ‘selective referral’ hypothesis)?22 Answering these questions will require follow-up on all surgeons' volumes and outcomes for more years. Fifth, the claimed database could not provide some parameters such as surgeon's experience, patient's compliance, preoperative and postoperative medication regime, etc. We can only use the variable of surgeon's age and patient's education as proxy variables in the Cox regression model in order to have a more comprehensive analysis.
In conclusion, high hospital and surgeon volume is associated with lower risk of postoperative endophthalmitis. Provider volume (hospital volume and surgeon volume) might play an important role in reducing the postoperative endophthalmitis.
References
American Academy of Ophthalmology. Basic and Clinical Science Course 2004/2005. Section 11: Lens and Cataract. American Academy of Ophthalmology: San Francisco, 2004/2005.
Javitt JC, Street DA, Tielsch JM, Wang Q, Kolb MM, Schien O et al. National outcomes of cataract extraction. Retinal detachment and endophthalmitis after outpatient cataract surgery. Cataract Patient Outcomes Research Team. Ophthalmology 1994; 101: 100–105.
Syam PP, Eleftheriadis H, Casswell AG, Brittain GP, McLeod BK, Liu CSC . Clinical outcome following cataract surgery in very elderly patients. Eye 2004; 18: 59–62.
Hannan EL, Racz M, Kavey RE, Quaegebeur JM, Williams R . Pediatric cardiac surgery: the effect of hospital and surgeon volume on in-hospital mortality. Pediatrics 1998; 01: 963–969.
Dardik A, Lin JW, Gordon TA, Williams GM, Perler BA . Results of elective abdominal aortic aneurysm repair in the 1990s: a population-based analysis of 2335 cases. J Vasc Surg 1999; 30: 985–995.
Hannan EL, Wu C, Ryan TJ, Bennett E, Culliford AT, Gold JP et al. Do hospital and surgeons with higher coronary artery bypass graft surgery volumes still have lower risk-adjusted mortality rate? Circulation 2003; 108: 795–801.
Smith ER, Butler WE, Barker FG . In-hospital mortality rates after ventriculoperitoneal shunt procedures in the United States, 1998–2000: relation to hospital and surgeon volume of care. J Neurosurg Spine 2004; 100: 90–97.
Losina E, Barrett J, Mahomed NN, Baron JA, Katz JN . Early failures of total hip replacement: effect of surgeon volume. Arthritis Rheum 2004; 50: 1338–1343.
Schrag D, Panageas KS, Riedel E, Hsieh L, Bach PB, Guillem JG et al. Surgeon volume compared to hospital volume as a predictor of outcome following primary colon cancer resection. J Surg Oncol 2003; 83: 68–78.
Morlet N, Li J, Semmens J, Ng J, team EPSWA . The Endophthalmitis Population Study of Western Australia (EPSWA): first report. Br J Ophthalmol 2003; 87: 574–576.
Javitt JC, Vitale S, Canner JK, Street DA, Krakauer H, McBean AM et al. National outcomes of cataract extraction: endophthalmitis following inpatient surgery. Arch Ophthalmol 1991; 109: 1085–1089.
Allardice GM, Wright EM, Peterson M, Miller JM . A statistical approach to an outbreak of endophthalmitis following cataract surgery at a hospital in the West of Scotland. J Hosp Infect 2001; 49: 23–29.
Norregaard JC, Thoning H, Bernth-Petersen P, Andersen TF, Javitt JC, Anderson GF . Risk of endophthalmitis after cataract extraction: results from the International Cataract Surgery Outcomes study. Br J Ophthalmol 1997; 81: 102–106.
Kanski JJ . Clinical Ophthalmology: A Systemic Approach, 4th edn. Butterworth-Heinemann Ltd: Stoneham, MA, 1999.
Cooper BA, Holekamp NM, Bohigian G, Thompson PA . Case control study of endophthalmitis after cataract surgery comparing scleral tunnel and clear corneal wounds. Am J Ophthalmol 2003; 136 (2): 300–305.
Menikoff JA, Speaker MG, Marmor M, Raskin EM . A case–control study of risk factors for postoperative endophthalmitis. Ophthalmology 1991; 98: 1761–1768.
Scott IU, Flynn Jr HW, Feuer W . Endophthalmitis after secondary intraocular lens implantation. A case-report study. Ophthalmology 1995; 102: 1925–1931.
Habib M, Mandal K, Bunce CV, Fraser SG . The relation of volume with outcome in phacoemulsification surgery. Br J Ophthalmol 2004; 88: 643–646.
Schein OD, Steinberg EP, Javitt JC, Cassard SD, Tielsch JM, Steinwachs DM et al. Variation in cataract surgery practice and clinical outcomes. Ophthalmology 1994; 101: 1142–1152.
Hannan EL, Kilburn H, Lindsey ML, Lewis R . Clinical versus administrative data bases for CABG surgery—does it matter? Med Care 1992; 30: 892–907.
Wei HM . Quality of claim management in healthcare organizations: a study on the consistency of ICD coding in a medical center. Institute of Hospital and Health Care Administration, National Yang-Ming University, Master's thesis, 2004.
Hannan EL, Kilburn Jr H, Bernard H, O'Donnell JF, Lukacik G, Shields EP . Coronary artery bypass surgery: the relationship between inhospital mortality rate and surgical volume after controlling for clinical risk factors. Med Care 1991; 29: 1094–1104.
Acknowledgements
The authors have no proprietary interest in any aspect of this study. This study was supported by a grant from the Bureau of National Health Insurance (DOH92-NH-1011).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Fang, YT., Chien, LN., Ng, YY. et al. Association of hospital and surgeon operation volume with the incidence of postoperative endophthalmitis: Taiwan experience. Eye 20, 900–907 (2006). https://doi.org/10.1038/sj.eye.6702045
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6702045
Keywords
This article is cited by
-
The effects of cement fixation on survival in elderly patients with hip hemiarthroplasty: a nationwide cohort study
BMC Musculoskeletal Disorders (2019)
-
Hospital and surgeon operation volume associated with endophthalmitis
Eye (2007)
-
Hospital cataract surgery volume and postoperative endophthalmitis
Eye (2007)
