
Abstract
Aim
A key aim of the photographic screening model for diabetic retinopathy advocated by the National Screening Committee is a reduction in new blindness due to diabetic retinopathy within 5 years. This study determines the incidence of visual impairment due to diabetic retinopathy in Leeds in 2002 and provides a benchmark against which the success of the retinopathy screening programme in Leeds will be judged.
Methods
A retrospective review of all blind and partially sighted registrations for 2002 was conducted. The 2001 Census data and the diabetes prevalence model developed by the Yorkshire and Humber Public Health Observatory were used to determine the total and diabetic populations of Leeds.
Results
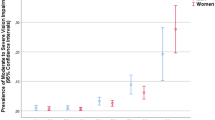
Diabetic retinopathy was the primary cause of registration in 24 of the 398 completed records obtained; seven patients were registered blind and 17 partially sighted. For the total population in 2002, the incidence of blind and partially sighted registration due to diabetic retinopathy was 10 per million and 24 per million per year, respectively. For the diabetic population of Leeds in 2002, the incidence of blind and partial sighted registration due to diabetic retinopathy was 337 and 817 per million per year, respectively.
Conclusions
The incidence of blind registration due to diabetic retinopathy in Leeds in 2002 is similar to the estimate provided by the National Screening Committee but higher than the figure from other UK centres.
Similar content being viewed by others


Introduction
Diabetic retinopathy complicates both type I and type II diabetes mellitus (DM). Although the cumulative risk of retinopathy is substantial in type I DM, reaching up to 60% for sight-threatening disease over 20 years, the overall burden of preventable blindness secondary to type II DM is greater, because its prevalence is higher.1, 2 The prevalence of DM, particularly type II DM, is rising throughout the world and especially in developed countries.3 In England and Wales, diabetic retinopathy remains the most common cause of blindness registration among people of working age.4, 5
Diabetic retinopathy fulfils the WHO criteria for screening in that it evolves through key recognizable stages in the progression to blindness, represents an important health problem, has valid and acceptable screening tests, and blindness can be prevented or visual decline slowed with laser photocoagulation.6, 7, 8, 9, 10
In the United Kingdom (UK), the National Screening Committee has recommended photographic screening for diabetic retinopathy as its preferred model.11 One of the key aims of the new systematic screening service is a reduction in the incidence of blindness due to diabetic retinopathy within 5 years.11 In this study, the incidence of visual disability due to diabetic retinopathy in Leeds is calculated for 2002. This figure will be used as a benchmark against which the success of the screening service in Leeds can be judged.
Methods
In this retrospective observational study, part 5 of all the completed BD8 registrations in Leeds for 2002 were collected and cross-checked against the central list of all new registrations held by Leeds Social Services. The age, degree of visual impairment (blind or partially sighted), and the main cause of visual impairment were noted for each completed form. Incomplete BD8 forms were excluded.
The 2001 Census data was used to provide the most accurate estimate of the population of the Leeds Metropolitan area for the study year. In the absence of a central register of diabetic patients, the number of people with diagnosed DM was estimated using the diabetes prevalence model developed by the Yorkshire and Humber Public Health Observatory.12 From the data available, the incidence of blind and partial sighted registrations due to diabetic retinopathy was calculated per million population and per million people with diagnosed diabetes.
Descriptive analysis were performed on the data collected using MS Excel 2000 (Microsoft Corporation, Seattle, USA).
Results
In 2002, Leeds Social Services received notification of 408 new BD8 registrations, of which 10 were incomplete and excluded from our analysis. Of the 398 new BD8 registrations analysed, there were 214 blind and 184 partially sighted registrations. (see Table 1)
Diabetic retinopathy was the primary cause of visual impairment in 24 cases; of whom seven were registered blind and 17 were registered partially sighted. Diabetic retinopathy accounted for 6% of all BD8 registrations and for 13% of registrations in the age group 16–64 years (Tables 1 and 2).
In 2001, the population of the Leeds Metropolitan area was 715 414. The breakdown by sex, ethnic group, and age is given in Table 3, together with the same breakdown for the England and Wales population. Based on the age, sex, and ethnicity distribution of the Leeds population, the Yorkshire and Humber Public Health Observatory Model estimated the prevalence of diagnosed diabetes within the total population to be 0.34% for type I and 2.57% for type II DM. The estimated number of people with diagnosed DM in 2002 was 20 800, of whom 2410 had type I and 18 390 had type II DM.
For the total population, the incidence of blind and partially sighted registration due to diabetic retinopathy in 2002 was 10 per million and 24 per million per year, respectively. For the diabetic population in Leeds, the incidence of blind and partial sighted registration due to diabetic retinopathy in 2002 was 337 and 817 per million per year, respectively (see Table 2).
Discussion
There are two accepted models of screening for diabetic retinopathy: a photographic model and an optometrist based model.11, 13 The National Screening Committee, convened by the British Diabetic Association, recommended a systematic national screening programme, based on the photographic model, in order to reduce present inequalities in service provision and produce a model for the establishment of a cost-effective national programme.11 One of the key aims of the strategy proposed by the National Screening Committee is a reduction in diabetic retinopathy related blindness by a ‘minimum’ target of 10% and an ‘achievable’ target of 40% within 5 years.11, 14
The success of a screening initiative can only be judged by documenting a fall in the relevant complication over a number of years and within a defined region. In Leeds as in many other UK units, there were no local figures for the incidence of visual disability due to diabetic retinopathy. While moving towards the full implementation of a systematic photographic screening programme, this study has established a base-line figure against which the success of this initiative can be judged.
In our study the BD8 registrations have been used to ascertain the incidence of visual disability in Leeds. To register a patient as either blind or partially sighted, the consultant Ophthalmologist must complete a BD8 form. Guidelines for registrations are shown in Table 4. The use of a blind register to study visual disability rates is imperfect. Blind registers are noted to underestimate significantly the visual impairment; particularly for chronic disease.15 Several factors may influence the probability of registration, such as patient access to GPs, opticians and social workers, and their subsequent referral to an ophthalmologist. Patients' perceptions of their own condition may also affect the likelihood of registration. A patient who perceives a need for registration and conveys this to an ophthalmologist is more likely to be registered than a patient who accepts failing eyesight. In the UK registration is voluntary for the patient and the proportion of patients who refuse registration is not known. Capture-mark recapture has been used to estimate the true incidence of visual disability.16 Although this system might help to reveal the degree of under-registrations, there is not enough in the ophthalmic literature to validate its use.
The incidence of blindness due to diabetic retinopathy in this study is similar to the estimate of 9.5 per million population per year for 1990–1991, used by the National Screening Committee.11 Furthermore, the relative contribution of diabetic retinopathy to visual impairment is similar to the national data for 1990–1991.4, 5 However, we do not believe that this figure can be assumed to be correct for all regions in the United Kingdom. Potential reasons for regional variation include the prevalence of diabetes and hence the expected incidence of diabetic retinopathy related blindness. This in turn is dependent on demographic factors such as age and ethnic distribution in the community.17, 18, 19, 20 It is well documented that the ethnic distribution is especially important as the prevalence of DM in middle-aged Asians is five times that of a European population.21 The ethnic distribution in Leeds is very similar to England and Wales; however, within the UK there is a large inter-regional variation.
The incidence of diabetic retinopathy related visual disability may also be affected by the presence of ongoing screening initiatives at varying stages of implementation in the different regions. During 2002, there were three diabetic retinopathy screening cameras in operation in Leeds. These were installed in the two teaching hospitals and in a community eye centre. This screening programme did not cover the entire diabetic population of Leeds, and the retinopathy screening programme for diabetics managed exclusively in the community was unstructured.22
Data from different regions regarding the incidence of diabetic retinopathy related blindness are scarce in the literature.23, 24, 25, 26, 27, 28, 29 The few studies that are available do not allow direct comparisons between regions as differing measurement parameters have been used. The National Screening Committee has estimated the incidence of diabetic retinopathy blindness per million per year and the same measure is used in this study.
Comparison with other studies is further complicated because of the different definitions of blindness in use; the WHO has accepted some 65 definitions of blindness.30 We used the definition recommended by the BD8 form. Since both the BD8 and BP1 forms have very similar guidelines for registration, the use of this definition should allow for direct comparison between centres in England, Wales, and Scotland. Comparison will also be possible with the Certificate of Visual Impairment introduced in 2003.31, 32
The incidence of blindness due to diabetic retinopathy in the total and diabetic populations in this study is similar to that calculated for Newcastle from 1998–2000, namely 8.7 per million total population per year and 350 per million diabetics per year.29 However, the incidence of either visual impairment or blindness due to diabetic retinopathy in the diabetic population of this study is far higher than the corresponding figure for visual impairment of 530 per million diabetics per year calculated for Tayside in 1998 or for blindness of 64 per million diabetics per year calculated for Fife between 1990–1999.26, 27 Although Arun claimed that the Newcastle figure was testimony to the success of the local screening programme, the figure for the Tayside region was derived for a diabetic population, which was also enrolled into a photographic screening programme.29 We believe that this variation more likely reflects differing local populations and illustrates the need for each individual area to calculate its own incidence data. Data from nearby Bradford supports this view. In Bradford, the South Asian community had an incidence of diabetic retinopathy related blindness almost four times that of the Caucasian community.19 To date, there is little good evidence to suggest that a formal screening programme does reduce the incidence of visual impairment due to diabetic retinopathy. Failed laser treatment and poor patient attendance accounted for much of the visual impairment in diabetics who had been screened, suggesting that the screening exercise itself may have little impact on future visual impairment.33
As with many UK centres, there was no diabetes register in Leeds during the study period. We therefore used the population prevalence model published by the Yorkshire and Humber Public Health Observatory to estimate the prevalence of diagnosed diabetes in Leeds. This model uses 2001 Census data and applies age, sex, and ethnicity specific estimates of prevalence. It assumes that one-third of prevalent cases of type II diabetes are undiagnosed, although this proportion would be expected to be lower in areas where there are proactive diabetes screening initiatives. The potential error associated with this mathematical model is unclear. The incidence figures in this paper relate to the predicted number of people with diagnosed diabetes only.
We plan to repeat this study at intervals in order to assess the success of photographic screening for diabetic retinopathy in Leeds. The full implementation of the photographic screening service is expected by the end of 2004. The current data provide us with a baseline figure and also suggest that the incidence varies between regions. We recommend that all regions should determine their baseline figures independently.
References
Davies R, Rodence P, Brailsford S . The evaluation of screening policies for diabetic retinopathy using simulation. Diabetic Med 2002; 19: 762–770.
Klein R, Klein BEK, Moss SE . Visual impairment in diabetes. Ophthalmology 1984; 91: 1–9.
James M, Turner DA, Broadbent DM, Harding SP . Cost effectiveness analysis of screening for sight threatening diabetic eye disease. BMJ 2000; 320: 1627–1631.
Evans JR . Causes of blindness and partial sight in England and Wales 1990–91, Studies on Medical and Population Subjects Reports No. 57 HMSO: London, 1995.
Evans JR, Rooney C, Ashwood F, Dattani N, Wormald R . Blindness and partial sight in England and Wales: April 1990–March 1991. Health Trends 1996; 28: 5–12.
Wilson JMG, Junner O . The principles and practice of screening for disease. Public Health Papers 34 WEW: Geneva, 1968.
Diabetic Retinopathy Screening Group. Photocoagulation treatment of proliferative diabetic retinopathy. Clinical application of diabetic retinopathy (DRS) findings. DRS Report No. 8. Ophthalmology 1981; 88: 583–600.
Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes and progression of long term complication in insulin dependent diabetes mellitus. N Engl J Med 1993; 329: 977–986.
Early Treatment Diabetic Retinopathy Study Research Group. Early photocoagulation for diabetic retinopathy. ETDRS Report No. 9. Ophthalmology 1991; 98: 766–785.
Early Treatment Diabetic Retinopathy Study Research Group. Treatment techniques and clinical guidelines for photocoagulation of diabetic macular oedema ETDRS Report No. 2. Ophthalmology 1987; 94: 761–764.
Working Party. Guidelines for Diabetic Retinopathy. Royal College of Ophthalmologists: London, 1997, p 5.
World Health Organisation in Europe and European Region of International Diabetes Federation. The St Vincent Declaration 1989. Diabet Med 1990; 7: 360.
Robinson R, Deutsch J, Jones HS, Youngson-Reilly S, Hamlin DM, Dhurjon L et al. Unrecognised and unregistered visual impairment. Br J Ophthalmol 1994; 78: 736–740.
McCarty DJ, Tull ES, Moy CS, Kwoh CK, LaPorte RE . Ascertainment corrected rates: applications of capture-recapture methods. Int J Epidemiol 1993; 22: 559–565.
Hayward LM, Burden ML, Burden AC, Chang YF . What is the prevalence of visual impairment in the general and diabetic populations: are there ethnic and gender differences? Diabetic Med 2002; 19: 27–34.
Rauf A, Ong PS, Wormald RPL . The pilot study into the prevalence of ophthalmic disease in the Indian population of Southall. J Roy Soc Med 1994; 84: 78–79.
Pardhan S, Mahomed I . The clinical characteristics of Asian and Caucasian patients on Bradford's Low Vision Register. Eye 2002; 16: 572–576.
Prasad S, Kamath G, Jones K, Clearkin LG, Phillips RP . Prevalence of blindness and visual impairment in a population of people with diabetes. Eye 2001; 15: 640–643.
Mather H, Keen H . The Southall Diabetes Survey: prevalence of known diabetes in Asians and Europeans. BMJ 1985; 291: 1081–1084.
McKibbin M, Walters G, O'Neil D . Current diabetic retinopathy screening by general practitioner practices in Leeds, Poster at the Royal College of Ophthalmologists Annual Congress, Cardiff, 1999.
Ghafour IM, Allan D, Foulds WS . Common causes of blindness and visual handicap in the west of Scotland. Br J Ophthalmol 1988; 67: 209–213.
Aclimandos WA, Galloway NR . Blindness in the city of Nottingham (1980–85). Eye 1988; 2: 431–434.
Munier A, Gunning T, Kenny D, O'Keefe M . Causes of blindness in the adult population of the Republic of Ireland. Br J Ophthalmol 1998; 82: 630–633.
Bamashmus MA, Mathiga B, Dutton GN . Causes of blindness and visual impairment in West of Scotland. Eye 2004; 18: 257–261.
Cormack TGM, Grant B, Macdonald MJ, Campbell IW . Incidence of blindness due to diabetic eye disease in Fife 1990–9. Br J Ophthalmol 2001; 85: 354–356.
Thompson JR, Du l, Rosenthal AR . Recent trends in the registration of blindness and partial sight in Leicestershire. Br J Ophthalmol 1989; 73: 95–99.
Arun CS, Ngugi N, Taylor R . Effectiveness of screening in preventing blindness due to diabetic retinopathy. Diabetic Med 2003; 20: 186–190.
World Health Organisation. International classification of impairments, disabilities and handicaps. WHO: Geneva, 1980, pp 79–85.
Form BP1 (2R). Edinburgh: The Scottish Office Home and Health Department, St Andrew's House.
Record of examination to certify a person as blind or partially sighted (BD8 1990). Guidance Notes. The Stationery Office: London.
Rhatigan MC, Leese GP, Ellis J, Ellingford A, Morris AD, Newton RW et al. Blindness in patients with diabetes who have been screened for eye disease. Eye 1999; 13: 166–169.
Acknowledgements
We thank the staff of Leeds Social Services and Mr Keith Jackson for their cooperation and secretarial support in conducting this study. Miss Sharmila Jivan was instrumental in data collection and assimilation.
Author information
Authors and Affiliations
Corresponding author
Additional information
The authors have no proprietary or financial interest in any of the products
Rights and permissions
About this article
Cite this article
Kumar, N., Goyder, E. & McKibbin, M. The incidence of visual impairment due to diabetic retinopathy in Leeds. Eye 20, 455–459 (2006). https://doi.org/10.1038/sj.eye.6701908
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6701908
