
Abstract
Purpose To study the distribution of anaesthetic fluid during sub-Tenon's block by B-scan ultrasonography using cannulae of three different lengths.
Methods A total of 30 patients undergoing routine phacoemulsification and lens implantation were studied after informed consent had been obtained. Ages ranged from 60 to 92 years and globe axial lengths from 21.50 to 27.00 mm. All were given a sub-Tenon's block and the patients were classified into three groups in which either a long, intermediate, or short cannula was used. B-scan ultrasonography was performed before administration of the anaesthetic agent, during injection, and 2 min after completion of the injection.
Results In all patients the optic nerve was identified. During the injection, anaesthetic fluid could be seen tracking behind the globe and opening up the posterior sub-Tenon's space (the previously described ‘T’-sign). After 2 min very little or no fluid was seen, suggesting that it had dispersed into the surrounding tissues. There was no discernible difference in the distribution of fluid or in the quality of the block in the three groups.
Conclusions B-scan ultrasonography can reliably identify the distribution of anaesthetic fluid during sub-Tenon's block. Anaesthetic agents can be successfully delivered into the sub-Tenon's space by long, intermediate, or short cannulae.
Similar content being viewed by others


Introduction
Local anaesthetic agents can be administered into sub-Tenon's space via long1 (Stevens: Visitec: metal 19 G, 2. 54 cm), intermediate2 (Kumar–Dodds: Simco, plastic 22 G, 1.8 cm), or short3 (Greenbaum: Alcon, plastic 14 G, 1.2 cm) sub-Tenon's cannulae. The long metal cannula is popular with practitioners, but there are recent reports of serious complications, such as globe perforation,4 orbital haemorrhage,5 and damage to extraocular muscles.6,7 Two recent studies8,9 have shown that satisfactory globe anaesthesia and akinesia can be achieved with a sub-Tenon's injection via a shorter cannula. It is undetermined whether posterior spread of the anaesthetic agent plays an important role in producing sensory and motor blockade. Fluid in the posterior part of sub-Tenon's space gives a characteristic ‘T’-sign on B-scan ultrasonography. This sign has been observed with the injection of anaesthetic solution via the 2.54 cm metal cannula.10,11 We are not aware of any study that has either reported or compared the ultrasonic localization of the anaesthetic fluid with shorter sub-Tenon's cannulae. We were particularly interested to determine whether shorter cannulae can deliver anaesthetic fluid into the posterior sub-Tenon's space with the same efficiency as the longer cannulae.
This study was designed to compare the distribution of anaesthetic fluid during sub-Tenon's block by B-scan ultrasonography using sub-Tenon's cannulae of three different lengths.
Methods
A total of 30 patients ranging in age from 60 to 92 years, with globe axial lengths of 21.50–27.00 mm, undergoing routine phacoemulsification and lens implantation were studied. All patients gave informed consent for ultrasonography and participation in the study. The anaesthetic techniques and assessment of ocular motility were part of the practitioner's (CMK) routine clinical practice. Following instillation of benoxinate 0.4% drops, one anaesthetist (CMK) made a small conjunctival incision with Westcott scissors in the inferonasal quadrant about 5 mm posterior to the limbus. At the beginning of each list a sealed envelope was opened, which contained a random choice of the cannula to be used during that session. Three cannulae were used: the 2.54 cm metal (Stevens—Figure 1), 1.8 cm plastic (Kumar–Dodds—Figure 2), and 1.2 cm plastic (Greenbaum—Figure 3). The study continued until 10 of each cannula had been used. The cannula was inserted through the incision onto the bare sclera and into the sub-Tenon's space. B-scan ultrasonography (Alcon Ultrascan® Imaging System) was performed on the eye before the injection by one surgeon (BJM) and optic nerve was identified. A measure of 5 ml of 2% lidocaine containing 150 units of hyaluronidase was injected. Another scan was performed during the injection and repeated 2 min later. Elevation, depression, adduction, and abduction of the globe were separately assessed on a scale of 0–3, where 0=no movement, 1=minor movement, 2=moderate movement, and 3=normal movement. Motility was assessed at 2 min interval until 6 min after injection. An aggregate akinesia score of less than 4 was deemed satisfactory for surgery. If the aggregate akinesia score was more than 4 at 6 min, a supplementary injection was administered. Patients estimated pain during injection on the Verbal Analogue Score. On the scale of 0–10, 0 represents no pain and 10 represents the worst imaginable pain. The severity and quadrant(s) of chemosis and conjunctival haemorrhage were also recorded if they occurred.

Long metal cannula 19 G, 2.5 cm.

Intermediate plastic cannula 22 G, 1.8 cm.

Short plastic cannula 14 G, 1.2 cm.
Results
The optic nerve was seen clearly on the scan in all cases before injection (Figure 4a–c). During injection, anaesthetic fluid was seen expanding the sub-Tenon's space behind the globe (a crescentic echo-free void) in all patients (Figure 5a–c). The fluid surrounded the optic nerve and gave a characteristic ‘T’-sign in all but one case, in which a Greenbaum cannula had been used. The cannulae themselves were not seen on the scan. At 2 min after injection, either the void had disappeared or very little fluid remained (Figure 6a–c). Each sequence of images (Figures 4a, 5a, 6a, etc) is from one patient in each cannula group. A total of 29 patients (97%) had an aggregate motility score of less than 4 within 4 min of injection, but one patient in Greenbaum group, where excessive loss of local anaesthetic occurred during injection, required supplementary injection. A total of 11 patients (36%) complained of slight pain on injection (Verbal Analogue Score <3). The remainder did not report any discomfort. The incidence of pain did not vary with the type of cannula used. Mild chemosis and conjunctival haemorrhage occurred in 18 patients (60%) in the inferonasal quadrant at the site of dissection. In some cases it spread to other quadrants.

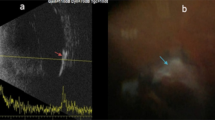
Preinjection ultrasound B-scan—arrows showing outline of optic nerve: (a) long cannula group, (b) intermediate cannula group, and (c) short cannula group.

During injection—arrows showing expanded posterior sub-Tenon's space and ‘T’-sign: (a) long cannula group, (b) intermediate cannula group, and (c) short cannula group.

At 2 min postinjection—arrows showing closure or diminution of posterior sub-Tenon's space: (a) long cannula group, (b) intermediate cannula group, and (c) short cannula group.
Discussion
Anaesthetic fluid appeared in the posterior sub-Tenon's space in all cases giving similar ultrasound pictures, including, with one exception, the typical ‘T’-sign. Satisfactory anaesthesia and akinesia were achieved in all patients.
In this study, access to sub-Tenon's space was inferonasal and 5 ml of fluid was injected in all cases to minimize variation caused by volume effects. The techniques were part of the routine practice of one experienced anaesthetist, who had regularly used all three cannulae. The volume of local anaesthetic chosen may appear excessive, but most published studies advocate this volume1,9,12,13 to achieve anaesthesia, adequate reduction of ocular movements, and to reduce the need for supplementary injections. The incidence of pain on injection,1,12,14,15 chemosis,1,9,12,14 and conjunctival haemorrhage1,9,12,14 are similar to those in other published studies. Chemosis was noted with all three cannulae, suggesting that fluid often tends to spread anteriorly, irrespective of the length of the cannula.
The study demonstrates that B-scan ultrasonography is a simple, noninvasive method of identifying the distribution of anaesthetic fluid during sub-Tenon's block. The characteristic ‘T’-sign seen during injection suggests that anaesthetic agents can be delivered into the posterior part of sub-Tenon's space with equal efficiency via a short, intermediate, or long cannula. The achievement of anaesthesia and satisfactory akinesia within 2–4 min of injection coincides with disappearance of fluid behind the eye and lends support to the hypothesis that sub-Tenon's techniques produce sensory and motor blockade in the orbit by posterior diffusion of anaesthetic agent into the muscle cone. It could also be postulated that eye movement is reduced by spread of fluid along the muscle sheaths, but we did not observe expansion of the sheaths on ultrasonography or any other signs to support this mechanism.
Direct mechanical trauma from longer cannulae is a plausible explanation for the reports of muscle damage, orbital haemorrhage, and globe perforation. We consider that our study lends additional support for the deployment of short cannula techniques and advocate further work to examine their safety and effectiveness in clinical practice.
References
Stevens JD . A new local anaesthesia technique for cataract extraction by one quadrant sub-Tenon's infiltration. Br J Ophthalmol 1992; 76: 670–674.
Kumar CM, Dodds C . A disposable plastic sub-Tenon cannula. Anaesthesia 2001; 56: 399–400.
Greenbaum S . Parabulbar anaesthesia. Am J Ophthalmol 1992; 114: 776.
Frieman BJ, Friedberg MA . Globe perforation associated with sub-tenon's anesthesia. Am J Ophthalmol 2001; 131: 520–521.
Olitsky SE, Juneja RG . Orbital haemorrhage after the administration of sub-Tenon's infusion anaesthesia. Ophthalmic Surg Lasers 1997; 28: 145–146.
Spierer A, Schwalb E . Superior oblique muscle paresis after sub-Tenon's anesthesia for cataract surgery. J Cataract Refract Surg 1999; 25: 144–145.
Jaycock PD, Mather CM, Ferris JD, Kirkpatrick JNP . Rectus muscle trauma complicating sub-Tenon's local anaesthesia. Eye 2001; 15: 583–586.
Ntim-Amponsah CT . Evaluation of Greenbaum's anaesthetic technique using lignocaine with adrenaline. West African J Med 1998; 17: 144–147.
Kumar CM, Dodds C . An anaesthetic evaluation of Greenbaum sub-Tenon block. British J Anaesth 2001; 87: 631–633.
Stevens JD, Restori M . Ultrasound imaging of no needle 1-quadrant sub-Tenon local anaesthesia for cataract surgery. Eur J Implant Refract Surg 1993; 5: 35–38.
Winder S, Atta HR . Ultrasonic localization of anaesthetic fluid in sub-Tenon's, peribulbar, and retrobulbar techniques. J Cataract Refract Surg 1999; 25: 56–59.
Roman SJ, Chong Sit DA, Boureau CM, Auclin FX, Ullern MM . Sub-Tenon's anaesthesia: an efficient and safe technique. Br J Ophthalmol 1997; 81: 673–676.
Tokuda Y, Oshika T, Amano S, Yoshitomi F, Inouye J . Anaesthetic dose and analgesic effects of sub-Tenon's anaesthesia. J Cataract Refract Surg 1999; 25: 1250–1253.
Verghese I, Sivraj P, Lai YK . The effectiveness of sub-Tenon's infiltration of local anaesthesia for cataract surgery. Aust N Z J Ophthalmol 1996; 24: 117–120.
Zafirakis P, Voudouri A, Rowe S, Livir-Rallatos G, Livir-Rallatos C, Canakis C et al. Topical versus sub-Tenon's anaesthesia without sedation in cataract surgery. J Cataract Refract Surgery 2001; 27: 873–879.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was presented at the annual meeting of the Ophthalmic Anesthesia Society in Chicago, IL, USA on 7th October 2001
The authors have no financial interest in the cannula or any other product mentioned
Rights and permissions
About this article
Cite this article
Kumar, C., McNeela, B. Ultrasonic localization of anaesthetic fluid using sub-Tenon's cannulae of three different lengths. Eye 17, 1003–1007 (2003). https://doi.org/10.1038/sj.eye.6700501
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6700501
Keywords
This article is cited by
-
Sub-Tenon’s anaesthesia for modern eye surgery—clinicians’ perspective, 30 years after re-introduction
Eye (2021)
-
Incidence and impact factors of intraoperative loss of light perception under sub-Tenon’s anesthesia in patients with macular diseases
Eye (2019)
-
Real-time visualisation of anaesthetic fluid localisation following incisionless sub-Tenon block
Eye (2014)
-
The effect of hyaluronidase on ultrasound-measured dispersal of local anaesthetic following sub-Tenon injection
Eye (2008)
