
Abstract
This paper describes three cases of vasoproliferative tumours of the retina including histopathology in one. The clinical presentation, differential diagnosis and treatment modalities are discussed with a brief review of the literature.
Similar content being viewed by others


Introduction
Vasoproliferative tumours of the retina (VPTR) are benign lesions that are typically found in healthy patients. The lesions are characteristically reddish-yellow or peach-coloured solid masses found in the retinal periphery. There are often associated exudative and haemorrhagic changes within and under the retina. The term ‘presumed acquired retinal haemangioma’ was described by Shields et al1 as a separate entity as compared to capillary haemangioma of hereditary origin. Shields later coined the more descriptive term ‘vasoproliferative retinal tumour’, as his group believed that many of these vascular lesions may not truly represent haemangiomas. Shields et al2 classify these vasoproliferative tumours as either idiopathic or secondary, caused by congenital, inflammatory, vascular, traumatic, dystrophic, and degenerative ocular diseases. We describe two cases referred to us as suspected melanoma and one referred as suspected retinal tear whom we diagnosed as vasoproliferative tumours of retina (one case with histopathology) and reviewed in our retina clinic.
Case reports
Case 1 A 64-year-old healthy white woman was referred for melanoma. She was complaining of poor central vision in her right eye following uneventful cataract surgery with intraocular lens implant 6 weeks ago. She had a history of prophylactic laser treatment for a symptomatic operculated retinal hole in the superotemporal periphery of her left eye 5 years earlier. On examination, her best-corrected visual acuity was 20/400 (3/60) in the right eye and 20/40 (6/12) in the left eye. Intraocular pressures were 24 mmHg in the right eye and 16 mmHg in the left eye. She had a 1+relative afferent papillary defect in the right eye. Anterior segment examination revealed a well-positioned posterior chamber lens in the right eye and a mild cortical cataract in the left eye. Binocular indirect ophthalmoscopy revealed a treated retinal hole in the superotemporal periphery of the left fundus. The right eye had a shallow, subtotal exudative retinal detachment with widespread retinal pigment epithelial disruption and subretinal lipid accumulation. In the vitreous base region of the right eye at 1 o'clock, there was an orange, elevated mass that appeared to be arising from sensory retina with surface microvascular, telangiectatic and glial changes (Figure 1a and b). There were numerous cells seen in the vitreous. Ultrasound B-scan showed a high initial and high internal reflectivity, which was quite uniform. A CT scan of the brain and para nasal sinuses was normal and the fundus lesion showed enhancement with contrast. A provisional diagnosis of vasoproliferative tumour of the retina was made and the patient was followed for signs of progression. Three months later, she developed neovascularization of the iris and angle and was scheduled for radioactive plaque therapy. Meanwhile she developed a vitreous haemorrhage that cleared after 4 months, and at this stage she had painful blind eye secondary to progressive neovascular glaucoma. Her right eye was enucleated to alleviate unrelenting pain.

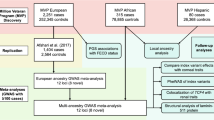
(a) In the superonasal periphery of the right eye, a pink solid mass (VPTR) with surface vascularization and glial changes is seen with adjacent haemorrhagic and exudative retinal changes. (b) In the inferior periphery of the same eye, there is evidence of exudative retinal detachment with telangiectatic vascular changes within the retina. (c) Low power magnification of the retinal tumour shows predominantly elongated cells arranged without any specific pattern and numerous blood vessels. Between the elongated cells, eosinophilic depositions are seen (haematoxylin and eosin stain, × 10 objective). (d) The depositions between elongated cells are stained in red for fibrin (Martius yellow-scarlet-blue (MSB), × 10 objective). (e) Only the endothelial cells of the blood vessels are immunoreactive for CD34 (× 10 objective). (f) The elongated cells are immunoreactive for glial fibrillary acidic protein (GFAP) demonstrating glial origin (× 25 objective).
Results of histopathology
Gross examination of the right enucleated eye showed a retinal mass located in the superior nasal quadrant measuring 7 × 6.5 × 4 mm3. and a massive retinal detachment with subretinal fluid. As seen in Figure 1(c–f), light microscopic examination of the retinal mass showed predominantly proliferation of elongated cells in addition to blood vessels. Eosinophilic cytoplasm and a small nucleus characterized the elongated cells. There was no evidence of cellular atypia or mitotic figures. Within the nodule, numerous blood vessels, some of which show thickened and hyalinized walls, were apparent. Between elongated cells, rare intact red blood cells were noted. Staining with Martius yellow-scarlet-blue (MSB) showed fibrin deposition between elongated cells and within the wall and lumen of some of the blood vessels. Perls' Prussian blue stain showed iron depositions within the nodule. Elongated cells were immunoreactive for glial fibrillary acidic protein, vimentin and S-100, consistent with glial cell origin. No immunoreactivity was seen for CD34, smooth muscle actin, desmin, myoglobin, and neurofilament. The melanocyte marker, HMB45, and epithelial marker, AE1/AE3, were also negative. Smooth muscle actin and CD34 outlined the blood vessels. Adjacent to the mass and within the subretinal exudate, foreign body giant cells, macrophages, and cholesterol clefts were noted. Focal retinal pigment epithelium hyperplasia and focal choroidal atrophy underlay the retinal mass. Vitreous neovascularization and haemorrhage were noted in addition to iris and epiretinal neovascularization. The central retinal vein and artery remained patent.
Case 2 A 67-year-old healthy Indian male was initially refered for melanoma. He had symptoms of floaters at that time. He had myocardial infarction 12 years prior to this and remained healthy and active without any sequelae. He gave a history of blunt trauma to the right eye in childhood, which resulted in some haemorrhage, but no further details were available regarding this, as he was in India at that time. He had 9 dioptre of myopia in the right eye and 5 dioptre of myopia in the left eye. His best-corrected visual acuity was 20/40 (6/12) in the right eye and 20/20 (6/6) in the left eye. The anterior segment was normal on slit-lamp biomicroscopy as well as the left fundus. However, the right fundus showed, between ora and equator, an orange-grey oval-shaped lesion, and examination with fundus contact lens showed multiple areas of neovascularization on its surface and some haemorrhage on its inferior part (Figure 2a) and a faint vitreous haemorrhage. There was no tortuosity or dilatation of vessels in its surroundings. The lesion measured, on ultrasound B-scan 5 × 4 mm in base diameter and 1.2 mm in height. There was no acoustic hollowness or choroidal excavation. This patient was followed up to now for nearly 5 years without any further symptoms. The base diameters remain the same, but the height was noticed to be 1.9 mm on his recent examination with increase in surrounding exudates and haemorrhages with increase in pigmentary changes (Figure 2b) but without any ocular symptoms (VPTR). The vision on his recent examination was 20/80 (6/24) because of nuclear lens changes. His disc and macula remained healthy.

(a) Oval-shaped lesion (this appeared greyish-pink in color) with surface neovascularization and surrounding haemorrhage in its inferior part. (b) The same lesion in (a) after 5 years appears slightly larger in size with surrounding exudates and haemorrhagic changes and increased pigmentary changes in its superotemporal part.
Case 3 A-30-year old white healthy male was referred for floaters in the right eye of 1-month duration subsequent to blunt trauma with hockey puck to the right eye, and was treated for suspected retinal tear with laser elsewhere and later referred to the retina services. On examination, visual acuity was 20/20 (6/6) in each eye. Slit-lamp biomicroscopy and fundus ophthalmoscopy was normal in the left eye. Right eye fundus showed a round, greenish-yellow, exudative, raised lesion (VPTR) in the inferotemporal periphery and a scanty overlying vitreous haemorrhage (Figure 3). Ultrasound B-Scan showed a solid lesion, irregular in shape with high internal reflectivity. This lesion was treated with cryotherapy. Two weeks post-operative period the visual acuity was 20/60 (6/18). An epiretinal membrane was noted in the macular area at this stage. The lesion showed some regression over a 3-month period and the epiretinal membrane became insignificant, improving the vision to 20/30 (6/9). This patient was followed up for 6 months; his vision remains stable without any further complication.

A globular raised lesion (this appeared grey-green in colour) is noted in the inferotemporal periphery of the right eye with a scanty overlying vitreous haemorrhage. There is prominent subretinal lipid posterior to the lesion. Focal retinal pigment epithelial changes are related to previous demarcating laser treatment.
Comments
VPTR are benign lesions of unknown origin. Histologically they represent reactive gliovascular proliferation.2,3,4 Shields et al2 suggested that these lesions develop secondary to a variety of underlying disease processes that prompt pigment epithelium and vascular proliferation. These tumours could represent an unusual manifestation of ocular neovascularization that assumes tumorous proportions, or these tumours could be an expression of vascularization of pigment epithelial proliferation or reactive gliosis.5,6,7
The differential diagnosis of VPTR includes other vascular or tumorous lesions of the ocular fundus, such as retinal capillary haemangiomas (with or without systemic angiomas, ie von Hippel Lindau disease), Coat's disease, peripheral exudative haemorrhagic chorioretinopathy (PEHC), choroidal melanomas, and retinal/choroidal metastasis. These vasoproliferative tumours differ from the typical von Hippel retinal capillary haemangioma in that they have predilection for the inferotemporal periphery. In VPTR lesions, there is a notable absence of the dilated and tortuous feeder and draining vessels, which are apparent in von Hippel retinal capillary angiomas even when the tumour is tiny (500 μm).2 VPTR lesions are usually seen at an older age of onset and with a negative family history. In VPTR, there is a lack of associated systemic tumours on CT scans. The VPTR lesions are usually unilateral and solitary.
In our cases, the diagnosis of VPTR was based on clinical findings, ultrasonography, and past ocular and family history. None of our patients had any positive family history for von Hippel Lindau or any other systemic hamartomas. In case 1, the location of the tumour was in the superonasal quadrant, which is not so common. The presence of rubeosis and progressive neovascular glaucoma leading to painful blind eye as seen in our case is not seen frequently in the previously reported case series in the literature. Shield et al2 described rubeosis in three cases out of 113 eyes with vasoproliferative tumours. One was idiopathic and the other two were secondary as classified in their series. The idiopathic tumour was inferotemporal in location and measured 7 × 7 × 4 mm3 in size, and the secondary VPTR were diffuse (<10 mm) and had neovascular glaucoma. Heiman et al3 described one patient out of 22 eyes with VPTR who had enucleation for painful blind eye because of neovascular glaucoma. The various triggering factors involved in the angiogenesis and glial proliferation remain a matter of further research in the aetiology of VPTR. It is not known how long the patient had this lesion as the cataract might have been masking her symptoms, but the rubeosis was seen 4 months after uneventful cataract surgery. We presume that this surgical event might have triggered the angiogenic factors to have its effect on the iris and angle structure. In case 1, the predominant glial cell proliferation is similar to previously reported cases of vasoproliferative tumours with glial predominance.3,8 The presence of fibrin deposition, the present and past episodes of haemorrhage within the retinal lesion, and massive exudative retinal detachment may all be contributing factors in the reactive process leading to massive glial cell proliferation. In case 2, the patient remained asymptomatic hitherto, although there are exudative changes in its surroundings with healthy macula and some visual axis lens changes. The presence of retinal pigment epithelial hyper pigmentation in its superior aspect (Figure 2b) is also suggestive of some on-going reactive process. In case 3, the association of vitreous haemorrhage and blunt trauma warranted retinal tear exclusion, and the poor peripheral view in the presence of mild vitreous haemorrhage can lead one to suspect retinal tear. However, the ultrasound A- and B- scan are helpful at this stage to rule out PVD and retinal detachment. It is difficult to say how long this tumour was present without any previous detailed retinal examination record. This patient remained asymptomatic until the episode of blunt trauma, which was the precipitating factor for onset of his symptoms. This suggests that this vasoproliferative tumour existed in the dormant form in this young healthy patient.
These cases, showing a wide clinical variation in their natural course, suggest that vasoproliferative tumours require periodic follow-up in spite of remaining asymptomatic and perhaps a careful explanation of associated complications that may affect the vision as in our cases, following cataract surgery or blunt trauma. We believe that the vasoproliferative tumours in our cases are presumed to be idiopathic. Although the contusion injury precipitated the vitreous haemorrhage and made the patient symptomatic as in cases 2 and 3, perhaps the tumour existed before and maybe these lesions are prone to bleed because of vascular proliferation as a reactive process.
Treatment of VPTR consists of periodic observation, cryotherapy, laser photocoagulation, plaque radiotherapy, or other modalities like dye laser, transpupillary thermotherapy and photodynamic therapy may be considered according to the individual case to preserve vision. Macular pucker in association with peripheral vascular tumour may improve after cryotherapy9 or remain stable.10 It is generally suggested that parsplana vitrectomy and peeling of the epiretinal membrane be delayed for at least a few months, looking for a decrease in vascularity of the tumour as in case 3 the epiretinal membrane became insignificant over a 3-month period following cryotherapy. Vitrectomy11 when performed for an epiretinal membrane or traction retinal detachment can potentially lead to central visual improvement. Irvine et al12 described trans-scleral resection when the diagnosis is difficult or uncertain. Shields et al2 treated 54 of 129 vasoproliferative tumours with cryotherapy. Plaque radiotherapy may be considered for larger lesions as described by Heimann et al3 or in cryotherapy failure cases. Although the previous authors2,3 have treated many of their patients with plaque radiotherapy, the long-term effects of this treatment are not known yet.
In conclusion, it is important to recognize VPTR as clinically distinct lesions, which should be followed up periodically as they may lead to visual loss because of their exudative tendencies and other associated complications like vitreous haemorrhage, epiretinal membrane formation, subretinal proliferation, macular oedema, rubeotic glaucoma, etc. These lesions should be differentiated from other vascular or tumorous lesions of the ocular fundus as their prognosis and treatment are different.
References
Jerry A Shields, William L Decker, George E Sanborn, James J Augsburger, Richard E Goldberg . Presumed acquired retinal hemangiomas. Ophthalmology 1983; 90: 1292–1300.
Carol L Shialob, Jerry A Shialob, Jefferey Barrett, Patrick De Potter . Vasoproliferative tumors of the ocular fundus. Classification and clinical manifestation in 103 patients. Arch Ophthalmol 1995; 113: 615–623.
Heimann H, Bornfeld N, Vij O, Coupland SE, Bechaakisne, Kellner U, Forster MM . Vasoproliferative tumors of the retina. Br J Opthalmol 2000; 84: 1162–1169.
Marianne H, Smeél D, Cornelia M Mooy, G Seerp Baarsma, Diane EA Martman, Jar C Van Meurs . Histopathology of a vasoproliferative tumor of the ocular fundus. Retina 1998; 18: 470–472.
Laqua H, Wessing A . Peripheral retinal telangiectasis in adults simulating a vascular tumour or melanoma. Ophthalmology 1983; 90: 1284–1291.
Gray RH, Gregor ZJ . Acquired peripheral retinal telangiectasia after retinal surgery. Retina 1994; 14: 10–13.
Jampol LM, Goldbaum MH . Peripheral proliferative retinopathies. Surv Ophthalmol 1980; 25: 1–14.
Sahel JA, Frederick Jr AR, Pesavento R et al. Idiopathic retinal gliosis mimicking a choroidal melanoma. Retina 1988; 8: 282–287.
Schwartz PL, Fastenberg DM, Shakin JL . Management of macular puckers associated with retinal angiomas. Ophthalmic Surg 1990; 21(8): 550–556.
Laatikainen L, Immonen I, Summanen P . Peripheral retinal angiomalike lesion and macular pucker. Am J Ophthalmol 1989; 108: 563–566.
Richard H McDonald, Howard Schantz, Robert N Johnson, Gary W Abrams, Gary C Brown, Alexander J Bruwer . Vitrectomy in eyes with peripheral retinal angioma associated with traction macular detachment. Ophthalmology 1996; 103(2): 329–335.
Fiona Irvine, Neal O'Donnell, Ewan Kemp, William R Lee . Retinal vasoproliferative tumors. Arch Ophthalmol 2000; 118: 563–569.
Author information
Authors and Affiliations
Corresponding author
Additional information
Work carried out at Department of Ophthalmology Sunnybrook and Womens College Health Science Centre 2075 Bayview Avenue Suite M1-202A Toronoto, Ontario Canada M4N 3M5
Rights and permissions
About this article
Cite this article
Jain, K., Berger, A., Yucil, Y. et al. Vasoproliferative tumours of the retina. Eye 17, 364–368 (2003). https://doi.org/10.1038/sj.eye.6700311
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6700311
Keywords
This article is cited by
-
Ru-106 plaque radiotherapy for vasoproliferative tumors of retina: a 15-year single-center experience
International Ophthalmology (2020)
-
Histologie bei bilateral asymmetrischem vasoproliferativem Tumor der Retina
Der Ophthalmologe (2012)
-
Retinal vasoproliferative tumours
Eye (2010)
-
Is vasoproliferative tumour (reactive retinal glioangiosis) part of the spectrum of proliferative vitreoretinopathy?
Eye (2009)
