
Abstract
Background:
Neuroblastoma is the most common malignancy of infancy but little is known about the aetiological factors associated with the development of this tumour. A number of epidemiological studies have previously examined the risk associated with paternal occupational exposures but most have involved small numbers of cases. Here we present results from a large, population-based, case–control study of subjects diagnosed over a period of more than 30 years and recorded in the national registry of childhood tumours in Great Britain.
Methods:
A case–control study of paternal occupational data for 2920 cases of neuroblastoma, born and diagnosed in Great Britain between 1962 and 1999 and recorded in the National Registry of Childhood Tumours, and 2920 controls from the general population matched on sex, date of birth and birth registration district. Paternal occupations at birth, of the case or control child, were grouped by inferred exposure using an occupational exposure classification scheme. Conditional logistic regression was used to estimate odds ratios (ORs) and 95% confidence intervals (95% CI), for each of the 32 paternal occupational exposure groups.
Results:
Only paternal occupational exposure to leather was statistically significantly associated with neuroblastoma, OR=5.00 (95% CI 1.07–46.93). However, this association became non-significant on correction for multiple testing.
Conclusion:
Our findings do not support the hypothesis that paternal occupational exposure is an important aetiological factor for neuroblastoma.
Similar content being viewed by others


Main
Neuroblastoma is a tumour of the sympathetic nervous system (OMIM, 2009), and is the most common of the four embryonal tumours diagnosed in children. Tumours are most commonly found in the adrenal gland, the abdomen, the retroperitoneal area or the chest. In Britain, the tumour accounts for 6% of all cancers diagnosed in childhood (0–14 years), and about 90 cases, including ganglioneuroblastoma, are registered in the National Registry of Childhood Tumours (NRCT) each year. The majority of cases (86%) are diagnosed by 5 years of age, and they constitute 19% of all tumours diagnosed in infants under 1 year, being the most common single type of tumour in this age group (Stiller, 2007).
The early onset of this tumour may be related to aetiological factors that influence conception, pregnancy and early life, such as parental occupation. In view of this, we carried out a large, population-based, matched case–control study of data that relates to paternal occupational exposures at the time of birth of the case or control subject. A number of epidemiological studies have examined the possible association between paternal occupation and the occurrence of neuroblastoma in offspring, some examined paternal occupational exposures which are comparable to the 32 groups examined in our study (see Table 1). These included: case–control studies (Spitz and Johnson, 1985; Bunin et al, 1990; Wilkins and Hundley, 1990; Michaelis et al, 1996; Olshan et al, 1999; Kerr et al, 2000; Schüz et al, 2001; De Roos et al, 2001a, 2001b, 2001c; Pearce et al, 2006, 2007); a cohort study (Feychting et al, 2000)); and a population-based study by (Carlsen, 1996) which compared cases of neuroblastoma which present at different ages (see Table 2 for more details of each study). The results of these studies were inconclusive and the estimates reported were often based on small numbers.
Patients and methods
The selection of cases and controls
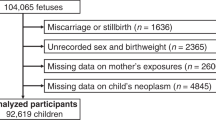
The population-based NRCT included 3219 cases of neuroblastoma born and diagnosed between 1962 and 1999, for 2920 cases (91%) a birth record was available. The remaining 299 cases, who were born or diagnosed overseas, adopted or not traced in the birth registers, were excluded from the study. The birth record for one control child per case matched on sex, date of birth (within 6 months), and birth registration sub-district was selected from the Office for National Statistics (ONS) or General Register Office in Scotland (GROS) birth registers.
Oxfordshire Research Ethics Committee (Oxfordshire REC C, Ref 07/Q1606/45) approved the use of the data reported in this study in 2007.
Coding of occupational data and derivation of the occupational exposure groups
Paternal occupation (part of the public record of birth registrations) was abstracted verbatim from the birth records and coded according to the 1980 Classification of Occupations (Office of Population Censuses and Surveys, 1980). The occupations were coded ‘blind’ to case or control status, independently by two coders. A third coder then recoded occupations where there were discrepancies, occupations coded differently by all three were reviewed by a fourth coder. At the end of this process 71 occupations remained uncertain and were coded as ‘inadequately described.’ The 1980 codes were converted to the 1970 Classification of Occupations (Office of Population Censuses and Surveys, 1970) using an automated recoding scheme. The occupations were classified as to whether or not they involved definite contact (i.e., every day or at very high levels) with any of the 33 exposures listed in Table 1, (see (Fear et al, 1999) for more details). Some occupations were classified in more than one exposure group, for example ‘bus conductors’ were included in the following exposure groups: ‘exhaust fumes’, ‘inhaled hydrocarbons’ and ‘social contact’.
Some 261 birth records did not have a paternal occupation recorded and were coded as ‘missing data’ in all exposure groups. The 71 ‘inadequately described’ occupations (described above) and 18 occupations that could not be converted to the 1970 coding scheme, were considered in the analyses as ‘unexposed’ to all of the exposure groups.
Analysis
Conditional logistic regression analyses (Breslow and Day, 1980) were carried out. As some of the exposure groups contained small numbers of exposed fathers, the analyses were carried out with LogXact 7 (2005) so that exact methods of statistical inference could be used. The exposure group ‘tobacco dust’ contained no case or control fathers. Odds ratios (ORs) and 95% confidence intervals (95% CI) were calculated for the remaining 32 exposure groups. Statistically significant results were defined as those where the P-value was <0.05. Any statistically significant ORs reflecting associations not previously reported in the literature were adjusted for multiple testing using the Bonferroni method (Bland and Altman, 1995).
Results
The study population is described in terms of age at diagnosis and sex in Table 3. Table 1 shows our results for 32 exposure groups. One estimate of risk was statistically significant, that for exposure to ‘leather’ OR=5.00 (95% CI 1.07–46.93). However, after adjustment for multiple testing, this OR was no longer significant. The 12 case or control fathers in this exposure group had the following occupational titles: ‘clicker (shoe company)’, ‘shoe operative’ (n=2), ‘shoe worker’ (n=2), ‘leather cutter’, ‘leather worker’, ‘shoe repairer/journeyman’ (n=2), ‘tanner (fellmongers)’, ‘machine operator (brush factory)’, ‘boot and shoe operative (men's moulding)’.
Discussion
Our findings for most exposure groups were unremarkable, with most ORs being around one. The only significantly raised risk – for the children of fathers exposed to leather – became non-statistically significant on correction for multiple testing. Estimated risks quoted in other epidemiological studies have varied in direction and magnitude. When comparing our results with those of other studies (listed in Table 2), it should be noted that in some of these studies information on occupational exposures has been collected from different sources, occupations and exposures were grouped using different classification schemes and in some studies the timing of the father's occupational exposure, with respect to the child's birth and diagnosis, was different from that in our study, which was ‘at birth’.
Many studies have found no significantly raised risks for the occupational exposure groups we studied. Below we discuss statistically significant findings for comparable groups of exposures from other studies.
Agrochemicals
Our estimates for the varied group of occupational titles classified as having exposure to ‘agrochemicals’ were not directly comparable to the statistically significant findings from other studies quoted for specific exposure to ‘pesticides’, ‘herbicides’ or ‘insecticides’ (Michaelis et al, 1996; Schüz et al, 2001; Pearce et al, 2006).
Electromagnetic fields
Spitz and Johnson (1985) reported a significantly raised risk for the offspring of men employed as ‘electricians, electric and electronics workers, linemen, utility employees, welders, electrical equipment salesmen and repairmen’: OR=2.13 (95% CI 1.05–4.35). This risk increased when the analysis was restricted to ‘electronics workers’ only, OR=11.75 (95% CI 1.40–98.55). Later studies (Bunin et al, 1990; Wilkins and Hundley, 1990; Olshan et al, 1999; Feychting et al, 2000; Kerr et al, 2000; De Roos et al, 2001b, 2001c; Pearce et al, 2007) reported non-significant estimates of risk (in both directions) for paternal occupational electromagnetic field exposures. The result of our study is in line with these later investigations.
Metal and lead
Results for ‘Metal’ from earlier published studies were non-significant, (Wilkins and Hundley, 1990; Michaelis et al, 1996; Olshan et al, 1999; Kerr et al, 2000; De Roos et al, 2001a, 2001c). Carlsen (1996) did not quote a relative risk but examined the frequency of paternal job titles for neuroblastoma cases from two birth cohorts split by age at diagnosis, and noted that the percentage of fathers employed in the ‘manufacture of iron and metal structures’ was ‘rather high’. Kerr et al (2000) reported a statistically significant raised estimate of risk for lead: OR=2.4 (95% CI 1.2–4.8). Our findings for exposure to lead, based on larger numbers, did not support this finding.
Coal dust
Kerr et al (2000) reported a raised risk for ‘coal soot’, OR=5.9 (95% CI 1.0–60.4, based on six case and two control fathers). Our estimate for ‘coal dust’ was much lower and not statistically significant.
Interpreting the results of this study
Despite the size of our study, it has limited power for some exposure groups. However, these data represent all cases of neuroblastoma in a large national population-based registry, and the study is much larger than any previously reported. Exact methods of statistical inference were used to take account of the small numbers in some exposure groups.
Where there is an exposure prevalence in the controls of 3% for a particular exposure group, the study has more than 80% power to detect an OR of 1.5 in that group. Eleven of the exposure groups we examined: construction, electromagnetic fields, exhaust fumes, forces, hydrocarbons (inhaled and dermal), lead, metal, metal working (oil mists), solvents and social contact had at least this prevalence of exposure in the control group. Of these groups, paternal exposure to: ‘electromagnetic fields’, ‘metal’ and ‘lead’ had previously been reported as significantly associated with an increased risk of childhood neuroblastoma. There were no significant results reported for ‘construction’ or ‘solvents’. There were no comparable groups reported in other studies for the remaining six groups.
In our study the occupation was recorded before the diagnosis of neuroblastoma, eliminating the possibility of recall bias. Occupations were coded, and discrepancies resolved, ‘blind’ to case–control status and were allocated to exposure groups within an exposure classification scheme devised with the help of an occupational hygienist, which has been used in a number of other studies (Fear et al, 1998, 1999, 2007, 2009; McKinney et al, 2003; MacCarthy et al, 2009). It is possible that occupations may have been incorrectly assigned to an occupational code and hence assigned to an inappropriate exposure group. Given that the coding was undertaken blind to the status of each subject, any bias would be non-differential and this would usually be expected to bias the OR towards 1.00, obscuring a real relationship with the exposure group.
We do not have information about biomarkers of occupational exposure, and cannot adjust for the use of protective equipment. Unlike some earlier studies based on detailed information from questionnaires or interviews, we have no detailed information on the actual level or frequency of the occupational exposure. Also, occupational practices and exposures may have changed over the years covered by this study. Our study examines paternal occupation as recorded at the time of birth of the child, and occupations could have changed in the time between birth and diagnosis of neuroblastoma. As shown in Table 2, neuroblastoma is most often diagnosed at an early age, so this is less of a consideration than it might be for some other diagnostic groups.
Other possible risk factors may be acting as confounders in our study, these factors are reviewed in detail in the comprehensive literature review by Heck et al (2009). We thought that socio-economic status might be relevant to our study of occupational exposures; however, when we adjusted for the variable ‘manual’ or ‘non manual’ social class status of the father (a proxy for socio-economic status), our initial results were unchanged (data not shown). Heck et al (2009) reviewed data on socio-economic status in earlier studies and concluded that there was insufficient evidence to draw a conclusion about this as a risk factor for neuroblastoma. They did report that there was some evidence of a positive association with both maternal alcohol consumption and low birth weight, factors which could be indirectly correlated with socio-economic status, but on which we have no information.
Conclusion
We have carried out the largest case–control study of paternal occupation and neuroblastoma possible in Britain. However, our study still has limited power for many of the defined exposure groups. Differences in study design also make it difficult to examine how our results relate to previous findings for occupational exposures. We have outlined a number of limitations in our study methods. Bearing these in mind, our findings for the exposure groups we examined do not support the hypothesis that paternal occupational exposure is an important aetiological factor for neuroblastoma.
Change history
16 November 2011
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Bland JM, Altman DG (1995) Multiple significance tests: the Bonferroni method. BMJ 310: 170
Breslow NE, Day NE (1980) Statistical Methods in Cancer Research Volume 1 – The Analysis of Case-Control Studies IARC Scientific Publications No. 32. pp 248–279, International Agency for Research on Cancer: Lyon
Bunin GR, Ward E, Kramer S, Rhee CA, Meadows AT (1990) Neuroblastoma and parental occupation. Am J Epidemiol 131: 776–780
Carlsen NLT (1996) Neuroblastomas presenting in the first year of life: epidemiological differences from those presenting at older ages. Cancer Detect Prev 20: 251–261
De Roos AJ, Olshan AF, Teschke K, Poole C, Savitz DA, Blatt J, Bondy ML, Pollock BH (2001a) Parental occupational exposures to chemicals and incidence of neuroblastoma in offspring. Am J Epidemiol 154: 106–114
De Roos AJ, Poole C, Teschke K, Olshan AF (2001b) An application of hierarchical regression in the investigation of multiple paternal occupational exposures and neuroblastoma in offspring. Am J Ind Med 39: 477–486
De Roos AJ, Teschke K, Savitz DA, Poole C, Grufferman S, Pollock BH, Olshan AF (2001c) Parental occupational exposures to electromagnetic fields and radiation and the incidence of neuroblastoma in offspring. Epidemiology 12: 508–517
Fear N, Roman E, Reeves G, Pannett B (1999) Father's occupation and childhood mortality: analysis of routinely collected data. Health Stat Q 2: 7–15
Fear NT, Hey K, Vincent T, Murphy MFG (2007) Paternal occupation and neural tube defects: a case-control study based on the Oxford Record Linkage Study register. Paediatr Perinat Epidemiol 21: 163–168
Fear NT, Roman E, Reeves G, Pannett B (1998) Childhood cancer and paternal employment in agriculture: the role of pesticides. Br J Cancer 77: 825–829
Fear NT, Vincent TJ, King JC, MacCarthy A, Bunch KJ, Murphy MFG (2009) Wilms tumour and paternal occupation: an analysis of data from the national registry of childhood tumours. Pediatr Blood Cancer 53: 28–32
Feychting M, Floderus B, Ahlbom A (2000) Parental occupational exposure to magnetic fields and childhood cancer (Sweden). Cancer Causes Control 11: 151–156
Heck JE, Ritz B, Hung RJ, Hashibe M, Boffetta P (2009) The epidemiology of neuroblastoma: a review. Paediatr Perinat Epidemiol 23: 125–143
Kerr MA, Nasca PC, Mundt KA, Michalek AM, Baptiste MS, Mahoney MC (2000) Parental occupational exposures and risk of neuroblastoma: a case-control study (United States). Cancer Causes Control 11: 635–643
LogXact 7 (2005) Discrete Regression Software Featuring Exact Methods (version 7). Cytel Software Corporation: Cambridge, Massachusetts, USA
MacCarthy A, Bunch KJ, Fear NT, King JC, Vincent TJ, Murphy MFG (2009) Paternal occupation and retinoblastoma: a case-control study based on data for Great Britain 1962–1999. Occup Environ Med 66: 644–649
McKinney PA, Fear NT, Stockton D, on behalf of the UK Childhood Cancer Study Investigators (2003) Parental occupation at periconception: findings from the United Kingdom Childhood Cancer Study. Occup Environ Med 60: 901–909
Michaelis J, Haaf HG, Zöllner J, Kaatsch P, Krummenauer F, Berthold F (1996) Case control study of neuroblastoma in West-Germany after the Chernobyl accident. Klin Padiatr 208: 172–178
Office of Population Censuses & Surveys (1970) Classification of Occupations 1970. HMSO: London
Office of Population Censuses & Surveys (1980) Classification of Occupations 1980. HMSO: London
Olshan AF, De Roos AJ, Teschke K, Neglia JP, Stram DO, Pollock BH, Castleberry RP (1999) Neuroblastoma and parental occupation. Cancer Causes Control 10: 539–549
Online Mendelian Inheritance in Man, OMIM (TM) (2009) Baltimore, MD, John Hopkins University. MIM Number 256700. World Wide Web URL: http://www.ncbi.nlm.nih.gov/entrez/dispomim.cgi?id=256700
Pearce MS, Hammal DM, Dorak MT, McNally RJ, Parker L (2006) Paternal occupational exposure to pesticides or herbicides as risk factors for cancer in children and young adults: a case-control study from the North of England. Arch Environ Occup Health 61: 138–144
Pearce MS, Hammal DM, Dorak MT, McNally RJQ, Parker L (2007) Paternal occupational exposure to electro-magnetic fields as a risk factor for cancer in children and young adults: a case-control study from the North of England. Pediatr Blood Cancer 49: 280–286
Schüz J, Kaletsch U, Meinert R, Kaatsch P, Spix C, Michaelis J (2001) Risk factors for neuroblastoma at different stages of disease. Results from a population-based case-control study in Germany. J Clin Epidemiol 54: 702–709
Spitz MR, Johnson CC (1985) Neuroblastoma and paternal occupation: a case-control analysis. Am J Epidemiol 121: 924–929
Stiller C (2007) Childhood Cancer in Britain: Incidence, Survival, Mortality. pp 68–70, Oxford University Press: Oxford
Wilkins JR, Hundley VD (1990) Paternal occupational exposure to electromagnetic fields and neuroblastoma in offspring. Am J Epidemiol 131: 995–1008
Acknowledgements
We are grateful to colleagues at the Childhood Cancer Research Group for help with this study, and to cancer registries and the Children's Cancer and Leukaemia Group for providing data to the National Registry of Childhood Tumours. We thank Brian Pannett and Krys Baker for their help in generating the recoding program and occupational exposure scheme. We are grateful to Gerald Draper and Charles Stiller for helpful discussions regarding this study. The Childhood Cancer Research Group receives Core Programme funding from the Department of Health and the Scottish Ministers. The funding agencies had no role in the design, conduct, reporting, or decision to publish the study. The views expressed here are those of the authors and not necessarily those of the Department of Health and the Scottish Ministers.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
MacCarthy, A., Bunch, K., Fear, N. et al. Paternal occupation and neuroblastoma: a case–control study based on cancer registry data for Great Britain 1962–1999. Br J Cancer 102, 615–619 (2010). https://doi.org/10.1038/sj.bjc.6605504
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bjc.6605504
This article is cited by
-
Agricultural exposures and risk of childhood neuroblastoma: a systematic review and meta-analysis
Environmental Science and Pollution Research (2023)
-
Case–control study of paternal occupational exposures and childhood bone tumours and soft-tissue sarcomas in Great Britain, 1962–2010
British Journal of Cancer (2020)
-
Case–control study of paternal occupational exposures and childhood lymphoma in Great Britain, 1962–2010
British Journal of Cancer (2019)
-
Childhood cancer research in Oxford II: The Childhood Cancer Research Group
British Journal of Cancer (2018)
-
Paternal occupational exposure to pesticides and risk of neuroblastoma among children: a meta-analysis
Cancer Causes & Control (2011)
