
Abstract
The optimal role for primary care in providing follow-up for men with prostate cancer is uncertain. A systematic review of international guidelines was undertaken to help identify key elements of existing models of follow-up care to establish a theoretical basis for evaluating future complex interventions. Many guidelines provide insufficient information to judge the reliability of the recommendations. Although the PSA test remains the cornerstone of follow-up, the diversity of recommendations on the provision of follow-up care reflects the current lack of research evidence on which to base firm conclusions. The review highlights the importance of transparent guideline development procedures and the need for robust primary research to inform future evidence-based models of follow-up care for men with prostate cancer.
Similar content being viewed by others


Main
Incidence rates of prostate cancer are rising in many countries, including the United Kingdom. It is now the most commonly diagnosed cancer in men in Europe (Ferlay et al, 2007) and the second most common male cancer worldwide (http://info.cancerresearchuk.org/cancerstats/types/prostate/incidence/). The numbers of men living with a diagnosis of prostate cancer will continue to increase as the population ages, and cancer is detected earlier with the more widespread use of prostate-specific antigen (PSA) testing.
Management options for localised and locally advanced prostate cancer include curative treatment, active surveillance and watchful waiting. The main curative treatments are radical prostatectomy, external beam radiotherapy (EBRT) and permanent (low-dose) brachytherapy. Hormone therapy (surgical or medical) may also be given as neoadjuvant, adjuvant or a stand-alone treatment for non-metastatic disease. Active surveillance is an option for men with low- or intermediate-risk localised disease that involves close monitoring to target curative treatment to those who would benefit most. Watchful waiting is a way to manage men who are unsuitable for curative treatment that involves relatively lax monitoring and palliative treatment when symptoms develop (NICE, 2008). Metastatic disease is treated palliatively with hormone therapy. Monitoring and post-treatment follow-up strategies aim to detect disease progression or recurrence, and manage long-term complications and treatment-related morbidity.
Traditionally, follow-up care has been hospital based and provided by clinical specialists in urology and oncology outpatient clinics. In practice, follow-up is provided in both primary and secondary care, and is not always well coordinated (Campbell et al, 2002; Neal, 2008) – this is despite widespread calls for better integrated care (Grunfeld, 2006; Oeffinger and McCabe, 2006; Department of Health, 2007; Nord et al, 2007). Further, there is evidence that prostate cancer patients are more likely to have a worse experience of care, including after care, than those with other cancers (Department of Health, 2005).
Various alternative models of cancer follow-up care have emerged, including nurse specialist and primary-care-led follow-up, and ‘shared care’ approaches. Only specialist nurse-led prostate cancer follow-up has been evaluated in randomised trials, which found it to be a safe alternative to consultant-led follow-up (Helgesen et al, 2000; Faithfull et al, 2001).
In the context of current widespread interest in greater involvement of primary care in cancer follow-up (Pascoe et al, 2004), we reviewed existing guidelines on follow-up for prostate cancer as part of a larger study to determine the optimal role for primary care. It is timely to review international guidelines to help (1) identify key elements of existing models of care and (2) establish a theoretical basis for evaluating future complex interventions.
Materials and methods
Search and selection
One reviewer performed the search and selection and a second reviewer verified the decisions on inclusion. Relevant guidelines were identified using the internet search engine SUMSearch, University of Texas, San Antonio, TX, USA (Hasse et al, 2007), followed by electronic searching of the individual websites of guideline collections (including clearinghouses and specialist libraries), guideline development agencies and professional societies, and finally the bibliographic databases MEDLINE, Bethesda, MD, USA and EMBASE (Elsevier, Amsterdam, The Netherlands). The searches were conducted from September to December 2007 with no language restriction. The sources searched are listed in Supplementary Table 1. References in the guidelines identified and personal contacts were consulted to identify additional guidelines. The pre-defined inclusion criteria were (1) the guideline was developed by a professional society or a national, regional, state or provincial government agency, (2) the guideline originated in the United Kingdom, Western Europe, Australia, Canada or the United States, (3) the guideline contained recommendations on post-treatment follow-up, active surveillance or watchful waiting, (4) the target group was primary or secondary health-care providers and (5) the date of issue was from 1990 onwards. Selection was thereby limited to current non-commercial guidelines and countries where the incidence of prostate cancer has risen over the past two decades and treatment options are similar.
Where necessary, the body that issued a potentially eligible guideline was contacted to obtain the full report. The most recent available version of updated guidelines was used. Additional reports and supporting material (such as journal articles and web pages) describing the guideline content, methods, development process or dissemination strategy, and tools for implementation were assembled for each included guideline.
Data extraction
One reviewer extracted data using a pro-forma that was checked by a second reviewer if the guideline was published in English. Data extraction from guidelines not published in English was based on translations. Data were extracted for the recommendations on follow-up (including strategies for active surveillance and watchful waiting as well as post-treatment follow-up), sources of evidence, criteria used to grade the quality of the evidence and strength of the recommendations, and the composition of the guideline development group.
Quality assessment
The Appraisal of Guidelines Research and Evaluation instrument was used to assess the quality of the included guidelines (www.agreecollaboration.org). It has 23 items in six domains: scope and purpose, stakeholder involvement, rigour of development, clarity and presentation, applicability and editorial independence. Assessing a guideline involves assigning each item a score of 1 (low) to 4 (high) and calculating a composite score for each domain. Domain scores are not aggregated. Two reviewers independently assessed the guidelines published in English. Assessment of foreign language guidelines was based on translations, supporting materials available in English and direct appraisal by native speakers to obtain, as far as possible, two independent appraisals.
Results
Included guidelines
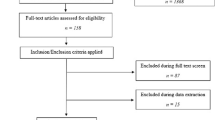
Forty-one potentially eligible guidelines were identified. Eighteen met the inclusion criteria – these are described in Table 1 and are marked with an asterisk in the reference list. One was still in preparation. The 22 excluded guidelines are listed in Supplementary Table 2. The included guidelines were published between 1999 and 2008: 11 originated in Europe (three in the United Kingdom), three in the United States and four in Canada; 11 were produced by professional societies and seven by government agencies; and 13 were published in English, two in French and one each in Dutch, Finnish and Swedish. The scope of most of the guidelines is prostate cancer management (COIN, 1999; BCCA, 2001; ESMO, 2006; CCNS, 2006; ACB, 2007; CBO, 2007; EAU, 2007; FCCG, 2007; NCCN, 2007; SBHW, 2007; NICE, 2008); one is specific to follow-up (AFU, 2005); one is restricted to management of non-metastatic disease (SOR, 2006); and two are specific to permanent brachytherapy for localised disease (ESTRO, 2000; ACR, 2005). One guideline (OMHLTC, 2002) and one best practice policy statement (AUA, 2000) on PSA, and a guidance document on urological cancer (including prostate cancer) services (NICE, 2002) were also included.
Guideline quality
Of the 18 guidelines reviewed, only the recent UK (NICE, 2008), Dutch (CBO, 2007) and Finnish (FCCG, 2007) guidelines, and the UK urological cancer services guidance (NICE, 2002), are of high overall quality according to the AGREE Collaboration's rating scheme, indicating that they could be considered for use in practice without provisos or alterations. The quality of the other 14 guidelines was either moderate (COIN, 1999; AUA, 2000; OMHLTC, 2002; ACR, 2005; CCNS, 2006; ESMO, 2006; SOR, 2006; SBHW, 2007) or low (ESTRO, 2000; BCCA, 2001; AFU, 2005; ACB, 2007; EAU, 2007; NCCN, 2007). The Collaboration considers low-quality guidelines to be more likely to have serious shortcomings and, therefore, not recommended for use in practice. The domain scores for each guideline are shown in Supplementary Table 3.
Most (14 out of 18) guidelines failed to describe their scope and purpose adequately, omitting details of the patient population to whom the guideline applied, the expected health benefits and the clinical questions they addressed. Six appeared to have been developed exclusively by clinical specialists (ESTRO, 2000; NICE, 2002; AFU, 2005; ESMO, 2006; SOR, 2006; EAU, 2007) and nine by multidisciplinary groups that also included other professionals from primary care (a GP or a specialist in family practice), nursing, psychology and social care (COIN, 1999; AUA, 2000; OMHLTC, 2002; CCNS, 2006; CBO, 2007; FCCG, 2007; NCCN, 2007; SBHW, 2007; NICE, 2008); three provided no information on the composition of the group (BCCA, 2001; ACR, 2005; ACB, 2007). Five guidelines involved patients, or their representatives or carers in the guideline development group, focus groups or in reviewing draft recommendations (COIN, 1999; NICE, 2002; OMHLTC, 2002; CBO, 2007; NICE, 2008); 13 gave no indication of having incorporated patients’ views or preferences. None of the guidelines were piloted in clinical practice before publication.
A third of the guidelines reported the sources searched to identify the supporting evidence (COIN, 1999; NICE, 2002; SOR, 2006; ACB, 2007; CBO, 2007; NICE, 2008). The quality of the evidence and the strength of the recommendations were graded using a wide variety of schemes. Most of the guidelines mentioned consensus in formulating the recommendations, yet none of them reported formal consensus procedures or fully described the methods used to reach final decisions or resolve disagreements. Only six provided clear and explicit links between the supporting evidence – or its absence – and the recommendations (AUA, 2000; SOR, 2006; CBO, 2007; FCCG, 2007; SBHW, 2007; NICE, 2008). Seven appeared not to have undergone external review before publication (ESTRO, 2000; BCCA, 2001; OMHLTC, 2002; ACB, 2007; EAU, 2007; NCCN, 2007; SBHW, 2007).
Ten of the guidelines had tools for application, as far as we could determine. In most cases, it was a single tool, such as a summary document or patient information. The recent UK guidelines were a notable exception, published together with a short version, quick reference guide and a patient information booklet (NICE, 2008).
The guidelines largely did not consider potential organisational barriers or the cost implications of applying the recommendations, or present review criteria for monitoring and audit. A conflict of interest statement of the guideline group members was missing from 11 of the 18 guidelines reviewed, and only one stated explicitly that the views and interests of the funding body did not influence the recommendations (CCNS, 2006).
Recommendations on follow-up
Service organisation
Most of the included guidelines did not address service organisation. The latest UK guidelines on prostate cancer (NICE, 2008) refer to the urological cancer services guidance (NICE, 2002) as the core model for service delivery, which stresses the importance of multidisciplinary team management. In all, nine of the guidelines mentioned the follow-up provider (who) or the setting (where). The UK guidelines show a shift over time from recommending that follow-up after treatment with curative intent takes place in a specialist unit (COIN, 1999) to offering appropriate patients follow-up outside hospital either by a specialist nurse or in primary care (NICE, 2002; NICE, 2008). Recent Dutch guidelines similarly recommend that a specialist nurse or GP can monitor PSA once it is stable (CBO, 2007), but do not require patients to be stable for 2 years before being given this option as stipulated in the UK guidelines (NICE, 2008). Contemporary Swedish and Finnish guidelines have divergent views: the former omitted the GP in recommending follow-up by a urologist, oncologist or specialist nurse, whereas in Finland, only the first post-treatment visit (after prostatectomy, EBRT or brachytherapy) takes place in secondary care with all subsequent follow-up in primary care (FCCG, 2007; SBHW, 2007). Recent guidelines issued in North America continue to recommend that patients are followed up by specialist clinicians after radical treatments (ACR, 2005; CCNS, 2008), although it was one Canadian guideline groups’ policy to refer patients back to the community ‘as far as practicable’ (BCCA, 2001).
Swedish guidelines specified that the urologist does active surveillance, whereas a specialist nurse or a GP can do watchful waiting (SBHW, 2007). In UK guidelines, watchful waiting should normally be provided in primary care, and primary care services have responsibility for the day-to-day management of men with metastatic disease (NICE, 2008). Similarly, according to Finnish guidelines, men undergoing hormone treatment receive all follow-up in primary care (FCCG, 2007).
Use of tests and examinations
Prostate-specific antigen testing: International guidelines agree on the fundamental role of PSA testing in prostate cancer follow-up, but recommendations on the frequency of tests and the duration of follow-up are highly inconsistent (Table 2). The recommended interval between PSA tests in the first year following prostatectomy or radical radiotherapy varies between 3 and 12 months. There is marked variation in the recommended frequency of routine testing relative to duration beyond the first year, irrespective of the type of treatment. The guidelines reflect the lack of consensus on the role of PSA following brachytherapy; those that do recommend regular testing differ in how often and for how long. Guidelines on active surveillance recommend a PSA test every 3–6 months, some increase the interval to 6 months only after the first 2 years (BCCA, 2001; NICE, 2008) or simply advise regular testing (AUA, 2000; NICE, 2002).
UK guidelines advise that men in watchful waiting should have at least one PSA test a year (NICE, 2008) in contrast to the specific (but different) test schedules in Swedish and French guidelines (AFU, 2005; SBHW, 2007). Overall, six guidelines contain similar recommendations on PSA test frequency after the initiation of hormone therapy, but three note that follow-up may need to be tailored to the needs of the patient depending on the type of hormone treatment, symptoms, clinical condition, age and prognosis (CCNS, 2006; ACB, 2007; EAU, 2007). Swedish guidelines recommend more frequent PSA tests for patients with metastases than for those without known metastases (SBHW, 2007) in contrast to one Canadian guideline that recommends routine PSA testing for advanced disease but not for metastatic disease (ACB, 2007).
There is also a high degree of variability between guidelines on what defines biochemical failure, that is, the change in PSA that should prompt further investigation (Supplementary Table 4). Most guidelines adopt expert panel standard definitions for biochemical failure following EBRT, but show a clear lack of consensus in regard to brachytherapy and prostatectomy – and a dearth of advice on active surveillance, watchful waiting and advanced disease.
Digital rectal examination and other tests: Guidelines on routine digital rectal examination (DRE) following treatment with curative intent fall into three categories: either it is not recommended (as long as PSA is stable) (CBO, 2007; NICE, 2008) or it is recommended supplementary to PSA testing, either with each PSA test (BCCA, 2001; OMHLTC, 2002; SOR, 2006; EAU, 2007) or less frequently (AFU, 2005; CCNS, 2006; ACB, 2007; NCCN, 2007) (Table 3). The type of curative treatment, prostatectomy or radiotherapy, does not explain these conflicting recommendations. It is also evident that there is no consensus on the use of DRE following brachytherapy. Six guidelines recommend DRE in the course of active surveillance (AUA, 2000; NICE, 2002; OMHLTC, 2002; CCNS, 2006; NCCN, 2007; SBHW, 2007) in contrast to the NICE guidelines’ recommendation against it as long as PSA remains at baseline levels (NICE, 2008). The NICE guidelines also recommend against routine DRE for men undergoing watchful waiting (NICE, 2008). Guidelines that advised on DRE during routine follow-up after initiation of hormone therapy recommend that it should be performed with each PSA test (OMHLTC, 2002; EAU, 2007; NCCN, 2007).
Biopsy, and imaging and biochemical tests other than PSA feature irregularly in follow-up recommendations. Four European guidelines agree that routine biopsy and imaging is unnecessary following treatment with curative intent if patients are asymptomatic and PSA is low and stable (AFU, 2005; SOR, 2006; CBO, 2007; EAU, 2007). Active surveillance should include at least one re-biopsy according to UK guidelines that do not specify the timing (NICE, 2008); other guidelines recommend it within 18 months, then periodically (CCNS, 2006; NCCN, 2007) or every 3 years (BCCA, 2001). Dutch and French guidelines (AFU, 2005; CBO, 2007) do not recommend routine biochemistry, such as creatinine, transaminases and testosterone, for follow-up of asymptomatic patients following treatment with curative intent, but Swedish guidelines do include creatinine and haemoglobin in routine follow-up after curative radiotherapy as well as during active surveillance and watchful waiting (SBHW, 2007). Regular monitoring of creatinine, haemoglobin and liver function tests (alkaline phosphatase or alanine aminotransferase) is recommended in European Association of Urology guidelines on metastatic disease and in concurrent Swedish guidelines on follow-up after hormone therapy (EAU, 2007; SBHW, 2007).
Complications and adverse effects
Specific recommendations on the evaluation of complications and treatment-related adverse effects appear infrequently in guidelines: those for Nova Scotia singularly recommend establishing a specific schedule of follow-up visits after radical treatment to discuss and manage urinary incontinence, erectile dysfunction and sexual health, and suggest routine screening for men considered to be at high risk for psychosocial distress throughout the course of the disease (CCNS, 2006). UK guidelines recommend that men and their partners are given the opportunity to discuss psychosexual problems (NICE, 2008) and that counselling on sexual problems and incontinence is made available for as long as it is needed (NICE, 2002).
Discussion
This study is the first to review prostate cancer guidelines systematically and to summarise international guideline recommendations on follow-up. Although monitoring PSA remains the cornerstone of follow-up for men with prostate cancer, the diversity of guideline recommendations on the frequency and duration of PSA testing, and components of follow-up other than PSA testing, reflects the current lack of research evidence on which to base firm conclusions. The guidelines provide only broad frameworks for evaluating potential intervention models of follow-up care, particularly in terms of the setting and the composition of the health-care team.
In conducting this review, we had a specific interest in the role of primary care in prostate cancer follow-up. The included guidelines illustrate the disagreement that persists on the extent to which primary care should be involved. The recommendations in recent guidelines that highlight primary-care-based follow-up would require considerable effort and investment to implement – in terms of education, protocols and strategies to change established practice (Grol et al, 1998; Foy et al, 2002). Furthermore, cancer follow-up in the community requires a close cooperation between primary and secondary care services. However, there has been little research on the best way to manage processes of care involving related actions and decisions by different care providers and, as this review shows, practice guidelines seldom address implementation (Grol et al, 2003). Guidelines recommending follow-up in the community give only general guidance, such as agreeing shared care protocols, maintaining close contact between all professionals involved and having mechanisms in place to allow primary care providers access to specialist services. With the current focus on integrated models of chronic care, there are, again, limitations on the usefulness of existing guidelines (Barr et al, 2003).
The paucity of high-quality studies in the literature on prostate cancer follow-up has important implications, particularly for primary care, because recommendations based on explicit and non-conflicting scientific evidence are adhered to more in general practice (Grol et al, 1998). It underlines the importance of strengthening the evidence base on prostate cancer follow-up and keeping guidelines up to date as new evidence emerges.
Our review has some limitations to consider. Identifying guidelines largely through electronic sources may have introduced bias towards English language guidelines and guidelines produced by larger, well-established organisations. Conversely, searching multiple sources, using foreign language search terms and pre-defining inclusion criteria on guideline developers, should have reduced the risk of language bias and failing to identify guidelines from eligible sources. We acknowledge that all relevant information may not have been included in the translations of foreign language guidelines and that quality assessment based on translations may not be entirely accurate. Nevertheless, our findings are consistent with earlier studies that have noted conflicting guideline recommendations on prostate cancer diagnosis and treatment (Meyer et al, 2006) and shortcomings in the methods used by leading urological associations to develop guidelines for prostate cancer (Dahm et al, 2007). The guidelines we reviewed were produced in developed countries with similar prostate cancer incidence trends and management options, consequently our findings may not be generalisable to other settings.
The methodological quality of the guidelines included in our review was heterogeneous and in most cases moderate to poor. We used the AGREE instrument as the indicator of guideline quality because it is validated and considered to be the international standard in guideline assessment (Vlayen et al, 2005). The criteria mainly address the methods of guideline development and the quality of reporting. The high-quality guidelines in this review were generally well reported and achieved high scores on almost all domains. However, inadequate and incomplete reporting cannot be ruled out as a reason for lower quality scores (Fervers et al, 2005). Guidelines of similar methodological quality still differ in their recommendations on prostate cancer follow-up, indicating that important influences on guideline development are not always explicit. Furthermore, in common with other critical appraisal tools for guidelines, the AGREE instrument does not assess the clinical content of the recommendations or the quality of the supporting evidence. Good methodological quality does not necessarily indicate good-quality recommendations (Burgers, 2006).
Most of the guidelines in our review combined an evidence-based approach with informal consensus – reflecting the status of the international literature in this field (Martin et al, 2006; Warren and McFarlane, 2007). When recommendations are formulated by consensus comprehensive stakeholder involvement, transparent consensus procedures and editorial independence are especially important for guideline credibility (Fervers et al, 2005). We found that these important elements are often not evident in prostate cancer guidelines. The balance between individual and speciality biases in guidelines development groups could, in part, account for different recommendations on who provides follow-up and in what setting. For example, guidelines recommending that clinical specialists provide follow-up were more likely to have been developed exclusively by representatives of that group. Those that recommend involvement of nurse specialists and primary care were largely developed by multidisciplinary groups that included a range of care providers and sought the views of service users. Research in other clinical areas has shown that speciality groups favour procedures in which they have a vested interest and even when presented with the same evidence will reach different conclusions than wider multidisciplinary groups (Murphy et al, 1998; Shekelle et al, 1999; Fretheim et al, 2006). Members of guideline development groups may also more readily endorse models of care that have already been implemented in their locality. When the consensus procedure is ill defined, it is difficult to ascertain which aspects might have influenced the outcome or how reliably expert opinion and stakeholders’ preferences were incorporated (Grol et al, 2003; Raine et al, 2005).
Reviews of international guidelines such as ours often find that recommendations are shaped or constrained by the structure and organisation of their country's health-care systems, even when the evidence is incontrovertible (Eisinger et al, 1999; Burgers et al, 2002; Philip et al, 2003). In the United Kingdom, for example, cancer plans (NHS, 2000; Department of Health, 2007) have emphasised patient preference on the delivery of cancer care and alternative models of health-care delivery, which bring care closer to the patient – these elements are reflected in the latest UK guidelines on prostate cancer (NICE, 2008).
Ultimately, the usefulness of a guideline needs to take account of the impact on patient outcomes of applying the recommendations in local settings. Systematic appraisal can aid informed judgment on guideline quality: guideline recommendations can only be rigorously tested by incorporating them in the development of interventions for evaluation in randomised trials.
Conclusions
This review shows the current status of international guidelines in prostate cancer follow-up. The variability in recommendations to some extent reflects the lack of definitive evidence from research in this field. Choices over management in prostate cancer, including follow-up, can only be informed to a limited extent by evidence from high-quality trials.
The review illustrates the importance of rigorous and transparent guideline development processes when research evidence is limited, without which it is difficult to assess factors such as independence and impartiality. It also highlights the need for robust primary research to improve the evidence base for prostate cancer follow-up – particularly research to inform best practice models of care. Only then can the many new models of care emerging internationally be shaped in a rational, evidence-based way.
Change history
16 November 2011
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
*Guidelines included in the review
*Alberta Cancer Board (2007) Clinical Practice Guideline Prostate Cancer. http://www.cancerboard.ab.ca/NR/rdonlyres/D9B8A40C-A089-45CE-8FAC-D7BBE6448FFA/0/GU_004_ProstateCancer.pdf [accessed 14 Jan 2009]
*American College of Radiology (2005) Practice guideline for transperineal permanent brachytherapy of prostate cancer. http://www.acr.org/SecondaryMainMenuCategories/quality_safety/guidelines/ro/brachy_prostate_cancer.aspx [accessed 14 Jan 2009]
*American Urological Association (2000) Prostate-specific antigen (PSA) best practice policy. Oncology 14: 267–286
*Ash D, Flynn A, Batterman J, de Reijke T, Lavagnini P, Blank L (2000) ESTRO/EAU/EORTC recommendations on permanent seed implantation for localized prostate cancer. Radiother Oncol 57: 315–321
Barr VJ, Robinson S, Marin-Link B, Underhill L, Dotts A, Ravensdale D, Salivaras S (2003) The expanded chronic care model: an integration of concepts and strategies from population health promotion and the Chronic Care Model. Hosp Q 7: 73–82
*British Colombia Cancer Agency (2001) Cancer Management Guidelines: Prostate. http://www.bccancer.bc.ca/HPI/CancerManagementGuidelines/Genitourinary/Prostate/Management/Followup/default.htm [accessed 14 Jan 2009]
Burgers JS (2006) Guideline quality and guideline content: are they related? Clin Chem 52: 3–4
Burgers JS, Bailey JV, Klazinga NS, Van der Bij AK, Grol R, Feder G, for the AGREE Collaboration (2002) Inside Guidelines. Comparative analysis of recommendations and evidence in diabetes guidelines from 13 countries. Diabetes Care 25: 1933–1939
Campbell NC, MacLeod U, Weller D (2002) Primary care oncology: essential if high quality cancer care is to be achieved. Fam Pract 19: 577–578
*Cancer Care Nova Scotia (2006) Guidelines for the Management of Prostate Cancer. http://www.cancercare.ns.ca/site-cc/media/cancercare/ProstateGuidelinesFullVersion2006(1).pdf [accessed 24 Apr 2009]
Dahm P, Kunz R, Schünemann H (2007) Evidence-based clinical practice guidelines for prostate cancer: the need for a unified approach. Curr Opin Urol 17: 200–207
Department of Health (2005) Tackling Cancer: Improving the Patient Journey. The Stationery Office: London
Department of Health (2007) Cancer reform strategy. http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/dh_081006 [accessed 31 July 2008]
*Dutch Institute for Healthcare Improvement (CBO) (2007) Prostate cancer Guidelines: diagnosis and treatment [Dutch]. http://www.cbo.nl/product/richtlijnen/folder20021023121843/rl_prostaat_carc_2007.pdf [accessed 14 Jan 2009]
Eisinger F, Geller G, Burke W, Holtzman NA (1999) Cultural basis for differences between US and French clinical recommendations for women at increased risk of breast and ovarian cancer. Lancet 353: 919–920
*European Association of Urology (2007) Guidelines on prostate cancer. http://www.uroweb.org/fileadmin/tx_eauguidelines/Prostate%20Cancer.pdf [accessed 14 Jan 2009]
*European Society for Medical Oncology (2007) Prostate cancer: ESMO Clinical Recommendations for diagnosis, treatment and follow-up. Ann Oncol 18 (Suppl 2): ii36–ii37
Faithfull S, Corner J, Meyer L, Huddart R, Dearnaley D (2001) Evaluation of nurse-led follow up for patients undergoing pelvic radiotherapy. Br J Cancer 85: 1853–1864
Ferlay J, Autier M, Boniol M, Heanue M, Colombet M, Boyle P (2007) Estimates of the cancer incidence and mortality in Europe in 2006. Ann Oncol 18: 581–592
Fervers B, Burgers JS, Haugh MC, Brouwers M, Browman GCF, Philip T (2005) Predictors of high quality clinical practice guidelines: examples in oncology. Int J Qual Health Care 17: 123–132
*Finnish Medical Society Duodecim Current Care Guidelines (FCCG) (2007) Prostate cancer [Finnish]. http://www.kaypahoito.fi/kh/kaypahoito?suositus=hoi11060 [accessed 14 Jan 2009]
Foy R, MacLennan G, Grimshaw J, Penney G, Campbell M, Grol R (2002) Attributes of clinical guidelines recommendations that influence change in practice following audit and feedback. J Clin Epidemiol 55: 717–722
*French Federation of Comprehensive Cancer Centres (2006) Clinical practice recommendations, Standards, Options and Recommendations for the management of nonmetastatic prostate cancer [French]. http://www.sor-cancer.fr/index.php?tg=fileman&idx=get&inl=1&id=2&gr=Y&path=organes+genitaux+masculins%2Fcancer+de+la+prostate%2Fcancer+de+la+prostate&file=Bulletin+de+synth%E8se+2006.pdf [accessed 14 Jan 2009]
Fretheim A, Schünemann HJ, Oxman AD (2006) Improving the use of research evidence in guideline development: 3. Group composition and consultation process. Health Res Policy Syst 4: 15
Grol R, Cluzeau FA, Burgers JS (2003) Clinical practice guidelines: towards better quality guidelines and increased international collaboration. Br J Cancer 89: S4–S8
Grol R, Dalhuijsen J, Thomas S, in’t Veld C, Rutten G, Mokkink H (1998) Attributes of clinical guidelines that influence use of guidelines in general practice: observational study. BMJ 317: 858–861
Grunfeld E (2006) Looking beyond survival: how are we looking at survivorship? J Clin Oncol 24: 5166–5169
Hasse A, Follmann M, Skipka G, Kirchner H (2007) Developing search strategies for clinical practice guidelines in SUMSearch and Google Scholar and assessing their retrieval performance. BMC Med Res Methodol 7: 28
Helgesen F, Andersson SO, Gustafsson O, Varenhorst E, Goben B, Carnock S, Sehlstedt L, Carlsson P, Holmberg L, Johansson JE (2000) Follow-up of prostate cancer patients by on-demand contacts with a specialist nurse: a randomized study. Scand J Urol Nephrol 34: 55–61
Martin RM, Gunnell D, Hamdy F, Neal D, Lane A, Donovan J (2006) Continuing controversy over monitoring men with localized prostate cancer: a systematic review of programs in the prostate specific antigen era. J Urol 176: 439–449
Meyer J-P, Sullivan ME, Bell RCRW (2006) Urological cancer guidelines: are there any differences? BJU Int 98: 940–941
Murphy MK, Black NA, Lamping DL, McKee CM, Sanderson CFB, Askham J (1998) Consensus development methods, and their use in clinical guideline development. Health Technol Assess 2 (3): 1–88
Neal RD (2008) The role of the GP in prostate cancer care. Trends Urol Gynaecol Sex Health 13: 27–30
NHS (2000) The NHS Cancer Plan. http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4009609 [accessed 11 November 2008]
Nord C, Ganz PA, Aziz N, Fosså SD (2007) Follow-up of long-term cancer survivors in the Nordic countries. Acta Oncol 46: 433–440
Oeffinger KC, McCabe M (2006) Models for delivering survivorship care. J Clin Oncol 24: 5117–5124
*Ontario Ministry of Health and Long-Term Care (2002) Ontario prostate specific antigen (PSA) clinical guidelines. http://www.health.gov.on.ca/english/providers/pub/cancer/psa/psa_guide/psa_mdref.pdf [accessed 14 Jan 2009]
Pascoe SW, Neal RD, Allgar VL, Selby PJ, Wright EP (2004) Psychological care for cancer patients in primary care? Recognition of opportunities for cancer care. Fam Pract 21: 437–442
Philip T, Fervers B, Haugh M, Otter R, Browman G (2003) European cooperation for clinical practice guidelines in cancer. Br J Cancer 89: S1–S3
Raine R, Sanderson C, Black N (2005) Developing clinical guidelines: a challenge to current methods. BMJ 331: 631–633
*Richaud P, Moreau J-L, Beuzeboc P, Rébillard X, Villers A, Peyromaure M, Cornud F, Soulié M, Davin J-L (2005) Follow-up of prostate cancer [French]. Prog Urol 15: 586–592
Shekelle PG, Woolf SH, Eccles M, Grimshaw J (1999) Developing guidelines. BMJ 318: 593–596
*Swedish National Board of Health and Welfare (SBHW) (2007) National guideline for prostate cancer management [Swedish]. http://www.socialstyrelsen.se/NR/rdonlyres/C149EC33-888D-4E30-AE40-84DBA21D152F/7340/20071029.pdf [accessed 14 Jan 2009]
*The National Comprehensive Cancer Network (2007) NCCN Clinical Practice Guidelines in Oncology. Prostate Cancer. http://www.nccn.org/professionals/physician_gls/PDF/prostate.pdf [accessed 14 Jan 2009]
*The National Institute for Health and Clinical Excellence (NICE) (2002) Guidance on Cancer Services. Improving outcomes in urological cancers: The Manual. http://www.nice.org.uk/nicemedia/pdf/Urological_Manual.pdf [accessed 14 Jan 2009]
*The National Institute for Health and Clinical Excellence (NICE (2008) Prostate cancer: diagnosis and treatment. http://www.nice.org.uk/nicemedia/pdf/CG58FullGuideline.pdf [accessed 14 Jan 2009]
*The Royal College of Radiologists’ Clinical Oncology Information Network (1999) Guidelines on the management of prostate cancer. BJU Int 84: 987–1014
Vlayen J, Aertgeerts B, Hannes K, Serneus W, Ramaekers D (2005) A systematic review of appraisal tools for clinical practice guidelines: multiple similarities and one common deficit. Int J Qual Health Care 17: 235–242
Warren KS, McFarlane JP (2007) Is routine digital rectal examination required for the followup of prostate cancer? J Urol 178: 115–119
Acknowledgements
Other members of the Prostate Cancer Follow-up Group are R O’Brien, M Keller and J Belcher. We gratefully acknowledge assistance with data extraction and quality assessment from translators: Francoise Cluzeau, Elina Heikkilä, Henry Jensen, Taina Taskila and Maurits van Tulder. This project was funded by Cancer Research UK C12357/ A7536
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Supplementary Information accompanies the paper on British Journal of Cancer website (http://www.nature.com/bjc)
Supplementary information
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
McIntosh, H., Neal, R., Rose, P. et al. Follow-up care for men with prostate cancer and the role of primary care: a systematic review of international guidelines. Br J Cancer 100, 1852–1860 (2009). https://doi.org/10.1038/sj.bjc.6605080
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bjc.6605080
Keywords
This article is cited by
-
A qualitative study on healthcare professional and patient perspectives on nurse-led virtual prostate cancer survivorship care
Communications Medicine (2023)
-
Active surveillance for prostate cancer: a narrative review of clinical guidelines
Nature Reviews Urology (2016)
-
The role of the GP in follow-up cancer care: a systematic literature review
Journal of Cancer Survivorship (2016)
-
Comparing the costs of three prostate cancer follow-up strategies: a cost minimisation analysis
Supportive Care in Cancer (2016)
-
Comparison of biochemical failure rates between permanent prostate brachytherapy and radical retropubic prostatectomy as a function of posttherapy PSA nadir plus ‘X’
Radiation Oncology (2014)
