
Abstract
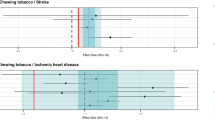
Among 309 male patients, those who had heavily consumed betel and tobacco were more likely than nonchewers (OR=2.91; 95% CI=1.36–6.25) and nonsmokers (OR=2.49; 95% CI=1.02–6.08) to develop cancer in the upper and middle third of the oesophagus, respectively; the effects of alcohol did not dominate in any third.
Similar content being viewed by others
Main
Our earlier study reported that habitual substance uses, including cigarettes, alcohol and areca, were the major risk factors for developing oesophageal squamous cell carcinoma in Taiwan (Wu et al, 2001). Although much research has investigated oesophageal cancer risk factors (Nandakumar et al, 1996; Phukan et al, 2001; Wu et al, 2001), only one study, to our knowledge, from India has examined the association between substance use and the anatomic site of oesophageal cancer lesions (Nandakumar et al, 1996). We therefore attempted to clarify the influence of substance use on the anatomical site of oesophageal cancer occurrence in Taiwan.
Materials and methods
Selection of subjects
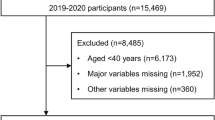
Over 6 years (1996–2002), we recruited 309 Taiwanese male patients with pathologically proved oesophageal squamous cell carcinoma from the National Taiwan University Hospital (Taipei), Kaohsiung Medical University Hospital and Kaohsiung Veterans General Hospital (Kaohsiung).
Subjects were interviewed by trained interviewers who collected demographic and substance use data by using a standardised questionnaire (Wu et al, 2001). This study was approved by Kaohsiung Medical University Hospital's IRB. Informed consent was obtained from all subjects. Information on habitual substance use included whether the subject had been a habitual areca chewer, cigarette smoker or alcoholic beverage drinker. Subjects who had smoked more than 10 cigarettes week−1 for at least 6 months were defined as cigarette smokers. Those who had regularly chewed betel quid for at least 6 months were defined as betel chewers. And those who had drunk beer, wine or distilled spirits more than one time week−1 for at least 6 months were defined as alcoholic beverage drinkers.
Location and staging classification of oesophageal cancer
Lesions were classified with respect to their location in the upper, middle or lower third of the oesophagus (Rosenberg et al, 1981; Chalasani et al, 1998). Upper-third lesions extended from the cricopharyngeal sphincter (15 cm) to the tracheal bifurcation (23 cm). Middle-third lesions extended from 23 cm to the approximate level of the T9 vertebral body (32 cm). Lower-third lesions extended from 32 cm to the gastro-oesophageal junction (40 cm). If the lesion involved more than one-third, both locations were recorded. The American Joint Committee on Cancer (AJCC) staging system was used (AJCC, 1988).
Statistical analysis
Unconditional logistic regression assessed the association between cancer location and substance use. Lesions in a given oesophageal third were compared to the remainder of the oesophagous.
For substance use, we used no cigarette smoking, no areca chewing and no alcohol consumption as baselines and compared these baselines to lifetime consumption. Users of substances were subdivided into two groups based on median levels of substance use. Lifetime consumption of tobacco was calculated by multiplying number of packs day−1 by the number of years smoked, yielding pack-years. Lifetime betel consumption was calculated by multiplying the average number of betel quids day−1 by the number of years chewed, yielding betel-years and alcohol by the number of years alcohol had been drunk (Wu et al, 2001). Variables in the models included age (>65 and ⩽65 years), educational level (⩾college, high school and ⩽elementary school) and substance use (tobacco, alcohol and areca). All P-values were two-sided.
Results
In total, 18.5% (57 out of 309), 41.7% (129 out of 309) and 26.5% (82 out of 309) of cancer lesions were located in the upper, middle or lower third of oesophagus, respectively (Table 1); 3.6% (11 out of 309) and 9.7% (30 out of 309) of cancers involved both upper and middle thirds or middle and lower thirds of the oesophagus, respectively.
Median cutoff points for lifetime consumption of these substances were 35 pack-years for smokers, 400 betel-years for areca chewers (about 20 betel quid day−1 for 20 consecutive years) and 32 years for alcoholic beverage drinkers. After adjusting for age (⩽65 vs >65 years), educational level (⩽primary school vs ⩾college and high schools vs ⩾college) and other substance use (tobacco and alcohol), we found that compared to nonchewers, subjects who had more than a 400 betel-year history were 2.91-fold more likely to develop cancer in the upper third of the oesophagus (95% CI=1.36–6.25) (Table 2). In addition, we found that subjects who had smoked more than 35 pack-years were 2.49-fold more likely to develop cancer in the middle third of the oesophagus than were nonsmokers (95% CI=1.02–6.08). Results remained similar after adjusting for clinical stage (>Stage II vs ⩽Stage II) (data not shown). In contrast, smokers were less likely to develop cancer in the lower third of oesophagus than were nonsmokers. We found no significant effect of alcohol consumption on the location of oesophageal cancer.
Discussion
Very few studies have investigated the relationship between habitual substance use and location of oesophageal cancer (Nandakumar et al, 1996). Nandakumar et al studied oesophageal cancer (343 cases and 686 controls) in India and found that chewing areca preparations were associated with an increased risk for developing cancer in the middle third of the oesophagus. In contrast, chewing tobacco was associated with lesions in the lower third.
In Taiwan, tobacco is smoked, instead of being added to areca preparations for chewing. Therefore, we speculate that the inhalation of carcinogens from cigarette smoking indirectly affects the oesophagus after entering into the blood stream via pulmonary capillary absorption. Our results agree with those of Nandakumar et al (1996) who also found that cigarette smoking more likely affected the middle rather than upper third of the oesophagus.
On the other hand, the association that we found between areca chewing and oesophageal cancer in the upper third differs from the findings of Nandakumar et al (1996). Areca is chewed and sometimes the areca juice is swallowed. Therefore, besides the oral cavity and pharynx, the first contact area of areca juice is the upper third of the oesophagus. Since chewing areca can cause oral and pharyngeal cancers (Ko et al, 1995; Lee et al, 2003), our findings suggest that lesions in the upper third of the oesophagus might be due to direct mucosal exposure to areca preparation contents.
In summary, we found that chewing areca and smoking cigarettes were associated with lesions in the upper and middle thirds of the oesophagus, respectively. Further studies need to examine whether tissue from areca-associated oesophageal cancer is associated with elevated levels of areca-associated DNA adducts in the upper third of oesophagus. In addition, our findings need to be confirmed in animal experiments.
Change history
16 November 2011
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
American Joint Committee on Cancer (AJCC) (1988) In: Manual for Staging of Cancer Beahrs OH, Henson DE, Hutter RVP, Myers MH (eds) 3rd edn, pp. 63–67. Philadelphia: JB Lippincott
Chalasani N, Wo JM, Waring JP (1998) Racial differences in the histology, location, and risk factors of esophageal cancer. J Clin Gastroenterol 26: 11–13
Ko YC, Huang YL, Lee CH, Chen MJ, Lin LM, Tsai CC (1995) Betel quid chewing, cigarette smoking and alcohol consumption related to oral cancer in Taiwan. J Oral Pathol Med 24: 450–453
Lee CH, Ko YC, Huang HL, Chao YY, Tsai CC, Shieh TY, Lin LM (2003) The precancer risk of betel quid chewing, tobacco use and alcohol consumption in oral leukoplakia and oral submucous fibrosis in southern Taiwan. Br J Cancer 88: 366–372
Nandakumar A, Anantha N, Pattabhiraman V, Prabhakaran PS, Dhar M, Puttaswamy K, Venugopal TC, Reddy NM, Rajanna, Vinutha AT, Srinivas (1996) Importance of anatomical subsite in correlating risk factors in cancer of the oesophagus – report of a case – control study. Br J Cancer 73: 1306–1311
Phukan RK, Ali MS, Chetia CK, Mahanta J (2001) Betel nut and tobacco chewing; potential risk factors of cancer of oesophagus in Assam, India. Br J Cancer 85: 661–667
Rosenberg JC, Franklin R, Steiger Z (1981) Squamous cell carcinoma of the thoracic esophagus: an interdisciplinary approach. Curr Probl Cancer 5: 1–52
Wu MT, Lee YC, Chen CJ, Yang PW, Lee CJ, Wu DC, Hsu HK, Ho CK, Kao EL, Lee JM (2001) Risk of betel chewing for oesophageal cancer in Taiwan. Br J Cancer 85: 658–660
Acknowledgements
This research was supported by grants from the Taiwan National Science Council (NSC 90-2320-B-037-040 and NSC 90-2320-B-037-052), the Taiwan National Health Research Institute (NHRI-CN-IN-9007P) and the Faculty Research Innovation Fund of Kaohsiung Medical University (Drs TF Chen and OL Chen).
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Wu, MT., Wu, DC., Hsu, HK. et al. Relationship between site of oesophageal cancer and areca chewing and smoking in Taiwan. Br J Cancer 89, 1202–1204 (2003). https://doi.org/10.1038/sj.bjc.6601251
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bjc.6601251
Keywords
This article is cited by
-
RETRACTED ARTICLE: Dépistage du cancer épidermoïde de l’œsophage par endoscopie chez les sujets à risque élevé de cancer
Acta Endoscopica (2010)
-
Dépistage du cancer épidermoïde de l’œsophage par endoscopie chez les sujets à risque élevé de cancer
Acta Endoscopica (2010)
-
Polymorphism in COX-2 modifies the inverse association between Helicobacter pyloriseropositivity and esophageal squamous cell carcinoma risk in Taiwan: a case control study
BMC Gastroenterology (2009)
-
Arecoline and the 30–100 kDa fraction of areca nut extract differentially regulate mTOR and respectively induce apoptosis and autophagy: a pilot study
Journal of Biomedical Science (2008)
