
Abstract
Data sources
An electronic search without time or language restrictions was undertaken using several databases: PubMed/Medline, Web of Science and the Cochrane Oral Health Group Trials Register and ongoing clinical trials. Manual searches were performed in dental implant related journals and reference lists of identified studies, and relevant reviews were scanned for possible additional studies.
Study selection
Eligibility criteria included human clinical studies, either randomised or not, comparing implant failure rates, MBL and/or post-operative infection in any group of patients receiving turned (machined) and anodised-surface (TiUnite) implants, both from the same implant manufacturer.
Data extraction and synthesis
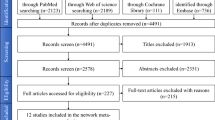
The titles and abstracts of all reports identified through the electronic searches were read independently by the three authors. For studies appearing to meet the inclusion criteria, or for which there were insufficient data in the title and abstract to make a clear decision, the full report was obtained. Disagreements were resolved by discussion between the authors. Quality assessment of the studies was executed according to the Newcastle-Ottawa scale (NOS), which is a quality assessment tool used when observational studies are also included in systematic reviews.
Results
Thirty-eight publications were included. The results suggest a risk ratio =2.82(95%CI, 1.95 – 4.06, P < 0.00001) for failure of turned implants when compared to anodised-surface implants. Sensitivity analyses showed similar results when only the studies inserting implants in maxillae or mandibles were pooled. There were no statistically significant effects of turned implants on the MBL (mean difference [MD]=0.02, (95%CI, 0.16 – 0.20; P = 0 82) in comparison to anodised implants. The results of a meta-regression considering the follow-up period as a covariate suggested an increase of the MD with the increase in the follow-up time (MD increase 0.012 mm year 1), however, without a statistical significance (P = 0.813). Due to lack of satisfactory information, meta-analysis for the outcome ‘post-operative infection’ was not performed.
Conclusions
Within the limitations of the existing investigations, the present study suggests that turned implants have a statistically higher probability to fail than anodised-surface implants, regardless of whether the implants were placed in maxilla or mandible. There were no statistically significant effects of turned implants on the MBL when compared with anodised implants. A comparison of post-operative infection between the implant types was not possible, due to lack of sufficient information. The reliability and validity of the data collected, the limitations of the quality assessment tool and the potential for biases and confounding factors are some of the shortcomings of the present study. The results have to be interpreted with caution due to the presence of several confounding factors in the included studies.
Similar content being viewed by others
Commentary
Dental Implants are feasible and predictable options for partially or fully edentulous patients. To achieve better primary stability and osteointegration, there are different studies about the microsurface of the implants. Anodised dental implants are machined implants types introduced in 2000. Anodisation is a procedure that consists of producing an electrolic stimulation to increase TiO2. The aim of these implants is to improve osteointegration by producing a combination of oxide texture and porosity. Turned implants are another classification that uses a polish manufacture process in order to get imperfection in their surface facilitating the osteoblastic cell apposition.1,2
The well organised systematic review and meta-analysis published in the Journal of Oral Rehabilitation had the purpose of comparing the survival rate of dental implants, marginal bone loss and post-operative infection of turned and anodised-surface dental implants.
The authors performed a vast search for published and unpublished trials about the topic and accepted 38 publications for the review.
The systematic review reported and analysed four randomised clinical trials, six controlled clinical trials, five prospective studies and twenty-three retrospective studies. Many of the included studies have a retrospective design, which is not the most appropriate design to evaluate interventions. Due to the different methodology, for quality assessment of the studies the authors used the Newcastle Ottawa Scale for non-randomised clinical trials, and they classified 23 studies as high quality and 15 as moderate quality.
For the outcome of implant failure, the authors combined 40 studies of varying designs, in a meta-analysis with a high statistical heterogeneity (the I2 calculated :84% ). The overall results presented in the forest plot are statistically significant (RR=2.82 CI (1-95-4.05) and favour the anodized dental implants.
In a different meta-analysis, the authors combined six studies that reported on implant failure in the maxilla. The overall result of the meta-analysis presents results favoring the anodized dental implants RR=2.54 CI (1.32- 4.89) with a high statistical heterogeneity of I2. 64%
An additional meta-analysis combined the results from studies that placed dental implants in the mandible. The overall results for implants are statisticall y significant, favoring the anodised dental implants RR=2.52 CI (1.27-4.97).
For marginal bone loss, the results were not statistically significant.
There are many factors that influence implant failure such as implant surface, immediate vs late loading, (occlusal forces may impair problems with osseointegration and bone loss), medical, social and dental history of the patient (for example periodontal disease, diabetes, smoking).3,4 Those factors were not described in the included studies so it's not possible to apply the results to the entire population.
As the authors concluded, the result of the review should be interpreted with caution due to biases and confounding factors.
References
Mishra SK, Kumar MA, Chowdhary R . Anodized dental implant surface. Indian J Dent Res 2017; 28:76–99.
Smeets R, Stadlinger B, Schwarz F, et al. Impact of Dental Implant Surface Modifications on Osseointegration. Biomed Res Int 2016; 2016:6285620.
De Bruyn H, Christiaens V, Doornewaard R, et al. Implant surface roughness and patient factors on long-term peri-implant bone loss. Periodontology 2000 2017; 73:218–227.
Troiano G, Lo Russo L, Canullo L, Ciavarella D, Lo Muzio L, Laino L . Early and late implant failure of submerged versus non-submerged implant healing: A systematic review, meta-analysis and trial sequential analysis. J Clin Periodontol 2018; 45:613–623.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Bruno R. Chrcanovic, Department of Prosthodontics, Faculty of Odontology, Malmo University, Carl Gustafs 34, SE-205 06, Malmo, Sweden. E-mail: bruno.chrcanovic@mah.se; brunochrcanovic@hotmail.com
Chrcanovic BR, Albrektsson T, Wennerberg A. Turned versus anodised dental implants: a meta-analysis. J Oral Rehabil. 2016; 43: 716–728. doi: 10.1111/joor.12415. [Epub ahead of print] Review. PubMed PMID: 27295394.
Rights and permissions
About this article

Cite this article
Reis, N., Bergamini, M., Silvestre, T. et al. Anodised or turned dental implants?. Evid Based Dent 19, 80–81 (2018). https://doi.org/10.1038/sj.ebd.6401325
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6401325
