
Abstract
Data sources
Cochrane Oral Health and Pregnancy and Childbirth's Trial Registries, Cochrane Register of Controlled Trials, Cochrane Library, Medline Ovid, Embase Ovid and LILACS BIREME, clinicaltrials.com and the WHO Clinical Trials Registry Platform were searched for published and ongoing trials until October of 2016.
Study selection
Randomised controlled trials (RCTs) investigating the effects of periodontal treatment in reducing or preventing perinatal and maternal morbidity and mortality with no exclusions of language or date of publication. Primary perinatal outcomes included: gestational age at birth, birth weight, small for gestational age and perinatal mortality, while the primary maternal outcomes included mortality, pre-eclampsia and treatment adverse effects.
Data extraction and synthesis
Two authors independently screened for inclusion and extracted data. Risk of bias was assessed using the Cochrane ‘risk of bias’ tool.
Dichotomous results were expressed as risk ratios (RR) with a 95% confidence interval (CI), and continuous data were expressed as mean differences (MD) with 95% confidence interval. Random-effects model was used for combining results.
The quality of the evidence was assessed using GRADE.
Results
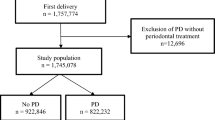
Fifteen studies with a total of 7,161 participants met the inclusion criteria.
Eleven studies (n = 5671) compared periodontal treatment with no treatment. For the outcome preterm birth before <37 weeks a calculated RR of 0.87, 95% CI 0.70-1.10 shows no clear difference. From seven studies (n = 3470) there is evidence that periodontal treatment may reduce birth weight <2500g (RR 0.77, 95% CI 0.48-0.95).
There is unclear evidence on the effect of periodontal treatment on preterm birth <35 weeks, <32 weeks, perinatal mortality and pre-eclampsia.
Three studies with 3,610 participants showed no evidence of difference in the outcome small for gestational age: RR 0.97, 95% CI 0.81-1.16.
Conclusions
There is no clear evidence that periodontal treatment during pregnancy has an effect on preterm birth. There is some evidence that it may reduce incidence of low birth weight.
There is insufficient evidence to define what type of periodontal treatment is superior in preventing any adverse pregnancy outcome.
Similar content being viewed by others

Commentary
Periodontal disease has been linked to multiple systemic diseases and conditions. As such, the treatment of periodontal disease should impact the disease or condition that it is linked to. However, supporting the link proved not to be as straightforward as one might think.
The effect of periodontal treatment on adverse pregnancy outcomes has been the topic of more than ten systematic reviews just in the last ten years, and provided inconsistent conclusions.
This quality review started with a clear question, outcome selection and a very comprehensive search strategy of multiple databases, two trial registries and reference lists of the included studies.
Two authors independently screened for inclusion, extracted data and assessed the risk of bias for randomised controlled trials that reported at least one obstetric outcome. The quality of the evidence was determined using GRADE. Fifteen studies with 7161 participants met the inclusion criteria while two await classification and one is ongoing.
The quality of the evidence was judged as being low to very low because of high bias risk, imprecision or very serious imprecision or serious inconsistency, and as such, likely to change with further research.
The authors pointed to some important considerations for future research. At the centre of those considerations is the lack of universally accepted criteria to establish periodontal status. Using a dichotomous approach for periodontal diagnosis instead of degrees of severity for inclusion or analysis may prove too simplistic and may miss potentially relevant outcomes for specific groups.
Eleven studies compare periodontal treatment with no treatment and the remaining four compare two periodontal treatments of different intensity or complexity. There was a wide range of the number of sessions, type of intervention, who administered treatment and the use of antimicrobials.
Variability from other sources is also present in the included studies. Important known factors like history of preterm birth were not reported in five of the included studies, while smoking status was included in some studies and treated as a reason for exclusion in others.
It is imperative to better address the important shortcomings of the present evidence.
Developing consensus on the criteria use for establishing periodontal status should become the first priority.
Purposely delaying treatment to individuals who could benefit most from it should be carefully considered, if only to improve general health.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Luisa Fernandez Mauleffinch, Managing Editor, Cochrane Oral Health Group, School of Dentistry, The University of Manchester, JR Moore Building, Oxford Road, Manchester, M13 9PL, UK. E-mail: luisa.fernandez@manchester.ac.uk
Iheozor-Ejiofor Z, Middleton P, Esposito M, Glenny AM. Treating periodontal disease for preventing adverse birth outcomes in pregnant women. Cochrane Database Syst Rev 2017; 6: Art. No.: CD005297. DOI: 10.1002/14651858.CD005297.pub3.
This paper is based on a Cochrane Review published in the Cochrane Library 2017, issue 6 (see www.thecochranelibrary.com for information). Cochrane Reviews are regularly updated as new evidence emerges and in response to feedback, and the Cochrane Library should be consulted for the most recent version of the review.
Rights and permissions
About this article

Cite this article
Spivakovsky, S. Periodontal treatment for the prevention of adverse birth outcomes. Evid Based Dent 19, 12–13 (2018). https://doi.org/10.1038/sj.ebd.6401286
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6401286
This article is cited by
-
20 years - 20 highlights
Evidence-Based Dentistry (2019)
