
Abstract
Data sources
Medline, Scopus, Web of Science, Latin American and Caribbean Health Sciences Literature database (LILACS), Brazilian Library in Dentistry (BBO), Cochrane Library, System for Information on Grey literature in Europe (SIGLE), ProQuest Dissertations and Theses, Periódicos Capes Theses database, Current Controlled Trials (www.controlled-trials.com), International Clinical trials registry platform (http://apps.who.int/trialsearch/), the ClinicalTrials.gov (www.clinicaltrials.gov), Rebec (www.rebec.gov.br) and EU Clinical Trials Register (https://www.clinicaltrialsregister.eu), abstracts of the annual conference of the International Association for Dental Research (IADR) and their regional divisions.
Study selection
Two reviewers selected studies; parallel or split-mouth randomised controlled trials (RCTs) comparing adhesive strategies were considered.
Data extraction and synthesis
Data were abstracted by two reviewers and into four follow up periods, 1 year; 18 months to 2 years; 3 years and 4 to 5 years. The Cochrane risk of bias tool was used to assess study quality. Data outcomes were dichotomous and summarised using relative risks and random effects meta-analysis.
Results
Twenty-nine studies were included in the meta-analysis. Bonding strategy did not influence postoperative sensitivity (risk ratio [RR] 1.04; 95% CI 0.81 to 1.34) or retention rates (RR = 1.04; 95% CI 0.81 to 1.34). The etch-and-rinse approach produced less marginal discoloration at 18 months to 2 years (RR 1.51; 95% CI 1.21 to 1.90) and at 4 to 5 years (RR 1.81; 95% CI 1.28 to 2.55) (p<0.0007).
Conclusions
Composite resin restorations placed with self-etch and etch-and-rinse adhesives produce restoration with similar clinical service and POS, however using etch-and-rinse adhesives one can reduce marginal discoloration.
Similar content being viewed by others
Commentary
Restoring non-carious cervical lesions with composite resin is common in dental practice given a cervical wear prevalence ranging from 11.4 to 62.2%.1 A dentist may choose different adhesive strategies such as etch-and-rinse or self-etch. Self-etch leaves a smear layer while etch-and-rinse removes all the smear layer thus theoretically may have less risk of postoperative sensitivity. The aim of this review was to assess if the risk of postoperative sensitivity (POS), retention rates and marginal discoloration of composite restorations (CR) bonded with self-etch (SE) in non-carious cervical lesions (NCCLs) of adults equals to etch-and-rinse (ER) adhesives.
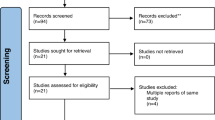
This review has been conducted using the Cochrane Collaboration's tool for assessing risk of bias in randomised trials. A large number of trials (n = 42 studies) have been included from a comprehensive list of databases and only low risk trials (n = 29 studies) were included for meta-analysis. Compared to other systematic reviews, the review authors clarified unclear risk of bias by directly contacting the authors of those studies. This rigorous approach is one of the strengths of this review and likely increases the validity of the result. The review authors reported details of their search strategy and analysis. They summarised all 29 included studies in terms of study design, sample size and clinical techniques used. The review authors used a set of criteria (random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data and selective reporting) to assess the risk of bias. They reported forest plots of all the risk ratios so readers can see the heterogeneity of the included studies in each outcome. One thing that is not very clear is how the review authors adjusted multiple teeth in one patient receiving restorations. The outcome variables would depend on the patient. A patient who is sensitive on one tooth may be more prone to develop postoperative sensitivity in other teeth.
This well-conducted meta-analysis found that for the postoperative sensitivity and retention there was no significant difference (POS risk ratio [RR] 1.04; 95% CI 0.81 to 1.34) between etch-and-rinse and self-etch adhesive strategies. However, etch-and-rinse system showed less marginal discoloration at 18 months to 2 years (RR 1.51; 95% CI 1.21 to 1.9) (p = 0.0003) and 4 to 5 years (RR 1.81; 95% CI 1.28 to 2.55) (p <0.0007) follow-up. This review finding is similar to those of previous studies with some discrepancies. Reis et al.s'2 systematic review also found no differences in postoperative sensitivity between ER and SE strategies for posterior composite restorations. On the other hand, Peumans et al.s'3 systematic review found ER and SE with mild acid (pH >1.5) showed adequate mean annual failure rates (2.5% and 3.1% respectively) while SE with stronger acid (pH <1.5) showed significantly higher mean annual failure rates (8.4%). This current systemic review did not differentiate SE with mild acid and SE with strong acid.
A clinician should consider several factors before applying this result to their practice. As the review authors pointed out, most of the included studies were conducted by highly calibrated clinicians using highly standardised clinical protocol which is different in individual practice settings. In addition, the clinical protocols varied in terms of placement technique (bulk or incremental), rubber dam use, mechanical preparation (beveling, roughening dentin, or no prep) and the adhesive and composite products/brands used. No comparison or conclusion was made about which technique or brand performed better. It also should be noted that how the studies measured postoperative sensitivity varied. Some studies used patient self-reported sensitivity while others used stimulus such as air or cold.
When a restoration is indicated for NCCLs, a clinician should remember he or she has a wide range of material choices: glass ionomers and composites with various bonding systems.4 Given the glass ionomer shows less retention failure and postoperative sensitivity, it would be a material of choice for a tooth with previous history of retention failure or postoperative sensitivity. If aesthetic is concerned or better mechanical property is required, a composite restoration with SE with mild acid or ER system would be a choice.
Practice point
-
When restoring non-carious cervical lesions using composite resin, both etch-and-rinse and self-etch systems resulted in similar post-op sensitivity and retention
-
Etch-and-rinse system performed better in marginal discoloration at follow-up 18 months and after.
References
Pecie R, Krejci I, García-Godoy F, Bortolotto T . Noncarious cervical lesions (NCCL)--a clinical concept based on the literature review. Part 2: restoration. Am J Dent 2011; 24: 183–192.
Reis A, Dourado Loguercio A, Schroeder M, Luque-Martinez I, Masterson D, Cople Maia L . Does the adhesive strategy influence the post-operative sensitivity in adult patients with posterior resin composite restorations?: A systematic review and meta-analysis. Dent Mater 2015; 31: 1052–1067.
Peumans M, De Munck J, Mine A, Van Meerbeek B . Clinical effectiveness of contemporary adhesives for the restoration of non-carious cervical lesions. A systematic review. Dent Mater 2014; 30: 1089–1103.
Pecie R, Krejci I, García-Godoy F, Bortolotto T . Noncarious cervical lesions (NCCL)--a clinical concept based on the literature review. Part 2: restoration. Am J Dent 2011; 24: 183–192.
Author information
Authors and Affiliations
Additional information
Address for correspondence: AD Loguercio, Department of Restorative Dentistry, School of Dentistry, State University of Ponta Grossa (UEPG), Rua Carlos Cavalcanti, 4748, Zip Code 84030-900, Campus Uvaranas, Ponta Grossa, Paraná, Brazil. E-mail: aloguercio@hotmail.com
Schroeder M, Correa IC, Bauer J, Loguercio AD, Reis A. Influence of adhesive strategy on clinical parameters in cervical restorations: A systematic review and meta-analysis. J Dent 2017; 62: 36–53.
Rights and permissions
About this article

Cite this article
Coe, J. Which adhesive strategy for non-carious cervical lesions?. Evid Based Dent 18, 119–120 (2017). https://doi.org/10.1038/sj.ebd.6401275
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6401275
