
Abstract
Data sources
Medline, Scopus and the Web of Science.
Study selection
Studies conducted in children under 16 undergoing general anaesthesia having change in oral health-related quality of life were considered. Selection was undertaken by two reviewers independently.
Data extraction and synthesis
Data abstraction was undertaken independently by three groups of two reviewers – discrepancies were resolved by discussion. Study quality was assessed using the Quality Assessment Tool for Studies of Diverse Design (QATSDD).
Results
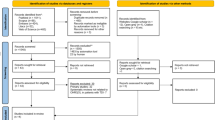
Twenty studies were included; there were 18 prospective studies, one randomised trial and one secondary analysis study. Most studies used a pre-test–post-test design and all but one used proxy measures of oral health-related quality of life (OHRQoL). All of the studies reported improved OHRQoL overall. However, results suggested that some aspects of OHRQoL may worsen.
Conclusions
Heterogeneity of included papers limited the conclusions which could be drawn. Treatment under GA appears to result in overall improvements in proxy-reported OHRQoL; however, there is a need for further high-quality studies employing validated, child-reported measures of OHRQoL.
Similar content being viewed by others


Commentary
Dental caries remains the most prevalent chronic childhood disease worldwide, exerting a negative impact on the oral health-related quality of life (OHRQoL) of children and their families.1,2 This highlights the importance of making normative criteria compatible with subjective criteria in the assessment of treatment need. In cases when there is severe dental pain, extensive dental caries lesions, uncooperative children or even children with special care needs, general anaesthetic (GA) can be a suitable option to provide adequate treatment.3 However, a careful analysis must be undertaken before choosing GA against other more conservative options3 due to associated morbidity and anxiety post procedure.4 The aim of this well-designed systematic review was to assess treatment-associated changes in OHRQoL of children following dental treatment under GA. One of the key features of systematic reviews is to appraise the methodological quality and provide evidence on a particular topic.5 The authors followed guidelines for undertaking systematic reviews and employed a comprehensive search strategy including several databases without year of publication or language restrictions, allowing a wide-ranging study identification. Authors used the Quality Assessment Tool for Studies of Diverse Design (QATSDD) with some modifications to assess the quality of studies. They set up three teams of two investigators to independently extract data for each paper, which lessened subjectivity in article selection and analysis. Also, an inter-reviewer agreement was performed, enhancing the reliability of the results.
A total of 20 studies were included in the final review, most of which had a prospective longitudinal design. Some results found in the review deserve considerations. Mean dmft/DMFT ranged from 6.9 to 13.3, which is a high mean value. The high caries experience was probably one of the reasons that guided the decision-making towards treating the children under GA. The majority of the selected studies used parental self-completed OHRQoL instruments to collect data, and two studies designed their own questionnaires. It is not a coincidence that these were also the oldest included studies in this review. The first OHRQoL questionnaires focused on children were published a little later, in 2002.6 Only one study used a child-reported measure of OHRQoL. Since parental and child reports measure different realities,7 it would be interesting if some studies had collected information from both children and parents to compare their perceptions regarding the choice for GA. Nine of the selected studies included validated instruments. This is a shortcoming, since the use of non-validated instruments restricts the reliability of the results. Loss to follow-up was reported in most of the studies, and this ranged from 0% to 47%. In the review, there was no mention about the main reasons for losses, which would be very enlightening.
Despite the significant heterogeneity in how the studies reported change in OHRQoL, all included studies reported an overall improvement in the OHRQoL of children following dental treatment under GA. Most of them found a significant change in both overall and subscale scores. It should be emphasised that this cannot be an effect of treatment under GA per se, but mainly the effect of relief from pain and discomfort.8 On the other hand, some studies found a worsening OHRQoL after dental treatment under GA. The review discussed some reasons for these intriguing results, such as the short time post-test questionnaires were administered in some studies, at which point children may still be experiencing discomfort from extraction sites. The review authors stated that children submitted to a high number of tooth extractions are more likely to experience the negative side effects of post-treatment discomfort or impaired function. When appraising data, the review found that different individuals completed the pre-test and post-test questionnaires, and this can also help explain the results. In future studies, a separation of children by burden of disease, number/complexity of treatments or even by procedures that can result in worse post-treatment symptoms should be more appropriate to help understand the responses.
Only three studies calculated the minimally important difference (MID). One strength aspect of including MID calculation is that it indicates whether the observed change is meaningful. The calculation showed the mean score changes were higher than the MID, justifying the interventions. Some studies assessed the effect sizes and found large-to-moderate effect sizes for overall changes and in all subscales. Nine studies reported secondary outcomes, such as the ongoing caries experience. These studies showed that children had a high number of new caries experiences a short time after the procedures under GA, confirming that dental treatment does not mean treatment of disease. A preventive approach is essential, with dietary recommendations, rational use of fluoride, regular dental care and oral hygiene instructions to both children and parents.9
Finally, the review judged the quality of the included studies. QATSDD scores for the individual studies ranged from seven to 32, out of a total possible score of 42. The low average (22 ± 7) score clearly reflects the overall poor methodological quality of the studies. Given the heterogeneity of the studies, a meta-analysis could not be carried out, limiting the conclusions of the review. Some quality criteria were well addressed in most studies, such as the fit between the research question and method of data collection and analysis. On the other hand, none of the included studies had evidence of user involvement in the design, and there was a lack of an explicit theoretical framework underpinning most studies. In addition, the approaches taken to sample size estimation and assessment of reliability and validity of the OHRQoL instruments used were other aspects less well addressed. Therefore, more studies with high-quality methodology are necessary on this topic.
Practice point
-
Using proxy reporting, the studies included in the review showed that dental treatment under GA had an overall improvement on OHRQoL of children, although further high-quality studies are needed.
-
Despite the effectiveness of dental treatment under GA, some included studies showed that children had a high number of new caries experiences shortly after the procedures, emphasising the importance of preventive care and public oral health promotion.
References
Martins-Júnior PA, Vieira-Andrade R G, Corrêa-Faria P, Oliveira-Ferreira F, Marques L S, Ramos-Jorge M L . Impact of early childhood caries on the oral health-related quality of life of preschool children and their parents. Caries Res 2013; 47: 211–218.
Naidu R, Nunn J, Donnelly-Swift E . Oral health-related quality of life and early childhood caries among preschool children in Trinidad. BMC Oral Health 2016; 16: 128.
Goodwin M, Sanders C, Davies G, Walsh T, Pretty I A . Issues arising following a referral and subsequent wait for extraction under general anaesthetic: impact on children. BMC Oral Health 2015; 15: 3.
Bridgman C M, Ashby D, Holloway P J . An investigation of the effects on children of tooth extraction under general anaesthesia in general dental practice. Br Dent J 1999; 186: 245–247.
Brignardello-Petersen R, Carrasco-Labra A, Glick M, Guyatt G H, Azarpazhooh A . A practical approach to evidence-based dentistry: understanding and applying the principles of EBD. J Am Dent Assoc 2014; 145: 1105–1107.
Jokovic A, Locker D, Stephens M, Kenny D, Tompson B, Guyatt G . Validity and reliability of a questionnaire for measuring child oral-health-related quality of life. J Dent Res 2002; 81: 459–463.
Jokovic A, Locker D, Guyatt G . How well do parents know their children? Implications for proxy reporting of child health-related quality of life. Qual Life Res 2004; 13: 1297–1307.
Ridell K, Borgström M, Lager E, Magnusson G, Brogårdh-Roth S, Matsson L . Oral health-related quality-of-life in Swedish children before and after dental treatment under general anesthesia. Acta Odontol Scand 2015; 73: 1–7.
American Academy of Pediatric Dentistry. Guideline on caries-risk assessment and management for infants, children, and adolescents. Pediatr Dent 2015; 37: 132–139.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Rebecca Knapp, Unit of Dental Public Health, School of Clinical Dentistry, Claremont Crescent, Sheffield S10 2TA, UK. E-mail: becky.knapp@sheffield.ac.uk
Knapp R, Gilchrist F, Rodd HD, Marshman Z. Operative caries management in adults and children. Change in children's oral health-related quality of life following dental treatment under general anaesthesia for the management of dental caries: a systematic review. Int J Paediatr Dent 2017; 27: 302–312.
Rights and permissions
About this article

Cite this article
Martins-Junior, P. Dental treatment under general anaesthetic and children's oral health-related quality of life. Evid Based Dent 18, 68–69 (2017). https://doi.org/10.1038/sj.ebd.6401249
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6401249
This article is cited by
-
Effectiveness of sensory adaptive dental environments to reduce psychophysiology responses of dental anxiety and support positive behaviours in children and young adults with intellectual and developmental disabilities: a systematic review and meta-analyses
BMC Oral Health (2023)
-
Quality assessment with diverse studies (QuADS): an appraisal tool for methodological and reporting quality in systematic reviews of mixed- or multi-method studies
BMC Health Services Research (2021)
-
The impact of dental caries and its treatment under general anaesthetic on children and their families
European Archives of Paediatric Dentistry (2021)
-
A rapid review of variation in the use of dental general anaesthetics in children
British Dental Journal (2020)
