
Abstract
Data sources
Cochrane Oral Health Group's Trials Register, the Cochrane Central Register of Controlled Trials (CENTRAL), Medline, Embase, LILACS, ISI Web of Science, ClinicalTrials.gov and the WHO International Clinical Trials Registry Platform.
Study selection
Randomised controlled clinical trials of analgesics given before dental treatment versus placebo or no analgesics in children and adolescents up to 17 years of age. Children and adolescents having dental treatment under sedation (including nitrous oxide/oxygen) or general anaesthesia were excluded.
Data extraction and synthesis
Two reviewers independently selected studies, abstracted data and assessed risk of bias. Standard Cochrane methodological approaches were used.
Results
Five trials involving 190 patients were included. None of the studies were at low risk of bias. Three trials involved dental treatment and two involved orthodontic treatment. Three of the included trials compared paracetamol with placebo. Meta-analysis of the two trials showed no evidence of a benefit in taking paracetamol preoperatively; (RR) for postoperative pain of 0.81 (95%CI; 0.53 to 1.22). Four trials compared ibuprofen with placebo. Pooled data from two studies showed a statistically significant mean difference in severity of postoperative pain of −13.44 (95%CI; −23.01 to −3.88) on a visual analogue scale (0 to 100), which indicated a probable benefit. Both trials were at high risk of bias and the quality of the evidence is low.
Conclusions
From the available evidence, we cannot determine whether or not preoperative analgesics are of benefit in paediatric dentistry for procedures under local anaesthetic. There is probably a benefit in using preoperative analgesics prior to orthodontic separator placement. The quality of the evidence is low. Further randomised clinical trials should be completed with appropriate sample sizes and well defined outcome measures.
Similar content being viewed by others

Commentary
The clearly defined question addressed in this Cochrane review is ‘do pre-operative analgesics reduce intraoperative or postoperative pain in children and adolescents having dental treatment.’
At present, use of pre-operative analgesia for dental treatment is rare, both amongst the adult and paediatric patient populations.
Post-operative analgesia may possibly be recommended by a dentist for child patients in verbal post-operative instructions, especially after preformed metal crown placement or root canal treatment. This will vary from clinician to clinician.
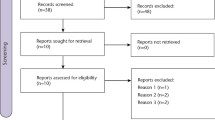
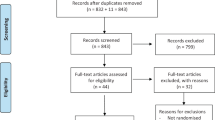
The authors of this publication carried out a comprehensive search of a number of electronic databases and hand-searched journals for suitable studies.
Unfortunately, none of the five studies which fulfilled the selection criteria and were included for analysis, was deemed of low or risk of bias following the methodology set out in the Cochrane Handbook for Systematic Reviews of Interventions.
When conducting research focusing on a paediatric sample population, there are important factors unique to child patients which are crucial to take into consideration.
It is important to ensure that the children selected to participate have the appropriate level of understanding to be able to provide reliable responses.
The researchers should ensure that they either focus on a narrow age range or have age appropriate resources (eg questionnaires1) for the range of ages involved in the study – to ensure that the questionnaires are neither patronising for older patients nor too advanced for younger or less mature patients. For example, smiley and sad faces can be incorporated into visual analogue scales to make them more ‘child-friendly.’2
The issue of consent/assent of the patient and their guardian should be given careful thought. It is important that future researchers take into consideration that a range of ages may involve patients who can consent to be involved in the study and require parental assent and also less mature patients who will assent to participation but consent must be gained from their parents.
A separate consideration for the treatment of paediatric dental patients is supporting them to co-operate with dental treatment. The use of preoperative analgesia will have negligible effect on this issue and communication tools and methods of behavioural management such as positive reinforcement, tell-show-do and modeling retain their value.3
However, if postoperative pain experience is proven to be reduced by a future study, this may in turn lead to a more positive overall experience of dental treatment by a child and therefore improve their attitude towards dentistry in general.
Inclusion of an anxiety assessment tool, completed by the children before and after key stages of the treatment plan, would make for interesting reading.
An important consideration for future studies would be the inclusion of potentially three arms – preoperative paracetamol, preoperative ibuprofen and preoperative placebo. In the UK, one in 11 children has asthma,4 meaning that ibuprofen is likely contraindicated as analgesia.5 These patients would not benefit from a study investigating the effect of ibuprofen only.
The review discussed how a split mouth study would not be possible to explore this topic as analgesia is delivered systemically. However, for a future study in this area, patients who need multiple treatments over a number of appointments could be recruited – therefore a cross-over study design could be employed eg where the patients have one crown fitted with preoperative analgesia administered and another at a separate appointment fitted following administration of a placebo.
If this intervention is proven to be an effective method of reducing postoperative pain, it appears a simple and cost-effective intervention for use in general practice.
The conclusion of the publication is clearly stated; the need for further research with appropriately calculated sample sizes and care to minimise potential bias.
References
Chapman HR, Kirby-Turner N . Visual/verbal analogue scales: examples of brief assessment methods to aid management of child and adult patients in clinical practice. Br Dent J 2002; 193:447–450.
Howard KE, Freeman R . Reliability and validity of a faces version of the Modified Child Dental Anxiety Scale. Int J Paediatr Dent 2007; 17:281–288.
Campbell C, Soldani F, Busuttil-Naudi A, Chadwick B . Update of Non-pharmacological behaviour management guideline: Clinical Guidelines in Paediatric Dentistry, Revised 2011.
Asthma UK . website. Available from https://www.asthma.org.uk/about/media/facts-and-statistics (accessed February 2017).
British National Formulary. Available at www.medicinescomplete.com/mc/bnfc/current/PHP78612-non-steroidal-anti-inflammatory-drugs.htm (Accessed February 2017).
Author information
Authors and Affiliations
Additional information
Address for correspondence: Luisa Fernandez Mauleffinch, Managing Editor, Cochrane Oral Health Group, School of Dentistry, The University of Manchester, JR Moore Building, Oxford Road, Manchester, M13 9PL, UK. E-mail: luisa.fernandez@manchester.ac.uk
Ashley PF, Parekh S, Moles DR, Anand P, MacDonald LC. Preoperative analgesics for additional pain relief in children and adolescents having dental treatment. Cochrane Database Syst Rev 2016; 8: Art. No. CD008392. DOI: 10.1002/14651858.CD008392.pub3.
This paper is based on a Cochrane Review published in the Cochrane Library 2016, issue 8 (see www.thecochranelibrary.com for information). Cochrane Reviews are regularly updated as new evidence emerges and in response to feedback, and the Cochrane Library should be consulted for the most recent version of the review.
Rights and permissions
About this article

Cite this article
McCann, C. Preoperative analgesia for children and adolescents to reduce pain associated with dental treatment. Evid Based Dent 18, 17–18 (2017). https://doi.org/10.1038/sj.ebd.6401220
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6401220
