
Abstract
Data sources
Medline, Embase and CENTRAL databases were searched up to December 2014. Unpublished data were sought by searching a database listing unpublished studies OpenGray [http://www.opengrey.eu/], formerly OpenSIGLE.
Study selection
Randomised clinical trials assessing treatment of patients with AgP comparing scaling and root planing (SRP) alone with SRP plus a single antibiotic or a combination of drugs with a minimum of three months follow-up were considered. Studies specifically designed to evaluate smokers or subjects with diabetes mellitus and HIV/AIDS were not included.
Data extraction and synthesis
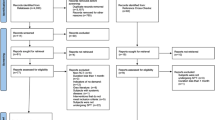
Two researchers independently screened titles, abstracts and full texts of the search results. The studies, which fulfilled inclusion criteria, underwent validity assessment and data extraction using a specifically designed form. The quality of included studies was assessed using the Cochranes collaboration tool for risk of bias. Only two of the 11 included trials were considered at a low risk of bias. The data extracted from ten studies was analysed by pair-wise meta-analyses and the data extracted from five studies was included in Bayesian network meta-analyses pooled estimates. The six studies evaluated in the pairwise meta-analyses were excluded in the pooled estimates because four studies included patients with advanced disease only and one study did not present average data for pocket depth (PD) and clinical attachment level (CAL) and another one for using a different mechanical treatment.
Results
Fourteen studies reporting 11 randomised clinical trials with a total of 388 patients were included in the review. Nine of 11 studies reported a statistically significant greater gain in full mouth mean clinical attachment (CA) and reduction in probing depth (PD) when a systemic antibiotic was used. From those studies the calculated mean difference for CA gained was 1.08 mm (p < 0.0001) and for PD reduction was 1.05 mm (p< 0.00001) for SRP + Metronidazole (Mtz). For SRP + Mtz+ amoxicillin (Amx) group the mean difference was 0.45 mm for CA gained and 0.53 mm for PD reduction (p<0.00001) than SRP alone/placebo. Bayesian network meta-analysis showed some additional benefits in CA gain and PD reduction when SRP was associated with systemic antibiotics.
Conclusions
The results support a statistically significant benefit of adjunctive systemic antibiotics in the treatment of AgP. The most consistent advantages - reduction in PD and CAL gain - were attained with the use of Mtz and Mtz + Amx. Future RCTs should be designed in order to directly compare these two antibiotic protocols in the treatment of AgP.
Similar content being viewed by others


Commentary
A comprehensive literature search was systematically performed for published and unpublished literature. Moreover, references listed in previous systematic reviews and included studies were examined by hand searching in an attempt to identify any further articles that could be considered for inclusion, although there was no indication on the use of non-English resources.
The quality of nine out of the 11 included studies was considered unclear or high risk of bias, questioning the accuracy of the results.
Of the included studies six reported smokers and four included three different chlorhexidine regimens. The results of two studies that performed full mouth ultrasonic debridement instead of SRP were combined and included in the meta-analysis. Of the seven studies that used the combination Mtz + Amx, four had the same regimen. Four out of the five studies included in the meta-analysis for Mtz-Amx and SRP used the same intervention.
According to the authors, the results of both the pair-wise meta-analyses and the Bayesian network pooled estimates support a statistically significant benefit of adjunctive systemic antibiotics in the treatment of AgP. The most consistent advantages, being reduction in PD and CAL gain, were attained with the use of Mtz and Mtz + Amx. Curiously the authors' conclusions on the performance of Mtz alone come from two small RCTs (n=27) using two different regimens.
It is worthwhile to note that the statistical technique, Bayesian network estimates used in the analyses were sophisticated and innovative in the field of dentistry. The Bayesian technique is generally more robust to outliers and allows pooling of all existing information to compare all systemic antibiotic protocols for the treatment of AgP, with an increased degree of precision.
Considering the limitations present in the included studies, it is not clear if the complex data analysis is of clinical relevance.
The findings of the current meta-analysis are in agreement with previous systematic reviews on periodontal improvement values, however; there is no report on side effects or the growing concern of antibiotic resistance.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Leandro Chambrone, Department of Periodontics, College of Dentistry, The University of Iowa, 801 Newton Road, 52242-1001 Iowa City, IA, USA. E-mail: leandro_chambrone@hotmail.com or leandro-chambrone@uiowa.edu
Rabelo CC, Feres M, Gonçalves C, Figueiredo LC, Faveri M, Tu YK, Chambrone L. Systemic antibiotics in the treatment of aggressive periodontitis. A systematic review and a Bayesian Network meta-analysis. J Clin Periodontol. 2015; 42: 647–657. doi: 10.1111/jcpe.12427. [Epub ahead of print]
Rights and permissions
About this article

Cite this article
Rajendra, A., Spivakovsky, S. Antibiotics in aggressive periodontitis, is there a clinical benefit?. Evid Based Dent 17, 100 (2016). https://doi.org/10.1038/sj.ebd.6401197
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6401197
