
Abstract
Scope and purpose
The systematic review was commissioned by the Australian National Health and Medical Research Council (NHMRC) to evaluate the scientific literature relating to the health effects of fluoride and fluoridation. The systematic review's research questions relate to the caries-reducing benefits and associated potential health risks of providing fluoride systemically (via addition to water, milk and salt) and the use of topical fluoride agents, such as toothpaste, gel, varnish and mouthrinse. Although the review summarises the recent evidence, it does not constitute health policy or clinical practice recommendations.
Data sources
A literature search was undertaken using the Medline and Embase databases (via www.embase.com). In addition, the Cochrane Systematic Review and Clinical Trial databases were searched to help identify additional systematic reviews and original studies. Because of the availability of recent systematic reviews, searches were limited to publications from 1996 onwards . The search was conducted in December 2006 and limited to English-language publications.
Study selection
Based on types of intervention (individual or population) and the outcomes assessed (efficacy or safety), the hierarchy of study types considered most relevant for answering each of the clinical questions defined in this review was chosen (Table 1). The levels of evidence used by NHMRC for intervention and aetiological studies are summarised in Table 2.
Data extraction and synthesis
Screening of eligible studies was conducted by three reviewers. Data were extracted for all of the included systematic reviews and individual studies using standardised data-extraction forms. This included information about the study design, NHMRC level of evidence, population, intervention, comparator, outcome definitions and results. Information relating to potential biases and study quality were also extracted. Where appropriate, study results were pooled using standard meta-analysis techniques.
Results
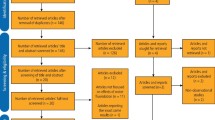
In total, 5418 nonduplicate citations were identified. After applying the inclusion and exclusion criteria, 408 citations were considered potentially eligible for inclusion in the review. After the review of the full papers of potentially eligible articles, 77 citations were included in the review. The summary of findings was presented in the context of the research questions (Table 3).
Recommendations
Fluoridation of drinking water remains the most effective and socially equitable means of achieving community-wide exposure to the caries prevention effects of fluoride. It is recommended (see also www.nhmrc.gov.au/news/media/rel07/_files/fluoride_flyer.pdf) that water be fluoridated in the target range of 0.6–1.1 mg/l, depending on the climate, to balance reduction of dental caries and occurrence of dental fluorosis.n particular with reference to care in hospital for those following stroke.
Similar content being viewed by others

Main
This systematic review of fluoridation is the fourth of the reviews commissioned by the NHMRC in Australia. The first two were carried out in 19854 and 19915 and focussed on the effectiveness of water fluoridation. The third one6 included a review of fluoride intake from discretionary fluoride supplements in addition to water fluoridation. The third review was published in 1999, and is presently available on the website of Australian Dental Association (www.ada.org.au/app_cmslib/media/lib/0703/m50958_v1_nhmrc%20fluoride.pdf). The fourth review7 published in 2007 has once again expanded its scope by including other methods of fluoride delivery, such as milk, salt, toothpaste, gel, varnish and mouthrinse. Fluoride supplements such as drops, chewable tablets and chewing gum tablets have not been explicitly included in the current review, however.
The aim of the most recent review was to synthesise the highest level of evidence to answer each clinical question. It should be noted that the levels of evidence accepted for fluoride intervention at the population level was based on those chosen for the systematic review of water fluoridation by McDonagh et al.2
The inclusion and exclusion criteria for the current review were explicit. The search strategy used to identify relevant studies could not be considered to be comprehensive as no controlled vocabulary was used in searching the electronic databases. Moreover, the range of electronic databases searched was rather limited and restricting studies to those published in the English language may also affect the findings. During the literature search, three reviewers assessed the eligibility of abstracts (approximately one third each). It is not clear whether study selection or data extraction was carried out independently or in duplicate.
Included studies were clearly laid out in table format in the appendix. This included information about the study design, population, intervention, comparator, outcomes and results. The quality of studies was assessed using the key questions from the NHMRC.7 For those study designs such as cross-sectional studies and ecological studies which had no guidance on assessment from the NHMRC, a summary of various factors relating to potential biases was provided. In addition, a global quality rating was given to each individual study. Post-hoc statistical analysis was carried out when necessary.
Two systematic reviews2, 8 and one additional, relevant, original study9 were identified in the literature search on water fluoridation and dental caries. The York review2 was chosen to form the evidence base for the effect of water fluoridation on dental caries in the current review, as it provided more detailed and comprehensive results than those shown in the review by Truman et al.6 It should be noted that 12 of the 21 studies included in the latter were among the 26 studies included in the York review.2 The lack of overlap between the two reviews is largely because the Truman review8 assessed both “fluoridation vs no fluoridation” and “fluoridation vs fluoridation at a lower level” whereas the York review5 assessed only “fluoridation vs no fluoridation”. Only one additional original study9 was identified in the current review and this did not change the conclusion from that of the York one.2 It should be noted that the benefits from fluoridated public water supply were weakened because beverages and food products processed in fluoridated communities were exported to surrounding non-fluoridated communities.10 This phenomenon is referred to as the halo effect: Griffin et al.11 attempted to quantify it by analysing data from the 1986–1987 National Survey of Oral Health in US School Children. Studies measuring the effectiveness of water fluoridation that consider only its direct benefit may have underestimated the total contribution of water fluoridation to caries reduction.
Regarding water fluoridation and dental fluorosis, the literature search identified two systematic reviews2, 12 and 10 additional original studies. It should be noted that in some cases there was a substantial difference in the prevalence of “any fluorosis,” both between different countries and within different countries. These differences result from a number of factors including methods (eg, different fluorosis indices), environmental influences (eg, phosphate mines) and lifestyles (eg, higher tea consumption). The authors concluded that although there was a fourfold risk of developing fluorosis of aesthetic concern with optimal water fluoridation compared with suboptimal water fluoridation, the absolute increase in prevalence was small (approx. 4–5%).
The studies cited in the report of the National Research Council13 have raised the possibility that infants could receive a greater than optimal amount of fluoride through liquid concentrate or powdered baby formula that has been mixed with water containing fluoride during a time when their developing teeth may be susceptible to dental fluorosis. Recently, a systematic review to investigate the association of fluorosis and infant formula has been completed.14 It concluded that the evidence suggests dental fluorosis might be caused by fluoride content in infant formula or the fluoride levels in the water used to reconstitute infant formula. Confounding factors could not be ruled out, however, and publication bias may also distort the evidence on infant formula and fluorosis.
Although the current review presents a summary of the relevant evidence, the potential effectiveness of any public health intervention must be considered in the context of practicalities associated with implementing the intervention, issues surrounding compliance, and issues related to equity of access.
References
National Health and Medical Research Council. How to Use the Evidence: Assessment and Application of Scientific Evidence. Canberra: National Health and Medical Research Council; 2000.
McDonagh M, Whiting P, Bradley M, et al. A systematic review of public water fluoridation. York: University of York National Health Service Centre for Reviews and Dissemination; 2000.
Bassin EB, Wypij D, Davis RB, Mittleman MA . Age-specific fluoride exposure in drinking water and osteosarcoma (United States). Cancer Causes Control 2006; 17:421–428.
National Health and Medical Research Council. Review of the Safety and Effectiveness of Water Fluoridation. Canberra: National Health and Medical Research Council; 1985.
National Health and Medical Research Council. The Effectiveness of Water Fluoridation. Canberra: National Health and Medical Research Council; 1991.
National Health and Medical Research Council. Review of Water Fluoridation and Fluoride Intake from Discretionary Fluoride Supplements. Melbourne: National Health and Medical Research Council; 1999.
National Health and Medical Research Council. NHMRC Public Statement: the Efficacy and Safety of Fluoridation. Canberra: National Health and Medical Research Council; 2007.
Truman BI, Gooch BF, Sulemana I, et al. Reviews of evidence on interventions to prevent dental caries, oral and pharyngeal cancers, and sports-related craniofacial injuries. Am J Preventive Med 2002; 23(suppl. 1):S21–S54.
Seppä L, Kärkkäinen S, Hausen H . Caries trends 1992-1998 in two low-fluoride Finnish towns formerly with and without fluoridation. Caries Res 2000; 34:462–468.
Ripa LW . A half-century of community water fluoridation in the United States: review and commentary. J Public Health Dent 1993; 53:17–44.
Griffin SO, Gooch BF, Lockwood SA, Tomar SL . Quantifying the diffused benefit from water fluoridation in the United States. Community Dent Oral Epidemiol 2001; 29:120–129.
Khan A, Moola MH, Cleaton-Jones P . Global trends in dental fluorosis from 1980 to 2000: a systematic review. South African Dent J 2005; 60:418–421.
Committee on Fluoride in Drinking Water, National Research Council. Fluoride in Drinking Water: a Scientific Review of EPA's standards. Washington: National Academies Press; 2006.
Zina LG, Hujoel P, Moimaz SAS, Cunha-Cruz J . Infant formula and fluorosis: a systematic review (abstract). J Dent Res 2008; 87(special issue): no.1144.
Author information
Authors and Affiliations
Corresponding author
Additional information
Australian National Health and Medical Research Council. Canberra: Australian Government; 2007
Rights and permissions
About this article
Cite this article
Yeung, C. A systematic review of the efficacy and safety of fluoridation. Evid Based Dent 9, 39–43 (2008). https://doi.org/10.1038/sj.ebd.6400578
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6400578
This article is cited by
-
Distribution and health risk assessment of natural fluoride of drinking groundwater resources of Isfahan, Iran, using GIS
Environmental Monitoring and Assessment (2018)
-
Dental caries prevention in children and adolescents: a systematic quality assessment of clinical practice guidelines
Clinical Oral Investigations (2018)
-
Fluoridation and attention deficit hyperactivity disorder – a critique of Malin and Till (2015)
British Dental Journal (2017)
-
A qualitative study of the factors that influence mothers when choosing drinks for their young children
BMC Research Notes (2014)
-
Effects of sodium fluoride treatment in vitro on cell proliferation, apoptosis and caspase-3 and caspase-9 mRNA expression by neonatal rat osteoblasts
Archives of Toxicology (2009)
