
Key Points
-
Peer reviewed publications demonstrate the low erosive properties of a blackcurrant/calcium drink. Further development of this beverage, by incorporation of xanthan gum, allows the beverage to increase in acidity to optimise variables such as consumer acceptance and stability, whilst retaining its low erosive potential to enamel.
-
The drinks tested, a new blackcurrant/calcium/gum drink (test product), and the original blackcurrant/calcium drink were both shown to be significantly less erosive to enamel than a conventional juice drink.
-
These low erosive beverages may be a valuable alternative to other acidic soft drinks for those individuals susceptible to erosion.
Abstract
Objective: To compare the erosive effect of a new blackcurrant/calcium drink with xanthan gum, on enamel in situ, with a low erosive product, a conventional fruit beverage and water.
Design: The study was single centre, randomised, single blind, 4 treatment crossover design.
Setting: This study, conducted in 2000, employed volunteers working at the Bristol Dental Hospital, UK.
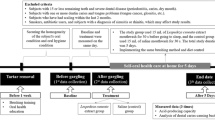
Subjects, materials and methods: 16 subjects (≥18 years) wore two enamel samples in a removable acrylic appliance. The drinks tested were (A) New blackcurrant/calcium/gum drink (test product), (B) Original blackcurrant/calcium drink, (C) Conventional blackcurrant drink (positive control) and (D) Water (negative control), for 15 day study periods. Drinking was supervised, with 250 ml imbibed four times/day between 9.00am–5.00pm. Profile measurements of specimens were made at baseline, 5, 10 and 15 days.
Main outcome measures: Paired t-tests compared erosion by surfometry with selected pairs of formulations.
Results: Of 16 screened subjects (3 male, 13 female), mean age 34.2 years, 1 subject failed to complete the study. A caused significantly less enamel loss than C, with no statistically significant differences from B at any time points measured. Of 43 treatment emergent adverse events, none were considered related to the study formulations.
Conclusions: A retained low erosive properties similar to B, with additional benefits of taste flexibility and beverage stability.
Similar content being viewed by others

Main
A number of peer reviewed epidemiological studies in the dental literature1,2,3,4,5 highlight the presence of erosion in our population, particularly in the younger generations. However, as yet no longitudinal data are available to support these clinical observations. A recent paper corroborated these findings, showing that approximately half of 14-year-olds have appreciable tooth wear and significant erosion.6 Interestingly, this was found to be more prevalent in lower socio-economic groups.6 Retail sales of soft drinks indicate a rise in consumption of 2–3% each year from 1986 to date and future projections suggest this trend will continue.7 The volume of soft drinks imbibed does correlate to some degree with the level of erosion observed.8 However, controlled studies have shown that susceptibility to erosion under similar exposure varies considerably.9,12,13,14 Other factors, mainly physical, including abrasion and erosion, will also modify the level of toothwear that occurs although the interaction of chemical and physical wear processes have received limited attention using in vitro methods and none in vivo. For those individuals who are susceptible to erosion, tooth loss can be rapid. Ideally, and hopefully in the not too distant future, such susceptible individuals will be identifiable before excessive hard tissue loss occurs and allow for the provision of appropriate dietary advice or medical intervention. In the meantime the development of low erosive beverages, that appeal to our organoleptic senses, will undoubtedly be extremely useful for these vulnerable people.
A series of published in vitro and in situ studies12,13,14 have demonstrated the ability to create an extremely low erosive beverage to enamel in situ by product modification with respect to raising the pH, lowering the titratable acidity and addition of calcium. Whilst these modifications have resulted in a product with very low erosive properties, other characteristics such as consumer acceptability and stability of the ingredients could be enhanced. However, to optimise these properties by raising titratable acidity and lowering pH, would counteract the positive ability to reduce enamel erosion. Fortuitously, a method was conceived of attaining both goals by incorporating a small amount of polysaccharide food grade gum in the formulation. In vitro investigations gave reason to suggest clinical trials would be promising.15 The advantages of gum addition without adversely influencing the low erosive potential is worthy of further clinical trials for validation.
The objective of this study was to compare the erosive effect on tooth enamel of a blackcurrant/calcium drink with gum with the marketed low erosive product (Ribena ToothKind™ — SmithKline Beecham, Coleford, UK), a conventional fruit beverage with no added sugar established as acting as a positive control, and water as a negative control, after a 15 day treatment period using an in situ method.9 A secondary objective was to determine the loss of enamel, measured by surfometry after 5 and 10 days from the four beverages in the study.
Method and materials
Ethical approval for the study was granted by the United Bristol Healthcare NHS Trust Ethics Committee and the study was conducted according to the guidelines for Good Clinical Practice.10 All volunteers received verbal and written information concerning the study and gave signed and witnessed consent to participate. A clinical research associate from the sponsor company monitored the conduct of the study in accordance with good clinical practice. The study was a single centre, randomised, single blind, four treatment crossover design balanced for first order carryover effects of treatment involving 16 healthy volunteers. Inclusion and exclusion criteria for acceptance in the study were exactly as described in previous publications.12,13,14 Oral soft tissue and dental examinations were performed at baseline and end of study. A sample size of 16 subjects was chosen based on experience from previous similar studies.
The drink formulations used in this study were concentrates and are listed below with details of the formulations and manufacturer shown in the data sheet (Table 1):
A – New blackcurrant/calcium/gum drink (test product)
B – Original blackcurrant/calcium drink (Ribena ToothKind™)
C – Conventional blackcurrant drink (Robinson's Special R™ No Sugar Added Apple and Blackcurrant Juice Drink) (positive control)
D – Water (negative control)
Volvic water was used as the negative control.11
As with previous studies12,13,14, the appliances carrying the enamel samples were worn 9.00am to 5.00pm (±30 minutes) with 250 ml volumes of the respective drink imbibed at 0900, 1100, 1300 and 1500 hours. Drinks were sipped under supervision, 25 ml per minute for 10 minutes. Subjects were randomised to receive each of the four study treatments during the four 15 day study periods, over a 12 week period according to a computer generated randomisation schedule supplied as a four-way Latin square design balanced for first-order carry over effects. Appliances were only removed for 1 hour to coincide with the lunch break. Whilst appliances were in place no food or drink except water and the test drink were to be consumed.
Enamel specimens, from human unerupted third molar teeth, were prepared for measurement by surfometry as previously described.9 Specimens employed in the investigation were polished flat to have profile tolerances of ±0.1 μm at baseline readings. As before, specimens were taped to expose a window of enamel approximately 2 mm wide. Volunteers were asked to wear an upper acrylic appliance, retained by Adams cribbs to the first upper molar teeth. One enamel sample was placed in the anterior mid-hard palate and another in the posterior mid-hard palatal position of the appliance. Samples were removed from the appliances at the end of day 5, 10 and 15 for duplicate measurements on a surfometer for both anterior and posterior samples. This recorded the mean depth of the eroded sample and the mean was taken. Fresh enamel samples were placed in the intra-oral appliance at the beginning of each new drink study period. Storage of specimens and appliances overnight were as before.12,13,14 Additional specimen disinfection was performed after profilometry (days 5, 10, 15) when specimens were placed in a solution of 0.5% chlorhexidine in 70% spirit for 30 minutes. If a preset safety limit of 20 μm enamel loss was recorded in any phase of the trial, the volunteer was withdrawn from that period.
Subjects were asked to use a standard toothpaste (Aquafresh™ 'Mild 'N' Minty' — SmithKline Beecham, Brentford, UK) as well as a standard toothbrush (Aquafresh Flex™ — SmithKline Beecham, Brentford, UK) twice daily throughout the trial. No mouthrinses were allowed. Subjects were asked not to take any acidic medication (pH < 5.3) during the study. Any adverse events were to be reported to an investigator at any time during each study period or questioned by the investigator at the end of each study period.
Statistical methods
Data for erosion for each subject with each drink were derived from the specimen measured by profilometry on baseline and days 5, 10 and 15. Gross heterogeneity of variation between erosive and non-erosive formulations was expected.13,15 Accordingly, the primary analysis consisted of paired t-tests comparing pre-specified pairs of formulations, together with corresponding confidence intervals for mean differences of enamel loss determined by surfometry at 15 days. Six pairwise contrasts between formulations were compared, that is, A versus B; A versus C; A versus D; C versus B; C versus D; D versus B. Analyses similar to the primary analysis, were performed for the secondary analysis for enamel loss measured by surfometry at 5 and 10 days. Although no formal adjustment for multiple testing was made, the primary parameter and comparisons of interest were pre-specified and the p-values for the secondary analysis were interpreted cautiously.
Results
Sixteen subjects were screened and randomised. One subject did not attend the last study period for dosing or assessments. Another subject consumed a mixture of products in period 2 and so the data from this period is analysed using all available data. Of the randomised subjects, 3 (18.75%) were male and 13 (81.25%) were female. The mean age was 34.2 years (SD = 12.3 years).
The results for the primary efficacy variables are tabulated in Table 2 together with P values. Mean differences between treatments for enamel loss at day 15 are presented with the corresponding confidence intervals. Mean enamel loss is shown diagrammatically in Figure 1. Tables 3 and 4 present secondary efficacy variables with mean differences (mm) between treatments for 5 and 10 days respectively, together with P values. For Tables 2,3 and 4 the reference formulation is the first formulation in each comparison so that a positive difference indicates more erosion with the second formulation.

Mean enamel loss in microns (error bars represent one standard deviation).
New blackcurrant/calcium/gum drink (A) caused significantly less enamel loss than the conventional blackcurrant drink (C). The differences in enamel loss between the beverages were found to be highly statistically significant at all time points measured (days 5,10 and 15). Similarly, original blackcurrant/calcium drink (B) caused significantly less enamel loss than C. Indeed, at day 15, C caused between 4.60 and 4.73 microns more erosion than the other three products. No statistically significant differences in enamel loss were found between A and B at any of the time points measured.
Statistically significant differences were found between A and D; and B and D. The mean differences between the comparators was 0.24 and 0.43 microns respectively at day 15, and these values were many times less than those seen between C and D.
For the sixteen randomised subjects, 43 adverse events were experienced (from 14 volunteers) possibly related to the treatment. Thirty-three adverse events were rated as mild, nine as moderate and one as severe as documented in the Good Clinical Practice Guidelines.10 There were no serious adverse events and all events were considered not related to the study formulations.
Discussion
One of the effects due to the growth of the food and drink industry, is the huge increase in the consumption of soft drinks and fruit juices. Many of these beverages are acidic in nature owing to their high juice content. Following the Chief Dental Officer's challenge in 1993 to reduce the erosive potential of products, a low erosive beverage was marketed in 1998. This low erosive formulation was achieved predominantly by innovative permutations of pH, titratable acidity and calcium content ratios.12,13,14 Whilst this formulation attained merit for low erosive properties, stability and consumer acceptance regarding taste could be enhanced. As a result of a chance observation and subsequent laboratory studies (unpublished), it was conceivable that these properties could be optimised with the addition of a gum such as xanthan, which is already used in some acidic soft drink products.
A clinical trial16 comparing orange juice as positive control, original blackcurrant/calcium drink, water as negative control and a blackcurrant/calcium/gum drink demonstrated significant (P < 0.05) reduction in erosion by the two blackcurrant/calcium drinks compared with the orange juice, with no significant differences from water at day 10. However, the original blackcurrant/ calcium drink produced significantly less erosion than the gum modified drink. Hence, the blackcurrant/calcium/gum drink underwent minor reformulation to provide the test product (A) evaluated in the study documented in this paper.
In the present study the new blackcurrant/calcium/gum drink was less erosive at all time points than original blackcurrant/calcium drink, although these differences did not reach statistical significance. This is an important finding, since if these beverages are to be fully used for susceptible individuals, they need to be equally acceptable to consumers as other propriety products, particularly in respect of taste.
This study also performed a valuable exercise for validation purposes. Both of the blackcurrant/calcium drinks showed minimal erosion to enamel compared with the conventional fruit drink.
Comparing erosion of enamel by the blackcurrant/calcium drinks, A and B, to water D, demonstrated the former products were significantly more erosive to enamel. However, the mean difference in microns between A and D at day 15 was only 0.24 microns and between B and D 0.43 microns, a factor of 120 less than between C and D, 4.67 microns. Previous trials12,13,14 have been performed comparing the erosive effect on enamel of blackcurrant/calcium drink compared with water. These studies indicated that there were only small differences, and in some instances no statistically significant differences were found between modified juice formulations and water during a 15 day treatment period. In the study documented, baseline tolerance was ±0.1 microns, but in previous studies it was ±0.3 microns. If we had retained the higher tolerance level in this study, it is arguable that we would not have reached significance and this should be borne in mind when interpreting the results. Slight differences between studies may also reflect biological variation in specimens. Subsurface softening of the enamel was not assessed in this study. It is also worthy of comment that these studies portray the worst case scenario for enamel erosion. However, statistical significance must be balanced against the more important factor of clinical relevance. The modified blackcurrant/calcium beverages have superior clinical low erosive properties to the conventional product tested. Further, comparisons of the blackcurrant/calcium and blackcurrant/calcium/gum drinks determined that the latter was both consumer-preferred and supported a longer shelf life (data not shown).
In conclusion, modification to the blackcurrant/calcium drink as a result of addition of a gum such as xanthan has facilitated benefits to the beverage in terms of beverage stability and taste qualities, without detrimentally influencing clinical enamel erosion.
References
The Office of Population Censuses and Surveys (OPCS) (1994). Dental caries among children in the United Kingdom in 1993. Office of Population Censuses and Surveys, publication number SS94/1.
Lussi A, Schaffner M, Hotz P et al. Dental erosion in a population of Swiss adults. Community Dent Oral Epidemiol 1991; 19: 286–290.
Milosevic A, Lennon MA, Fear SC . Risk factors associated with tooth wear in teenagers: a case control study. Community Dent Health 1997; 14: 143–147.
Millward A, Shaw, Smith AJ et al. The distribution and severity of tooth wear and the relationship between erosion and dietary constituents in a group of children. Int J Paediatr Dent 1994; 4: 152–157.
Bartlett DW, Coward PY, Nikkah C et al. The prevalence of tooth wear in a cluster sample of adolescent schoolchildren and its relationship with potential explanatory factors. Br Dent J 1998; 184: 125–129.
Al-Dlaigan YH, Shaw L, Smith A . Dental erosion in a group of British 14-year-old, school children. Part 1:Prevalence and influence of differing socio-economic backgrounds. Br Dent J 2001; 190: 145–149.
The 1997 Sucralose Drinks Report. Tate & Lyle Speciality Sweeteners, Whiteknights, Reading RG6 6BX.
Al-Dlaigan YH, Shaw L, Smith A . Dental erosion in a group of British 14-year-old, school children. Part 2: Influence of dietary intake. Br Dent J 2001; 190: 258–261.
West NX, Maxwell A, Hughes JA, Parker DM, Newcombe RG, Addy M . A method to measure clinical erosion: The effect of orange juice consumption on erosion of enamel. J Dent 1998; 26: 329–336.
Good Clinical Practice Tripartite Guideline for Good Clinical Practice. The Institute of Clinical Research, PO Box 1208, Maidenhead, Berkshire SL6 3GD UK.
Curzon MEJ, Hefferen JJ . Modern methods of assessing the cariogenic and erosive potential of foods. Br Dent J 2001; 191: 41–46.
Hughes JA, West NX, Parker DM, Newcombe RG, Addy M . Development and evaluation of a low erosive blackcurrant juice drink in vitro and in situ 1. Comparison with orange juice. J Dent 1999; 27: 285–289.
Hughes JA, West NX, Parker DM, Newcombe RG, Addy M . Development and evaluation of a low erosive blackcurrant juice drink 3. Final drink and concentrate, formulae comparisons in situ and overview of the concept. J Dent 1999; 27: 345–350.
West NX, Hughes JA, Parker DM, Newcombe RG, Addy M . Development and evaluation of a low erosive blackcurrant juice drink 2. Comparison with a conventional blackcurrant juice drink and orange juice. J Dent 1999; 27: 341–344.
Baker NJ, Parker DM . International Patent Publication WO 00/13531
Hughes JA, Jandt JK, Parker D, Newcombe RG, Eisenburger M, Addy M . Further modification to soft drinks to minimise erosion: a study in situ. Submitted Caries Research 2001.
Acknowledgements
This trial was supported by a grant from SmithKline Beecham, St George's Avenue, Weybridge, Surrey KT13 0DE, UK.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article
Cite this article
West, N., Hughes, J., Parker, D. et al. Modification of soft drinks with xanthan gum to minimise erosion: a study in situ. Br Dent J 196, 478–481 (2004). https://doi.org/10.1038/sj.bdj.4811186
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4811186
This article is cited by
-
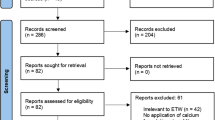
The role of calcium in the prevention of erosive tooth wear: a systematic review and meta-analysis
Evidence-Based Dentistry (2024)
-
In situ effect of enamel salivary exposure time and type of intraoral appliance before an erosive challenge
Clinical Oral Investigations (2017)
-
In vitro evaluation of the erosive potential of viscosity-modified soft acidic drinks on enamel
Clinical Oral Investigations (2014)
