
Key Points
In this part, we will discuss:
-
Why occlusal considerations are different in children
-
How the adult occlusion can be influenced by the treatment of common problems in the child's dentition
Abstract
The difference between paediatric dentistry and most other branches of dentistry is that in the child the occlusion is changing. Consequently 'Good Occlusal Practice' in children is a matter of making the right clinical decisions for the future occlusion. The clinician needs to be able to predict the influence that different treatment options will have on the occlusion when the child's development is complete.
Similar content being viewed by others



Main
Many of the factors governing the developing occlusion have already been covered in the section on orthodontics, but there are specific instances in which the dentist in general practice will be faced with decisions which could have an influence on the occlusion of child patients. This section aims to present these situations and give guidelines, which will help the reader make the most appropriate treatment decision for their individual patients.
Problems and Choices:
Common Problems:
-
Premature loss of a primary tooth
-
'Submerging E'
-
'Firm upper C'
-
Premature loss of first permanent molar
-
Avulsed permanent tooth
-
Fracture of permanent upper incisor
-
Missing permanent teeth
Premature loss of a tooth in the primary dentition:
If a primary tooth is lost prematurely, then consideration of an extra (balancing) extraction will be necessary.1,2 This will be with a view to preventing a shift of the midline or resultant disruption of the developing occlusion.
-
If a primary incisor tooth is lost as a result of caries or trauma this does not usually have an effect on the developing occlusion. Space closure is not going to occur as primary incisor teeth usually become spaced prior to exfoliation.
-
If a primary canine tooth needs to be extracted, then the contralateral primary canine should also be extracted, in many cases, to prevent an untoward midline shift. Only if the anterior dentition is spaced should unilateral loss be accepted.
-
If a single primary molar tooth is unsavable and the other teeth have a good prognosis there is no need to extract other molar teeth.
If primary first and/or primary second molars in three quadrants have to be extracted then the equivilant molar in the fourth quadrant should be extracted in order to keep the development and drift symmetrical in each quadrant.
The 'submerging E'
The sight of a primary second molar that appears to be 'submerging' below the level of the occlusal plane of the adjacent teeth is not uncommon. Submergence is an inaccurate term as it is the adjacent teeth which are erupting normally, whilst the ankylosed primary molar is remaining static (Fig. 1).

A case where the degree of submergence is minor; there is no tilting of the first permanent molar. This requires no treatment because the primary tooth is usually eventually shed, as long as the permanent sucessor is present
The significance of the 'submerging E' lies not just with the loss of occlusal contact with the opposing teeth, but also the loss of contact, interdentally, with the adjacent teeth, especially distally with the first permanent molar.3 Figure 2 shows that the first permanent molar has tilted mesially, because of the loss of an effective stabilising contact with the second primary molar.

The submergence of the primary molar is more severe than that in Figure 1. As a consequence the primary second molar has lost contact against the adjacent first permanent molar, which has tilted mesially
The issues, therefore, are:
Is there an effective contact with the opposing teeth and has the first permanent molar started to tilt mesially?
If the 'submerging primary tooth is disrupting the occlusion and there is a permanent successor then the ankylosed primary molar must be extracted to facilitate the eruption of the permanent tooth. There is an argument that this tooth should be extracted even if there is no permanent successor, because the 'submerged E' is not adding to the occlusion and the tilting of the first permanent molar is still an unwanted side effect.
'Firm upper C'
The permanent canine is an essential tooth to consider in the developing occlusion. In an 'ideal' adult occlusion this tooth provides the anterior guidance during an excursive movement of the mandible.
At 9.5 years of age an assessment must be made for the position of the permanent canines.
This is initially done by palpating for the buccal canine bulge.4 When canines are not palpable the assessment must now include radiographs, for example parallax periapical views. If the canines are veering off from the normal path of eruption the primary canines should be extracted in order to encourage their permanent successors to erupt in the correct position. The eruption of the permanent canines should be reassessed radiographically after 6 months. If their position is not improving referral to a specialist orthodontist is advised.
At ages 9.5 to 10.5 continuing assessment must be made for the canine position. If one primary canine is mobile but the other is firm and the permanent canine is palpable under the mucosa the firm primary canine should be extracted to allow eruption of the successor.
At ages 10.5 onwards if a primary canine is still firm and the permanent canine is not palpable under the mucosa the appropriate treatment will depend upon the position of the unerupted canine. Specialist orthodontic opinion should be sought so that an early decision can be taken as to whether:
-
To encourage eruption of the permanent successor
-
To leave the permanent canine unerupted
-
To arrange surgical removal of the unerupted permanent canine
These are treatments that will, almost certainly, require specialist opinion and action; the important element is timing and it is only the patient's regular dentist who can ensure a timely referral is made by meticulous monitoring.
Premature loss of a first permanent molar
'Restoration at all costs' may not always be the best option
The literature is replete with data on how to, whether to, or whether not to restore carious first permanent molars, and the debate is still active. The authors consider that a clinician should think carefully before filling and especially before refilling a first permanent molar tooth in a child who is less than 10 years of age.5
'Restoration at all costs' may not always be the best option. Early extraction of first permanent molars with a poor long-term prognosis may be the best treatment option and must be considered at the outset. The essential question that general dental practitioners need to ask themselves at this time is whether the patient may require orthodontic treatment or will the affected tooth need a crown in the future? If either is likely, then consideration should be given to extraction of the decayed/hypoplastic tooth and also the other first permanent molars. With the welcome arrival of a more restorative treatment expectation in the minds of both the profession and general public, there is a real danger that some dentists may be tempted into restoring severely carious or hypoplastic first permanent molars in their young patients without considering how these teeth fit into the long-term treatment plan. Patients will almost certainly wish to avoid extraction, and whilst supporting this as a general principle, it may fall to the dentist to explain sensitively that this is an instance when extraction is preferable. To compound the problem, if there is a strong indication that if one or two first permanent molars need to be extracted, then extraction of the others must also be considered.
It is our aim to give some guidelines to the treatment planning of these cases. As always the treatment planning starts with an examination.
Examination procedures
Radiographic examination
-
Extent of caries
-
Danger of pulpal involvement
-
Sign of caries on smooth surfaces
-
Likelihood of refilling or crown
-
-
Presence of all other unerupted permanent teeth, especially second premolars
-
Development of the second permanent molars.
If an assessment reveals that spontaneous space closure is desirable, timing of extractions is crucial. When the bifurcation of the second molars is visible (just formed) on radiographs and the upper lateral incisor teeth have erupted, this is the best time to extract the first molars to ensure maximum spontaneous alignment. This is because if this stage of development has been reached the lower second molars will move bodily mesially during eruption rather than tilt mesially, which is what happens if extraction are left until later.6
-
Hypoplasia of unerupted premolar teeth If the premolar teeth are of poor quality and there is potential crowding then the balance swings towards conservation of the first permanent molars. The decision on which teeth to extract is delayed until the premolars can be assessed upon their eruption.
-
Crowding in the premolar region If the first molars are so carious or hypoplastic as to warrant extraction, then often the second primary molars may well have previously been extracted. This may have allowed the first molars to have drifted mesially resulting in a lack of space for the unerupted second premolar. In this situation, extraction of the permanent first molars is certainly indicated as it removes a tooth with a poor prognosis and also relieves premolar crowding (Fig. 3).
Figure 3 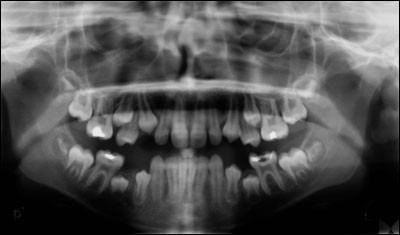
Panoramic radiograph: the lower first permanent molars are carious and there is premolar crowding

Factors influencing decision to extract
-
Number of other carious teeth
-
Extent of caries (extract if there is pulpal involvement)
-
Oral heath status
-
Motivation towards dental health
-
Presence of malocclusion
-
Motivation towards orthodontic treatment
Trauma in the permanent dentition
The general dental practitioner frequently encounters a patient presenting with a fractured or avulsed upper incisor tooth. The management of the clinical condition of the fractured, or avulsed, tooth is the subject of many publications and the practical and definitive treatment plan can be sought elsewhere. What we aim to address in this section is the effect of the treatment plan upon the occlusion.
Avulsed tooth
-
If the avulsed upper tooth is successfully replanted
There is likely to be no lasting effect upon the developing occlusion, except that effects of the orthodontic treatment on this tooth are likely to be unpredictable, in respect of root resorption.
-
If the avulsed upper incisor tooth is not replanted
A space maintainer should be fitted. The design of this is important from an occlusal point of view. A simple tissue borne spoon denture is not sufficient, because if the prosthetic tooth fractures off from this type of denture then immediately the teeth on either side will start to drift into the space. A more desirable approach is to fit what is in effect an orthodontic appliance with a tooth attached. This design should include clasps on the posterior teeth and stops onthe teeth either side of the gap, at the level of the gingival papillae. If the tooth fractures off this appliance, then the stops will maintain the space until the appliance can be repaired (Fig. 5, 6).
Figure 4a 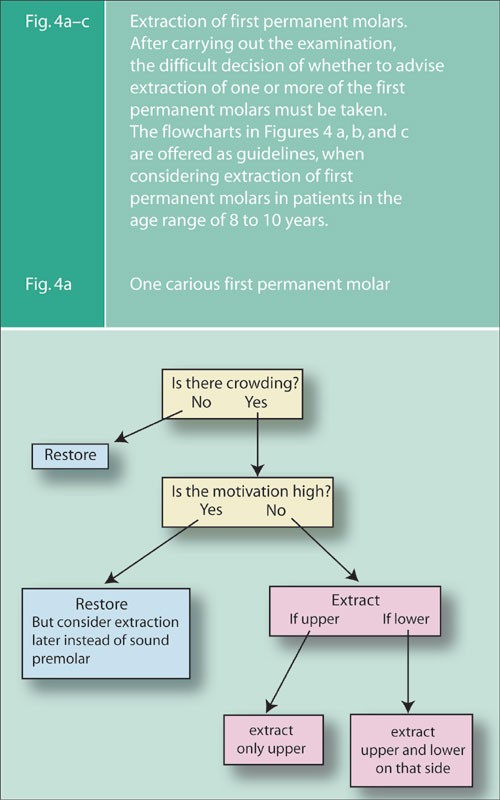
One carious first permanent molar
Figure 4b 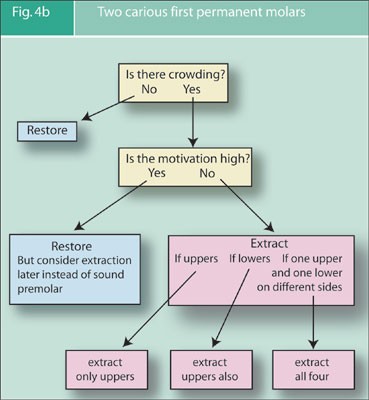
Two carious first permanent molars
Figure 4c 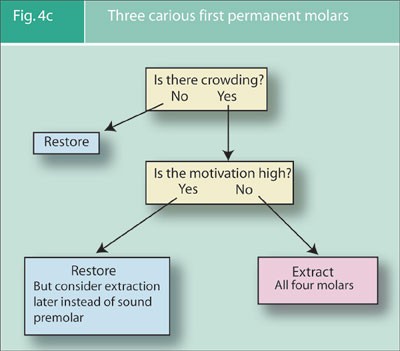
Three carious first permanent molars
Figure 5 
Anterior view of space maintainer showing mesial and distal stops
Figure 6 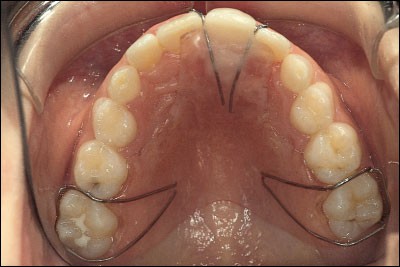
Mirror view of space maintainer





Fracture of permanent upper incisor
-
The most common fracture involves the mesial or distal aspects of the crown. These teeth can be relatively easily and quickly restored by acid etch composite tips so preserving the contact point with the adjacent tooth. The restoration of the contact with the adjacent tooth is very important. In the case illustrated (Fig. 7a, b) the failure to do so has resulted not only in a mesial and labial tilting of the unrestored tooth, but also in a loss of palatal width. As a consequence of this inaction the restoration of this young patient's dentition represents a major orthodontic and restorative challenge.
Figure 7a 
Despite the poor aesthetics and marginal adaptation, the fracture of UR1 (11) has been restored. The lack of restoration of UL1 (21) has allowed mesial and labial tilting
Figure 7b 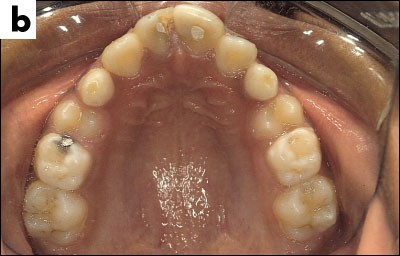
The tilting of UL1 (21) has resulted in narrowing of the space for the crown of the tooth
-
Fortunately a horizontal fracture of the crown of a tooth is less common. It is important that the crown of a tooth so fractured is restored to its original size and shape to prevent occlusal problems developing. The results of this type of injury to the tooth remaining unrestored are over-eruption of the opposing tooth, and less obviously the damaged tooth may tilt buccally because there is reduced lip control.


Missing permanent teeth
In the case of the congenital absence of permanent teeth, the general practitioner's responsibility is early detection. The responsibility, now, for treatment planning lies with the paediatric dentist and specialist orthodontist because with timely referral many of the potential problems of hypodontia can be avoided.

References
Andlaw R J, Rock W P . A manual of paediatric dentistry. 4th edn. Edinburgh: Churchill Livingstone, 1996.
Ball I A . Balancing the extraction of primary teeth: a review. Int J Paed Dent 1993; 4: 176–185.
Shaw W C . Orthodontic and occlusal management. Oxford: Wright, 1993.
British Orthodontic Society. Young practitioners guide to orthodontics. British Orthodontic Society, 1998.
Blinkhorn A S, Mackie I C . Treatment planning for paedodontic patients. London: Quintessence, 1992.
Mackie I C, Blinkhorn A S, Davies P J H . The extraction of permanent first molars during the mixed dentition period — a guide to treatment planning. J Paed Dent 1989; 5: 85–92.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed paper
Rights and permissions
About this article
Cite this article
Davies, S., Gray, R. & Mackie, I. Good occlusal practice in children's dentistry. Br Dent J 191, 655–659 (2001). https://doi.org/10.1038/sj.bdj.4801261
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4801261
This article is cited by
-
The interdisciplinary management of patients with amelogenesis imperfecta – restorative dentistry
British Dental Journal (2012)
-
Management of dental trauma in primary care: a postal survey of general dental practitioners
British Dental Journal (2005)
