
Abstract
Aim To examine the relationship between the Index of Complexity, Outcome and Need (ICON) and the subjective opinions of patients attending for routine dental care.
Materials and methods This study was undertaken at two general dental practices in Cardiff and Bedford. 50 patients aged between 11–14 years and 50 patients aged 30–40 years presenting for routine dental treatment were selected in each. The subjects were assessed objectively using the ICON guidelines by two examiners trained and calibrated in the use of this index. The scores were recorded directly from the patient. Subjective assessments were obtained from the patients by means of a questionnaire consisting of four simple questions addressing aesthetics, function, speech and treatment need using a five point Likert scale.
Results The mean ICON scores for the different genders and age groups participating in this study were; 11–14 year old males 58.4 (SE 3.17); 11–14 year old females 51.8 (SE 3.51); 30–40 year old males 51.2 (SE 2.70); 30–40 year old females 45.3 (SE 2.56). There were statistically significant differences in ICON scores between the younger and older groups (P = 0.024) and females and males (P = 0.04). Adult patients were more likely to reject treatment than younger patients. Analysis of the professional scores in relation to subjective assessments, using the Spearman rank correlation coefficient, for 11–14 and 30–40 year olds, and for the male and female genders, revealed that the ICON has a significant correlation with patients' perceptions of aesthetics, function, speech and treatment need (r2 = 0.01 to 0.28). The only exceptions were patients' perceptions of speech in the 30-40 year old group, and function in the female gender, which did not show a statistically significant correlation to the professional assessments.
Conclusion In this study, the ICON was found to correlate with patients' opinions of aesthetics, function, speech and treatment need. The strength of association, however, was low. It can be concluded that the ICON alone is not necessarily a suitable predictor for appearance, function, speech or treatment need for those individuals attending general dental practice for routine dental care. In combination with a simple question to assess the patients desire for treatment, the shared decision for any particular individual to enter the treatment process can be determined.
Similar content being viewed by others

Main
With the ever-increasing importance of clinical effectiveness and audit, the only way of ensuring the proper undertaking of evidence-based research on a large scale is to standardize methods of measurement. Indices have been used for a long time to standardize methods of measurement, thus facilitating comparisons when conducting epidemiological surveys in populations. Furthermore, they have been used to objectively assess the need for treatment to maximize benefit from limited resources.
The provision of orthodontic care in terms of treatment need and outcome has also been assessed for many years by such indices as the Index of Orthodontic Treatment Need (IOTN)1 and Peer Assessment Rating (PAR),2 respectively. However, the multifactorial nature of malocclusion, which includes the patients' expectations and psychological needs, physical characteristics of occlusion, complexity of treatment3,4 and the degree of improvement aimed for by the orthodontist, makes it difficult to standardize judgements.
In order to overcome such factors, the Index of Complexity, Outcome and Need (ICON) has been developed.5 Based on the expert opinion of 97 practising specialist orthodontists from Germany, Greece, Hungary, Italy, Netherlands, Norway, Spain, UK and USA, this international index provides a single assessment method to record treatment complexity, outcome and need (Appendix 1).
The ICON consists of five components, each having been awarded a different weight according to its relative importance. Component 1 of the ICON has been adopted from the Aesthetic Component (AC) of the IOTN. The other components include upper arch crowding/spacing, crossbite, incisor open bite/overbite, and buccal segment antero-posterior relationship. Each component can be measured on patients or study casts. Furthermore, this index can be a useful tool in audit, research and orthodontic decision-making. The ICON score determines level of need, complexity and degree of improvement as a result of treatment.
The purpose of this study is to determine the relationship between this index and patients' perceptions regarding malocclusion.
Aim
To examine the relationship between ICON and the subjective opinions of patients attending for routine dental care.
Objectives
-
i
To calibrate examiners to an acceptable level of reliability.
-
ii
To determine the subjective opinions of 11–14 and 30–40 year olds with respect to aesthetics, function, speech and treatment need.
-
iii
To highlight the differences in ICON scores between the two age groups, and the two genders.
-
iv
To determine the strength of association between the ICON and patients' subjective opinions.
-
v
To determine the sensitivity and specificity of the ICON with respect to treatment need.
Materials and methods
This study was undertaken at 2 dental practices in Bedford and Cardiff, UK. Fifty patients aged between 11–14 years and 50 patients aged 30–40 years presenting for routine dental treatment were selected in each general practice. An equal ratio of males to females was examined in each age category. Individuals with physical and/or mental impairment, individuals who had previously received orthodontic treatment, individuals who were undergoing orthodontic treatment, and individuals who were presenting for orthodontic treatment were excluded from the study.
The subjects were assessed objectively using the ICON guidelines (Appendix 1) by two examiners trained and calibrated in the use of this index. The scores were recorded directly from the patient. Subjective assessments were obtained from the patients by means of a questionnaire consisting of four simple questions addressing aesthetics, function, speech and treatment need using a five point Likert scale (Table 1).
Statistical analysis
Reliability: Examiner reliability was assessed using the Root Mean Square (RMS) for the ICON. The Root Mean Square is given by the formula:

Where diis the difference between the two raters. The RMS error is an estimate of the standard deviation representing the measurement error of a single measurement.6
Analytical Statistics: Independent samples t-test was used to highlight the differences in mean ICON scores between the two different age groups and genders.
Level of association: The relationship between the ICON and the subjective assessments determined from the patients was analysed using the Spearman rank correlation coefficient. The strength of association was determined using r2.
Sensitivity and specificity: Cross-tabulation analysis was used to determine the ability of the ICON to detect treatment need where it is required, and to reject it where treatment is not needed.
Results
A high level of reliability was achieved with the ICON (RMS < 9; mean difference 1.50 ICON points; limits of agreement: –2.88 to 5.88).
The mean ICON scores for the different genders and age groups participating in this study were as follows (Table 2): 11–14 year old males 58.4 (SE 3.17); 11–14 year old females 51.8 (SE 3.51); 30–40 year old males 51.2 (SE 2.70); 30–40 year old females 45.3 (SE 2.56). There were statistically significant differences in ICON scores between the younger and older groups (P = 0.024) and females and males (P = 0.04).
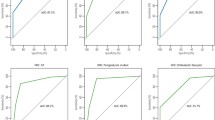
Analysis of the professional scores in relation to subjective assessments, using the Spearman rank correlation coefficient, for 11–14 and 30–40 year olds, and for the male and female genders, revealed that the ICON has a significant correlation with patients' perceptions of aesthetics, function, speech and treatment need (Tables 3, 4). The only exceptions were patients' perceptions of speech in the 30–40 year old group, and function in the female gender which did not show a statistically significant correlation to the professional assessments.
Finally, cross-tabulation analysis of the ICON scores in relation to subjective assessments regarding treatment need revealed that 8% of males and 13% of females who did not need treatment, and 35% of males and 38% of females who needed treatment, answered 'yes' to question 4 ('If you were offered treatment now to straighten your teeth would you accept it'). Twenty-four per cent of males and 29% of females who did not need treatment, and 33% of males and 20% of females, who needed treatment, answered 'no' to question 4 (Table 5, Table 6). With regard to the cut-off point on treatment need (> 43 ICON points) for young female adults 5 out of 20; young males 3 out of 17; adult females 8 out of 15 and adult males 13 out of 18 cases did not want treatment. Therefore, there is a clear distinction, adults generally preferring not to have orthodontic treatment. In terms of difficulty: 5 young females; 2 young males; 0 adult females and 2 adult males would be classified as very difficult (ICON > 77).
Discussion
This study offered advantages over previous studies comparing professional indices and patients' perceptions of malocclusion in that the subjects participating in this study were presenting for routine dental care with no past or present experience of orthodontic treatment. Consequently, these subjects would not have been sensitized to orthodontic treatment, and therefore, their opinions were a representation of that of the general population. Furthermore, the ICON has been developed as an international index and uniformity exists between the various professionals in identifying and placing importance on the different components of the ICON that represent deviant occlusal traits. This means that factors such as ethnic origin were less likely to influence the results of this study.
As the ICON is a new index, no studies to date have been undertaken to investigate the correlation of patients' subjective perceptions of malocclusion with professional opinions. However, a study comparing the relationship of two professional indices with patients' perceptions of aesthetics, function and speech and treatment need, has shown that the AC of IOTN, also used as component 1 of ICON, to have a statistically significant correlation with the patients' subjective opinions.7 Furthermore, studies in Finland, Norway and the UK have demonstrated that the AC of IOTN, also used as component 1 of the ICON, is a strong indicator for patient satisfaction.8,9,10
Analysis of the mean ICON scores determined by the professional (Table 2) demonstrated that for both genders and age groups the mean score was higher than the pre-treatment need cut-off point of 43 as indicated by the ICON. This can be explained from the viewpoint that the subjects participating in this study had not previously or were not receiving orthodontic treatment, which would tend to lead to higher ICON scores.
The ICON was found to have statistically significant correlations (P < 0.01) with patients' perceptions of aesthetics, function, speech and treatment need. The figures for strength of correlation (r2) between ICON and patients' opinions of aesthetics, function, speech and treatment need ranged from 0.01 to 0.28. However, these figures are low and indicate that the ICON is not necessarily a suitable predictor for aesthetics, function, speech and treatment need for those individuals of the normal population attending routine dental care. This may be explained by the fact that patients who have had no exposure to orthodontic treatment may not regard discrepancies in occlusion to be unattractive or require treatment, but the clinician, who considers a spectrum of malocclusions ranging from minor to major, following objective assessment of the occlusion may disagree. Professionals tend to recommend orthodontic treatment in 10–12% more cases compared with lay persons.11
The cross-tabulation analysis of ICON scores and treatment need (Tables 5, 6) demonstrated that for both genders the ICON showed good sensitivity but poor specificity. That is, the ICON was good at detecting those patients requiring treatment but was not so good in rejecting those patients who did not need treatment. Although there may be an objective need for orthodontic treatment this may not be followed by the patient's desire to seek treatment. It appears difficult to predict the patients' attitudes to the arrangement of their teeth and their perceptions of need using a single index. However, if the index is accompanied by a simple question to determine whether the patient desires treatment this determines the professional's objective and individual's perceived need. Adult patients were more likely to decline treatment than younger patients. The level of difficulty may aid in matching the patient to appropriate clinicians to undertake the treatment.
Conclusion
The ICON attempts to incorporate both patients' and clinicians' perceptions regarding orthodontic treatment need in a single index. In terms of provision of orthodontic care, the importance of this cannot be under-estimated as it is ultimately the patients who are receiving treatment and need to gain satisfaction from improved aesthetics and function, and the clinicians who assess treatment need and set standards for the acceptability of the outcome of orthodontic treatment.
In this study, the ICON was found to correlate with patients' opinions of aesthetics, function, speech and treatment need. The strength of association, however, was low and it would be valuable to undertake similar studies with a larger number of subjects and, perhaps, in different dental care provider settings.
It can be concluded that the ICON alone is not necessarily a suitable predictor for appearance, function, speech or treatment need for those individuals attending general dental practice for routine dental care. In combination with a simple question to assess the patients' desire for treatment, the shared decision for any particular individual to enter the treatment process can be determined.

References
Brook P H, Shaw W C. The development of an Orthodontic Treatment Priority Index. Eur J Orthod 1989; 11: 309–320.
Richmond S. The development of the PAR Index (Peer Assessment Rating): reliability and validity. Eur J Orthod 1992; 14: 125–139.
Baume L J, Marechaux S. Uniform methods for the epidemiologic assessment of malocclusion. Am J Orthod 1974; 66: 121–129.
Mclain J B, Proffit W R. Oral health status in the United States: prevalence of malocclusion. J Dent Educ 1985; 49: 386–396.
Daniels C P, Richmond S. The Development of the Index of Complexity, Outcome and Need (ICON). J Orthod 2000; 27: 149–162.
Roberts C T, Richmond S. The design and analysis of reliability studies for the use of epidemiological and audit indices in orthodontics. Br J Orthod 1997: 24: 139–147.
Shue-Te Yeh M, Koochek AR, Vlaskalic V, Boyd R, Richmond S. The relationship of 2 professional occlusal indexes with patients' perceptions of aesthetics, function, speech, and orthodontic treatment need. Am J Orthod Dento Orthopedics 2000; 118: 421–428.
Pietila T, Pietila I. Dental appearance and orthodontic services assessed by 15-16 year-old adolescents in eastern Finland. Community Dent Health 1996; 13: 139–144.
Birkeland K, Boe O E, Wisth P J. Subjective assessment of dental and psychological effects of orthodontic treatment. J Orofacial Orthop 1997; 58: 44–61.
Burden D J, Pine C M. Self-perception of malocclusion among adolescents. Community Dent Health 1995; 12: 89–92.
Vally I. A comparison of lay and professional opinion on treatment need and treatment outcome. MScD Thesis University of Wales College of Medicine, 1997.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed paper
Appendix 1 ICON – Index of Complexity, Outcome and Need
Appendix 1 ICON – Index of Complexity, Outcome and Need
-
Based on expert opinion of 97 practising specialist orthodontists from Germany, Greece, Hungary, Italy, Netherlands, Norway, Spain, United Kingdom and the USA
-
For use on patients or dental casts
-
A single assessment method to record complexity, outcome and need
-
For use in clinical governance, audit, research and decision making
-
Five components, taking about 1 minute to measure
The aesthetic component was first published as a scan. Evans R, Shaw W C. A Preliminary evaluation of an illustrated scale for rating dental attractiveness Eur J Orthod, 1987; 9:314-318.
Component I Aesthetic assessment
Ten pictures ranking dental attractiveness
Component 2 Upper arch crowding/spacing
-
The difference between the sum of the mesio-distal tooth diameters and the available arch circumference in the upper arch reduced to a 5-point score
-
Impacted teeth in either arch immediately score 5
Impacted teeth must be unerupted and either:
a)Ectopic or impacted against an adjacent tooth (excluding third molars but including supernumerary teeth)
b)Possess less than or equal to 4 mm of space between the adjacent permanent teeth. Use average canine and premolar widths to estimate the potential crowding in the mixed dentition, namely, 7 mm for pre-molars, lower canine, and 8 mm for upper canine
-
Spacing in one part of the arch will cancel out crowding elsewhere
-
Retained deciduous teeth (without permanent successor) and erupted supernumerary teeth score as space (unless they are to be retained to obviate the need for prosthesis)
-
Lost teeth caused by trauma or extraction should be counted as space (unless space is maintained for a prosthetic replacement).
Component 3 Crossbite
-
Anterior and posterior transverse discrepancies of cusp to cusp or greater m intercuspal position
Component 4 Incisor open bite/overbite
-
Open bite (except developmental conditions) is measured to the mid-incisal edges
-
Deep bite is measured to deepest part of overbite
-
If both traits are present only the highest score is counted
Component 5 Buccal segment antero-posterior
-
Quality of buccal segment interdigitation is measured (not Angle's classification)
-
Both sides are scored then added together
B. Icon scoring protocol
-
Measure all 5 traits according to the protocol above to obtain a set of scores
-
Multiply the scores by their respective weights
-
The sum of the weighted scores is the ICON score for the case
-
Pre-treatment scores give the treatment need and complexity grades
-
End of treatment scores gives the acceptability
-
Pre-treatment –4 x post treatment scores gives the degree of improvement
B.ICON® Copyright University of Wales College of Medicine
Further information can be obtained from: Professor S. Richmond, Department of Dental Health and Development UWCM, University Dental Hospital, Heath Park, Cardiff CFI4 4XY Great Britain Tel/Fax: #44(0)29 2074 2451 email: richmonds@cardiff.ac.uk
Rights and permissions
About this article
Cite this article
Koochek, AR., Shue-Te Yeh, M., Rolfe, B. et al. The relationship between Index of Complexity, Outcome and Need, and patients' perceptions of malocclusion: a study in general dental practice. Br Dent J 191, 325–329 (2001). https://doi.org/10.1038/sj.bdj.4801175
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4801175
This article is cited by
-
Agreement of young adults and orthodontists on dental aesthetics & influencing factors of self-perceived aesthetics
BMC Oral Health (2018)
-
Validity assessment and determination of the cutoff value for the Index of Complexity, Outcome and Need among 12–13 year-olds in Southern Chinese
International Journal of Oral Science (2012)
