
Abstract
Objective To conduct a systematic review of the literature on the longevity of routine dental restorations in permanent posterior teeth, and to identify and examine factors influencing its variability.
Method Accepted guidelines were followed. An advisory group oversaw the project. Simple Class I and Class II amalgam, composite resin, glass ionomer and cast gold restorations were covered. Comprehensive searching of electronic databases, hand-searching, and location of 'grey' literature, generated 124 research reports. Those considered relevant were assessed for validity and quality according to agreed criteria. The analysis was descriptive.
Results Eight of 58 relevant research reports were categorised, according to agreed criteria, as being of satisfactory validity and quality. They suggested that 50% of all restorations last 10 to 20 years, although both higher and lower median survival times were reported. The findings were supported by the totality of studies reviewed. However, variability was substantial. Restoration type, materials, the patient, the operator, the practice environment and type of care system appeared to influence longevity.
Conclusions Many studies were imperfect in design. Those considered to be the most appropriate for analysis were too limited to undertake a formal statistical exploration. Therefore there remains a need for definitive randomised controlled trials of restoration longevity, of sound design and adequate power, employing standardised assessments and appropriate methods of analysis.
Similar content being viewed by others

Main
The durability, or longevity, of a dental restoration is clearly a salient factor in determining its effectiveness as a presumed long-term treatment for caries. Yet despite the very large number of fillings placed annually by the profession, how long a routine restoration can, or should, be expected to stay functionally intact remains a matter of uncertainty. In order to collate, assess and draw conclusions from the available evidence, it was evident that a systematic review of the literature on longevity should be undertaken, no previous exercise of this kind having been identified. A comprehensive search was therefore initiated which revealed a body of work that might be suitable for inclusion.1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124 This paper aims to provide a condensed, easily assimilable version of the full review,125 the objectives of which were to establish from research reports of satisfactory quality the longevity of different types of routine dental restoration in permanent posterior teeth, and its variability; and to identify and examine factors (referred to as effect modifiers) influencing the durability of restorations.
Method
Conduct of the review
The review was conducted in general accordance with guidelines promulgated by the NHS Centre for Reviews and Dissemination (CRD),126 and the Cochrane Collaboration.127 An advisory group was formed at the outset to assist the principal researcher (NAA) and act as consultants to the project. The group consisted of the remaining authors of the current report whose collective knowledge was considered to cover the areas of relevant expertise. Its task was to decide the scope of the review and the specific questions to be addressed; to approve and finalise the protocol; to monitor progress in identifying studies and deciding on their suitability for inclusion (assessment of validity); to discuss the proposals for analysis of the material and completion of the review; and to agree the final report. A meeting of the group and principal researcher took place at each stage. In addition, advice and guidance was obtained from the Systematic Review Unit at the Institute of Child Health, University College London.
Inclusion and exclusion criteria
Resources were limited and it was necessary to place some constraints on the scope of the review. Evaluations of the clinical performance of Class I (occlusal) and Class II (mesial-occlusal, distal-occlusal, mesial-occlusal-distal) restorations in permanent teeth, the commonest type of conservative treatment, predominate in the literature. It was therefore determined that the review should be confined to an assessment of the longevity of simple amalgam, composite resin, glass ionomer and cast gold restorations of those two types. A simple restoration was defined as one not requiring any form of additional retention measures.
Search strategy
Through a comprehensive search, an attempt was made to identify all relevant studies irrespective of language. Available electronic databases, MEDLINE, EMBASE, CINAHL, DISSERTATION ABSTRACTS and ERIC were searched from their date of inception together with ISTP. Conference proceedings were searched using the citation index SCISEARCH. The subject headings or key components used included dental restoration, longevity, failure, durability, survival analysis, and life table analysis. In addition, the Cochrane Controlled Trials Register (CCTR) in the Cochrane Library (1998 Issue 2) was scrutinised for any relevant trials and cross checked with those already retrieved.
Bibliographies of research reports identified through the search were checked for further relevant references. These were sought as a citation on the SCISEARCH database. An attempt was also made to obtain copies of unpublished or unlisted studies, referred to as 'grey literature', by writing to key authors in the subject area. Five authors from the UK and 15 from overseas were approached. 'Grey literature' was taken to include any pertinent material not indexed on the main databases. Apart from this, no attempt was made to contact the author of any publication to seek additional information about a study. To complete the process, prospective hand-searching of all studies by key authors identified in the review was carried out and cross referencing performed with studies identified from the previous search strategies. It was established from the MEDLINE system for identifying systematic reviews126 that none within the subject area had been carried out previously.
Study selection
The literature search produced many studies that did not meet the criteria agreed by the advisory group or were outside the scope of the review. From the totality of material obtained from the search process, using agreed criteria each member assessed independently, which studies should go forward for further evaluation. Testing the level of agreement on the content of the list between the principal investigator and each of the four other assessors yielded kappa values of 0.60, 0.40, 0.75 and 0.65 respectively, indicating fair to reasonable agreement.128 The studies were then grouped according to those selected by three or more of the five assessors and those selected by two or fewer. The first selection, intended for prospective inclusion, was then further checked for duplication. Only the latest article was retained where several updating the same study had been published over time. However, multiple publications reporting different aspects of the same study were admitted as separate work. If agreement could not be reached by the assessors a study was excluded.
Assessment of validity and quality
The criteria used by the advisory group in the assessment of quality are presented in Table 1. For the purposes of the review, only studies that had a period of observation of at least 5 years were considered. The type of design (A) was divided into six sub-categories plus abstracts (designated as 7). Fulfilment of each criterion from B through to I inclusive, was categorised simply as 'yes' or 'no'. With regard to the outcome measures reported (I), use of an appropriate method of expressing longevity was considered important since unorthodox measures militate against valid comparisons between studies. In longitudinal studies, appropriate expressions of longevity were regarded as those which involved a formal statistical analysis of survival, such as life table or product-limit (Kaplan-Meier) estimates of survival functions. The Survival Distribution Function (SDF), often referred to simply as 'survival', for a specified time interval (t) is an estimate of the probability that an individual restoration from the population will have a lifetime exceeding t.129 The survival time associated with SDF = 0.5 is frequently termed the median survival time (MST), in other words the lifetime which any individual restoration has a 50% chance of exceeding (designated as 8 in Table 1). Another appropriate expression is the proportion of the initial number of restorations that remain in service after specific survival times, for example, 5- or 10-year cumulative survival percentages (designated as 9).67 In cross-sectional studies involving retrospective case record examination, the term median age or longevity (designated as 10) is commonly encountered. It is the functional period of the 50th percentile of restorations deemed to have failed. Whatever expression of longevity is used, precautions must be observed regarding adequate length of observation and the effect of data being censored as a result of premature withdrawal.67 Data extraction was performed by the principal researcher (NAA) using a previously prepared proforma (see Table 2). Reliability of data extraction was re-checked and any disagreements referred to the group for final decision.
Data synthesis and analysis
The cut-off point determined by the advisory group to delineate studies of 'adequate' quality from those of 'unsatisfactory ' quality was a score of six 'yes' ratings and above on the assessment criteria. Characteristics recorded were design type; practice setting; consideration of effect modifiers; comparison of alternative materials; randomisation in sampling (ie random allocation of patients or teeth to a filling material); period of observation; appropriateness of analysis; and the main findings (see Table 3). Heterogeneity among the studies, particularly in respect of the varying quality and presentation of results, precluded use of statistical methods of pooling data, such as meta-analysis. In order to better explain the data, descriptive analysis was used with the studies grouped according to:
-
The 'adequacy' of quality, based on an assessment score of at least six 'yes' responses
-
The main outcome measure used in the studies considered to be of 'adequate' quality, and the longevity of restorations estimated in these studies
-
The defining of 'failure', 'survival' or criteria for replacement, and the consideration of effect modifiers.
Results
Study selection
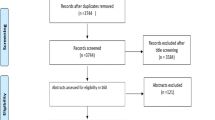
Fifty-eight research reports were selected by three or more of the five assessors as meeting the agreed criteria for inclusion in the review.1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58 Of these, eight were eventually considered to be of adequate validity and quality. Sixty-six reports were excluded.59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124 Of the 58 studies initially selected, three were subsequently discarded as they were not primary data sources.13,30,32 The investigation by Lavelle consisted of a longitudinal retrospective and a cross-sectional study and these were considered separately.24 One study came to light after completion of the search process.130 The final list of studies which were assessed for validity and quality is presented in Table 2 together with their ratings according to the assessment criteria presented in Table 1.
Assessment of validity and quality
Scrutiny of the assessment ratings of the studies, shown in Table 2, indicated that the majority satisfied between three and five of the 'yes/no' criteria. The modal score of four was obtained by 14 studies; 25% of those selected. Longitudinal retrospective designs, the largest proportion of the studies included (36%), had a modal score of five 'yes' ratings (32%). Cross-sectional investigations had a modal score of four. Only eight studies achieved at least six 'yes' scores and thus satisfied the criteria of being of 'adequate' quality. Of these, six were of longitudinal retrospective design,3,10,11,18,26,47one was a longitudinal prospective study,21 and one was a non- randomised clinical trial.56 None of the randomised controlled trials or cross-sectional studies originally selected achieved this score. The studies by Bentley and Drake3 and Drake10,11 were regarded as being independent.
Outcome measures
The main outcome measure reported in the eight reports judged of 'adequate' quality was median survival time (MST). This was used in six studies (Bentley and Drake,3 Drake,10,11 Hawthorne and Smales,18 Jokstad and Mjor,21 Robbins and Summitt,47). Only two reported survival/failure rate as the sole outcome measure (Letzel et al.,26 Wilson and Norman,56) while four used both MST and survival/failure rate.3,10,11,21
Findings on longevity
Table 3 shows the high degree of variability reported between the validated studies which made it difficult to determine an average period of time over which restorations would last. Nevertheless, the results suggest that 50% of all restorations can be expected to survive between 10 and 20 years although both lower and higher values were recorded. For amalgam restorations, the results suggested a range of 50% survival from a low of 5–8 years recorded by Jokstad and Mjor for seven practitioners in public and private practice in Scandinavia,21 to around 23 years reported by Hawthorne and Smales18 for 20 dentists in three private Adelaide dental practices. An intermediate value of 11.5 years was reported by Robbins and Summitt47 in a study of Australian military personnel. For other filling materials, the findings were conflicting. Hawthorne and Smales18 reported a MST of 17 years for composite restorations and 14 for cast gold; both less than for amalgam. They also showed that the durability of glass ionomer was rather less than that of composite resin and it should not be considered for posterior occlusal or approximal restorations. On the other hand Bentley and Drake3 reported that 91% of cast gold, 72% of amalgam and 56% of composite fillings survived at the conclusion of their 10-year study.
Other considerations
The defining of 'failure', 'survival' or criteria for restoration replacement, and the examination of effect modifiers in studies were also considered in the review. The term 'failure' rather than 'survival' was generally used, although in the eight validated studies, the definitions of these varied. The preferred criteria were those of Robinson,48 and the USPHS system used by Wilson and Norman.56 Letzel et al.26 and Robbins and Summitt,47 defined their own criteria for replacement.
Some influence from effect modifiers was suggested by the validated studies. For example, occlusal amalgams lasted significantly longer than multi-surface amalgams, and single surface composites fared better than multi-surface ones.3 Durability was reduced in dental students' patients more than 60-years-old3 but was reportedly increased in patients more than 38-years-old treated by Scandinavian dentists.21 In the latter study, survival was also shown to be dependent on the operator and on caries activity.
Discussion
Analytical considerations
Stepwise plots (Kaplan Meier curves) of SDF against time have deservedly become popular in studies of restoration longevity but it is important that researchers interpret them correctly. The SDF, being a probability, must range from 0 to 1 but is not, as it may appear, an indicator of the proportion of restorations surviving after specific time intervals11 unless, improbably, 100% of restorations have been followed up and all have failed. Survival analysis methods, unlike simple proportions, are able to make use of survival information from cases that are right-censored as a result of loss from recall before failure, as well as from units that remain in service at the end of the study period. Both MST and cumulative survival percentages have been reported in the studies reviewed. However there are difficulties in comparing results from investigations that depend on only one of these analytical approaches, as discussed fully by Djemal et al.131 An additional complication is that when failure rates are low, it may be necessary to wait a long time before it is possible to compute the MST.
On a further point, it is worth noting that MST is not the median of the recorded survival times for the whole group of restorations, nor for the failed or surviving subgroups. It is also not the 'half-life', or time taken for 50% of restorations to fail, a statistic which requires observation of the sample until that failure proportion is reached. An alternative life-table method is to generate an estimate of the time elapsed before reduction of the number of restorations to one-half. This is the Median Residual Lifetime (MRL). The danger of confusing terms containing the adjective 'median', such as MRL and median age or longevity, is clear. A 5-year cut-off point on observation times was imposed since it was considered that any attempt to assess longevity from a shorter study period would be unacceptably imprecise.
Study selection
In assessing the quality and validity of studies for inclusion in the review, considerable importance was given to the clinical examiners being trained and calibrated, and using well-defined and standardised criteria for 'failure', 'survival' or restoration replacement. Elderton73 considered that without proper and universally acceptable guidelines, assessment of the quality of restorations would remain very subjective. Nevertheless, Mjor29 and Allander et al.60 have suggested that examiners who are not standardised have the advantage of using their own judgment and therefore represent the true position in clinical practice. There is little doubt that ecological studies of the natural history of restorations in the practice situation can give valuable insight into effect modifiers such as the dental care system or environment, and the influence, if any, of the way in which practitioners are remunerated, although such studies may not rate highly in the hierarchy of acceptable evidence.
Effect modifiers
Overall there was a high degree of variation and non-standardised use of definitions among the investigations reviewed and the statistical significance, or non significance, of effect modifiers depended to a great extent on study design. Therefore, although any generalisations would appear to be of questionable value, taking into account the totality of studies selected, the review did give some fairly strong indications of factors that probably influence longevity. As regards the patient, effect modifiers include age3,21 and having a high caries activity which has a negative influence on restoration survival.11,21 Secondary caries was the most frequently cited reason for failure or replacement5,14,15,22,23,24,44,46,58 followed by fractured fillings. However, two studies reported fractured fillings as the prime reason.31,49 From the operator viewpoint, inserting restorations that have the maximum likelihood of survival is one of the most important factors in securing a health gain for the patient and here the choice of filling material is clearly relevant. Another factor is the avoidance of surgical treatment of carious lesions confined to enamel. This results in the avoidable destruction of tooth tissue and negates any possible health gain from the intervention.132 It is evident that dentists' attitudes, the circumstances in which they practice and the system of their remuneration, and also patient behaviour in seeking treatment, are possible effect modifiers in determining the decision to place or replace restorations. The MST of amalgam fillings provided in the General Dental Service in Scotland under fee for service conditions was found by Elderton12 to be less than 5 years. Also patients who changed dentists were likely to receive nearly twice as many restorations as those who stayed with the same practitioner.7 On the other hand, the MST of restorations provided for military personnel by salaried dental officers has been reported as between 10 and 20 years,9,28,47 irrespective of changes of practitioner.9 The differing modes of remuneration may partly explain the difference.9
Longevity of restorations
Most of the studies categorised as being of 'adequate' quality were comparative. They used appropriate outcome measures and tended to employ few clinical examiners working to carefully defined criteria. Other studies reviewed met fewer of the quality assessment criteria, but it is nonetheless instructive to consider their findings on longevity. Those which used median survival time as the outcome measure are the most readily grouped. With regard to amalgam fillings, a few reported a MST of 5 years or less,4,12,14,36,37 the majority a MST in the range of 6–10 years,2,5,6,20,23,24,27,29,42,44,45,48,49,55,58 and others a MST in the range of 11–20 years.9,16,22,28,34,51 Fewer studies involved tooth-coloured filling materials. For resin composite, a handful reported a MST of 5 years or less,12,15,35,37,44 and the majority a MST in the range of 6–10 years.22,27,29,34,38,42,55,58 One study reported a MST of more than 14 years.9 There is little useful evidence on the durability of glass ionomer restorations since most studies report an observation period short of 5 years. As regards cast gold restorations, one study reported a MST of less than 10 years.6 However, three others have reported MSTs of between 10 and 20 years,22,27,33 while one reported a median age of 34 years for gold restorations in a selected practice.39
Conclusion
A major difficulty in conducting the review was trying to draw valid conclusions from a large mass of disparate data, much of which was generated in studies with imperfections in their design. For example, even in those investigations which were for the most part methodologically sound, there was little indication that the unit of analysis adopted was the person rather than the individual restoration. The possibility of colinearity in the properties of restorations within the same mouth was not generally recognised. While it is acknowledged that conducting scientifically rigorous investigations in this subject area is fraught with great practical difficulty, there remains a challenging need for definitive comparative studies of the longevity of routine dental restorations, designed as long term, randomised controlled trials, using sample sizes of adequate power, trained and calibrated assessors, well-defined standard criteria of survival/failure, and appropriate outcome measures and methods of analysis.
References
Akerboom H B M, Advokaat J G A, Amerongen W E van, Borgmeijer P J . Long-term evaluation and re-restoration of amalgam restorations. Community Dent Oral Epidemiol 1993; 21: 45–48.
Allan D N . A longitudinal study of dental restorations. Br Dent J 1977; 143: 87–89.
Bentley C, Drake C W . Longevity of restorations in a dental school clinic. J Dent Educ 1986; 50: 594–600.
Bjertness E, Sonju T . Survival analysis of amalgam restorations in long-term recall patients. Acta Odontolol Scand 1990; 48: 93–97.
Burke F T J, Cheung S W, Mjor I A, Wilson N H F . Restoration longevity and analysis of reasons for the placement and replacement of restorations provided by vocational dental practitioners and their trainers in the UK. Unpublished ms 1998. ('grey literature').
Crabb H S M . The survival of dental restorations in a teaching hospital. Br Dent J 1981; 150: 315–322.
Davies J A . The relationship between change of dentist and treatment received in the General Dental Service. Br Dent J 1984; 157: 322–324.
Dawson A S, Smales R J . The influence of examination frequency and changing dentist on dental treatment provision in an Australian defense force population. Br Dent J 1992; 173: 237–241.
Dawson A S, Smales R J . Restoration longevity in an Australian Defense Force population. Aust Dent J 1992; 37: 196–200.
Drake C W . A comparison of restoration longevity in maxillary and mandibular teeth. J Am Dent Assoc 1988; 116: 651–654.
Drake C W . Dental restoration longevity: survival functions and statistical indices in low and high failure rate groups. Community Dent Oral Epidemiol 1988; 16: 258–262.
Elderton R J . Longitudinal study of dental treatment in the general dental service in Scotland. Br Dent J 1983; 155: 91–96.
El-Mowafy O M, Lewis D W, Benmergui C, Levinton C . Meta-analysis on long-term clinical performance of posterior composite restorations. J Dent 1994; 22: 33–43.
Friedl K H, Hiller K A, Schmalz G . Placement and replacement of amalgam restorations in Germany. Oper Dent 1994; 19: 228–232.
Friedl K H, Hiller K A, Schmalz G . Placement and replacement of composite restorations in Germany. Oper Dent 1995; 20: 34–38.
Gray J C. An evaluation of the average lifespan of amalgam restorations. MSc report. London: University of London, 1976 ('grey literature').
Hamilton J C, Moffa J P, Ellison J A, Jenkins W A . Marginal fracture not a predictor of longevity for two amalgam alloys: a ten-year study. J Prosthet Dent 1983; 50: 200–202.
Hawthorne W S, Smales R J . Factors influencing long-term restoration survival in three private dental practices in Adelaide. Aust Dent J 1997; 42: 59–63.
Hendriks F H, Letzel H, Vrijhoef M M . Cost benefit analysis of direct posterior restorations. Community Dent Oral Epidemiol 1985; 13: 256–259.
Hunter B . Survival of dental restorations in young patients. Community Dent Oral Epidemiol 1985; 13: 285–287.
Jokstad A, Mjor I A . Analyses of long-term clinical behavior of class-II amalgam restorations. Acta Odontol Scand 1991; 49: 47–63.
Jokstad A, Mjor I A, Qvist V . The age of restorations in situ. Acta Odontol Scand 1994; 52: 234–242.
Klausner L H, Green T G, Charbeneau G T . Placement and replacement of amalgam restorations: a challenge for the profession. Oper Dent 1987; 12: 105–112.
Lavelle C L B . A cross-sectional longitudinal survey into the durability of amalgam restorations. J Dent 1976; 4: 139–143.
Letzel H, van't Hof M A, Vrijhoef M M, Marshall G W Jr, Marshall S J . A controlled clinical study of amalgam restorations: survival, failures, and cause of failure. Dent Mater 1989; 5: 115–121.
Letzel H, van't Hof M A, Marshall G W Jr, Marshall S J . The influence of the amalgam alloy on the survival of amalgam restorations: a secondary analysis of multiple controlled clinical trials. J Dent Res 1997; 76: 1787–1798.
Mahmood S, Smales R J . Longevity of dental restorations in selected patients from different practice environments. Aust Dent J 1994; 39: 15–17.
Mayhew M T . An evaluation of the average life span of posterior amalgam restorations in the Royal Air Force. MSc report. London: University of London, 1995.
Mjor I A . The reasons for replacement and the age of failed restorations in general dental practice. Acta Odontol Scand 1997; 55: 58–63.
Mjor I A, Burke F J T, Wilson N H F . The relative cost of different restorations in the UK. Br Dent J 1997; 182: 286–289.
Mjor I A, Jokstad A . Five-year study of Class II restorations in permanent teeth using amalgam, glass polyalkenoate (ionomer) cerment and resin-based composite materials. J Dent 1993; 21: 338–343.
Mjor I A, Jokstad A, Qvist V . Longevity of posterior restorations. Int Dent J 1990; 40: 11–17.
Mjor I A, Medina J E . Reasons for placement, replacement, and age of gold restorations in selected practices. Oper Dent 1993; 18: 82–87.
Mjor I A, Moorhead J . Selection of restorative materials. Reasons for failures and longevity of restorations in Florida. J Dent Res 1998; 77 (Special Issue A): 244.
Mjor I A, Toffenetti F . Placement and replacement of resin-based composite restorations in Italy. Oper Dent 1992; 17: 82–85.
Mjor I A, Toffenetti F . Placement and replacement of amalgam restorations in Italy. Oper Dent 1992; 17: 70–73.
Mjor I A, Um C M . Survey of amalgam and composite restorations in Korea. Int Dent J 1993; 43: 311–316.
Nordbo H, Leirskar J, Von der Fehr, F R . Saucer-shaped cavity preparations for posterior approximal resin composite restorations: Observations up to 10 years. Quintessence Int 1998; 29: 5–11.
Nordbo H, Lyngstadaas S P . The clinical performance of two groups of functioning class-II cast gold inlays. Acta Odontol Scand 1992; 50: 189–192.
Osborne J W, Norman R D . A 13-year clinical assessment of 10 amalgam alloys. Dent Mater 1990; 6: 189–194.
Osborne J W, Norman R D, Gale E N . A 14-year clinical assessment of 12 amalgam alloys. Quintessence Int 1991; 22: 857–864.
Paterson N . The longevity of restorations: a study of 200 regular attenders in a general dental practice. Br Dent J 1984; 157: 23–25.
Pieper K, Meyer G, Marienhagen B, Motch A . Eine langzeitstudie an amalgam-und kuntstoff-fullungen ( A long term study of amalgam and composite fillings). Dtsch Zahnarztl Z 1991; 46: 222–225.
Pink F E, Minden N J, Simmonds S . Decisions of practitioners regarding placement of amalgam amd composite restorations in general practice settings. Oper Dent 1994; 19: 127–132.
Qvist J, Qvist V, Mjor I A . Placement and longevity of amalgam restorations in Denmark. Acta Odontol Scand 1990; 48: 297–303.
Qvist V, Qvist J, Mjor I A . Placement and longevity of tooth-colored restorations in Denmark. Acta Odontol Scand 1990; 48: 305–311.
Robbins J W, Summit J B . Longevity of complex amalgam restorations. Oper Dent 1988; 13: 54–57.
Robinson A D . The life of a filling. Br Dent J 1971; 130: 206–208.
Rytomaa I, Murtomaa H, Turtola L, Lind K . Clinical assessment of amalgam fillings. Community Dent Oral Epidemiol 1984; 12: 169–172.
Smales R J . Longevity of cusp-covered amalgams: survival after 15 years. Oper Dent 1991; 16: 17–20.
Smales R J, Webster D A, Leppard P I, Dawson A S . Prediction of amalgam restoration longevity. J Dent 1991; 19: 18–23.
Smales R J . Longevity of low- and high-copper amalgams analyzed by preparation class, tooth site patient age and operator. Oper Dent 1991; 16: 162–168.
Van Dijken J W . A six year follow-up of three dental alloy restorations with three different copper contents. Swed Dent J 1991; 15: 259–264.
Walls A W G, Wallwork M A, Holland I S, Murray J J . The longevity of occlusal amalgam restorations in first permanent molars of child patients. Br Dent J 1985; 158: 133–136.
Welbury R R, Walls A W G, Murray J J, McCabe J F . The management of occlusal caries in permanent molars. A 5-year clinical trial comparing a minimal composite with an amalgam restoration. Br Dent J 1990; 169: 361–366.
Wilson N H, Norman R D . Five-year findings of a multiclinical trial for a posterior composite. J Dent 1991; 19: 153–159.
Wilson N H, Wastell D G, Norman R D . Five year-performance of high-copper content amalgam restorations in a multiclinical trial of a posterior composite. J Dent 1996; 24: 203–210.
York A K, Arthur J S . Reasons for placement and replacement of dental restorations in the United States Navy Dental Corps. Oper Dent 1993; 18: 203–208.
Allan D N . The durability of conservative restorations. Br Dent J 1969; 126: 172–177.
Allander L, Birkhed D, Bratthal D . Reasons for replacement of Class II amalgam restorations in private practice. Swed Dent J 1990; 14: 179–184.
Anusavice J A . Conference report: Criteria for placement and replacement of dental restorations. J Dent Res 1988; 67: 795–796.
Burke F J T, Mjor I A, Cheung S W, Wilson N H F . Reasons for placement and replacement of restorations in vocational training. J Dent Res 1998; 77 (Special Issue A): 114.
Cheetham J D, Makinson O F, Dawson A S . Replacement of Cu amalgams by a group of dental practitioners. Aust Dent J 1991; 38: 218–222.
Christensen G J . Alternatives for the restoration of posterior teeth. Int Dent J 1989; 39: 155–161.
Christensen G J . The practicability of compacted golds in general practice - survey. J Colo Dent Assoc 1971; 18–22.
Dahl J E, Eriksen H M . Reasons for replacement of amalgam dental restorations. Scand J Dent Res 1978; 86: 404–407.
Davies J A . Dental restoration longevity: a critique of the life table method of analysis. Community Dent Oral Epidemiol 1987; 15: 202–204.
Deligeorgi V, Wilson N H F, Fouzas D, Kouklaki E, Burke F J T, Mjor I A . Reasons for the provision of restorations in student clinics. J Dent Res 1998; 77 (Special Issue A): 137.
Doglia R, Herr P, Holz J, Baume L J . Clinical evaluation of four amalgam alloys: a five-year report. J Prosthet Dent 1986; 56: 406–415.
Drake C W, Maryniuk G A, Bentley C . Reasons for restoration replacement: differences in practice patterns. Quintessence Int 1990; 21: 125–130.
Eddie S . Frequency of attendance in the General Dental Service in Scotland. A comparison with claimed attendance. Br Dent J 1984: 157; 267–270.
Elderton R J . The prevalence of failure of restorations: a literature review. J Dent 1976; 4: 207–210.
Elderton R J . Assessment of the quality of restorations: A literature review. J Oral Rehabil 1977; 4: 217–226.
Elderton R J . Clinical studies concerning re-restoration of teeth. Adv Dent Res 1990; 4: 4–9.
Elderton R J . The durability of restorations in the General Dental Service. J Dent Res 1983; 62: 434.
Elderton R J . The causes of failure of restorations: a literature review. J Dent 1976; 4: 257–262.
Elderton R J, Al-Ansary I S . Influence of the dentist in the survival of dental restorations. J Dent Res 1991; 70 (Special Issue): 684.
Elderton R J, Nuttall N M . Variation among dentists in planning treatment. Br Dent J 1983; 154: 201–206.
Gryst M E I, Mount G J . The use of glass-ionomer in special needs patients. Unpublished ms 1998 ('grey literature').
Healy H J, Phillips R W . A clinical study of amalgam failures. J Dent Res 1949; 28: 439–446.
Jacobsen P H . The clinical evaluation of amalgam alloys. Br Dent J 1984; 157: 436–439.
Jokstad A . Class 2 cavity preparation and restoration performance. PhD thesis, Oslo: University of Oslo, 1992.
Jokstad A, Mjor I A . The quality of routine class II cavity preparations for amalgam. Acta Odontol Scand 1989; 47: 53–64.
Kelsey W P, Franco S J, Blankenau R J, Cavel W T, Barkmeier W W . Caries as a cause of restoration replacement: a clinical survey. Quintessence Int 1981; 12: 971–974.
Knibbs P J . Glass ionomer cement: 10 years of clinical use. J Oral Rehabil 1988; 15: 103–115.
Lacy A M . A critical look at posterior composite restorations. J Am Dent Assoc 1987; 114: 357–362.
Leempoel P J B, Van't Hof M A, De Haa A F J . Survival studies of dental restorations: criteria, methods and analyses. J Oral Rehabil 1989; 16: 387–394.
Leinfelder K F . Posterior composite resins: the materials and their clinical performance. J Am Dent Assoc 1995; 126: 663–676.
Leinfelder K F, Sluder T B, Santos J F F, Wall J T . Five-year clinical evaluation of anterior and posterior restorations of composite resin. Oper Dent 1980; 5: 57–65.
Mahler D B, Marantz R . The effect of the operator on the clinical performance of amalgam. J Am Dent Assoc 1979; 99: 38–41.
Maryniuk G A . Clinicians' perceptions of restoration longevity. J Dent Educ 1985; 49: 769–772.
Maryniuk G A . In search of treatment longevity — a 30-year perspective. J Am Dent Assoc 1984; 109: 739–744.
Maryniuk G A, Kaplan S H . Longevity of restorations: survey results of dentists' estimates and attitudes. J Am Dent Assoc 1986; 112: 39–45.
Matis B A, Carlson T, Cochran M, Phillips R W . How finishing affects glass ionomers. Results of a five-year evaluation. J Am Dent Assoc 1991; 122: 43–46.
Matis B A, Cochran M, Carlson T . Longevity of glass-ionomer restorative materials: results of a 10-year evaluation. Quintessence Int 1996; 27: 373–382.
Mjor I A . Long term cost of restorative therapy using different materials. Scand J Dent Res 1992; 100: 60–65.
Mjor I A . Placement and replacement of restorations. Oper Dent 1981; 6: 49–54.
Mjor I A . Problems and benefits associated with restorative materials; side-effects and long- term costs. Adv Dent Res 1992; 6: 7–16.
Mjor I A . Repair versus replacement of failed restorations. Int Dent J 1993; 43: 466–472.
Mjor I A, Dahl J E, Moorhead J E . Longevity of restorations. Unpublished ms. 1998. ('grey literature').
Moore D L, Stewart J L . Prevalence of defective dental restorations. J Prosthet Dent 1967; 17: 372–378.
Mount G J . Restoration with glass ionomer cement: Requirements for clinical success. Oper Dent 1981; 6: 59–65.
Mount G J . Longevity of glass ionomer cements. J Prosthet Dent 1986; 55: 682–685.
Mount G J . Longevity in glass-ionomer restorations: Review of a successful technique. Quintessence Int 1997; 28: 643–650.
Norman R D, Wright J S, Rydberg R J, Felkner L L . A 5-year study comparing a posterior composite resin and an amalgam. J Prosthet Dent 1990; 64: 523–529.
Nuttall N M . General Dental Service treatment received by frequent and infrequent dental attenders in Scotland. Br Dent J 1984; 156: 363–366.
Nuttall N M, Elderton R J . The nature of restorative dental treatment decisions. Br Dent J 1983; 154: 363–365.
Osborne J W, Berry T G . The effect of setting time on the clinical performance of a high-copper amalgam alloy. Oper Dent 1995; 20: 26–29.
Osborne J W, Binon P P, Gale E N . Dental amalgam: clinical behavior up to eight years. Oper Dent 1980; 5: 24–28.
Porter K H, Marshall T D, Re G J . A cost-effective restoration. Oper Dent 1988; 13: 94–95.
Qvist V, Thylstrup A, Mjor I A . Restorative treatment pattern and longevity of amalgam restorations in Denmark. Acta Odontol Scand 1986; 44: 343–349.
Qvist V, Thylstrup A, Mjor I A . Restorative treatment pattern and longevity of resin restorations in Denmark. Acta Odontol Scand 1986; 44: 351–356.
Rueggeberg F A, Jordan D M . Effect of light-tip distance on polymerization of resin composite. Int Dent J Prosthodont 1993; 6: 364–370.
Ryge G, Snyder M . Evaluating the clinical quality of restorations. J Am Dent Assoc 1973; 87: 369–377.
Rykke M . Dental materials for posterior restorations. Endod Dent Traumatol 1992; 8: 139–148.
Skogedal O, Heloe L A . Clinical quality of amalgam restorations. Scand J Dent Res 1979; 87: 459–461.
Smales R J . Long-term deterioration of composite resin and amalgam restorations. Oper Dent 1991; 16: 202–209.
Sturdevant J R, Lunden T F, Sluder Jr T B, Wilder A D, Taylor D F . Five-year study of two light-cured posterior composite resins. Dent Mater 1988; 4: 105–110.
Summitt J B, Osborne J W . Initial preparations for amalgam restorations: extending the longevity of the tooth-restoration unit. J Am Dent Assoc 1992; 123: 67–73.
Summitt J B, Howell M L, Burgess J O, Dutton F B, Osborne J W . Effect of grooves on resistance form of conservative class 2 amalgams. Oper Dent 1992; 17: 50–56.
Summitt J B, Osborne J W, Burgess J O . Effect of grooves on resistance/ retention form of Class 2 approximal slot amalgam restorations. Oper Dent 1993; 18: 209–213.
Taylor D F, Bayne S C, Leinfelder K F, Davis S, Koch G G . Pooling of long term clinical wear data for posterior composites. Am J Dent 1994; 7: 167–173.
Walls A W G . Glass polyalkenoate (glass ionomer) cements: a review. J Dent 1986; 14: 231–246.
Wilson N H, Wilson M A, Wastell D G, Smith G A . A clinical trial of a visible light cured posterior composite resin restorative material: five-year results. Quintessence Int 1988; 19: 675–681.
Azli N A . A systematic review of the longevity of dental restorations. MSc report. London: University of London, ('grey literature') 1998 .
NHS Centre for Reviews and Dissemination . Undertaking systematic reviews of research on effectiveness. CRD Report 4. York: University of York, 1996.
The Cochrane Collaboration . The Cochrane Collaboration Handbook, Version 4.0. Oxford: The Cochrane Collaboration, 1997.
Landis J R, Koch G G . The measurement of observer agreement for categorical data. Biometrics 1977; 33: 159–174.
SAS/Stat User's Guide — The LIFETEST procedure. Cary, N. Carolina, SAS Institute, 1994.
Meeuwissen R, van Elteren P, Eschen S, Mulder J . Durability of amalgam restorations in premolars and molars in Dutch servicemen. Community Dent Health 1985; 2: 293–302.
Djemal S, Setchell D, King P, Wickens J . Long-term survival characteristics of 832 resin-retained bridges and splints provided in a post-graduate teaching hospital between 1978 and 1993. J Oral Rehabil 1999; in press.
Downer M C, Moles D R . Health gain from restorative dental treatment evaluated by computer simulation. Community Dent Health 1998; 15: 32–39.
Author information
Authors and Affiliations
Additional information
Refereed Paper
Rights and permissions
About this article
Cite this article
Downer, M., Azli, N., Bedi, R. et al. How long do routine dental restorations last? A systematic review. Br Dent J 187, 432–439 (1999). https://doi.org/10.1038/sj.bdj.4800298a1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4800298a1
This article is cited by
-
General diseases and medications in 687 patients reporting on adverse effects from dental materials
Clinical Oral Investigations (2023)
-
Amalgam und Alternativen – Diskussionen zur Quecksilberreduktion in der Umwelt
Bundesgesundheitsblatt - Gesundheitsforschung - Gesundheitsschutz (2021)
-
A bridge too far? The relationship between interventive operative dentistry and future dental morbidity
British Dental Journal (2019)
-
Four-year outcomes of restored posterior tooth surfaces—a massive data analysis
Clinical Oral Investigations (2017)
-
A prospective 8-year follow-up of posterior resin composite restorations in permanent teeth of children and adolescents in Public Dental Health Service: reasons for replacement
Clinical Oral Investigations (2014)
