
Abstract
Objectives To compare different methods being used to determine eligibility for enhanced capitation registration payments, which were introduced in the UK in April 1998 with the intention of improving the numbers of children aged 0–5 years from deprived areas registering with General Dental Service practitioners.
Design Comparative study of the enhanced capitation registration payment schemes; data from a longitudinal study of Scottish children used to compare patient and dentist postcodes.
Outcome measures Published registration rates; levels of agreement between patient and dentist postcodes.
Results Quarterly registration rates for 3–5-year-olds show little improvement as yet; Scottish figures for 0–2-year-olds indicate a more substantial increase which may have been influenced by other initiatives. In Scotland, the degree of agreement between the deprivation scores of patient's and their dentist's postcode was less good among patients from deprived areas than for the sample as a whole.
Conclusions More detailed breakdown, using the same criteria as for the enhanced payments, may eventually offer more definitive results. Patient postcodes enable better targeting than practice postcodes, but both may omit a substantial number from the target group if area measures of deprivation are used.
Similar content being viewed by others

Main
Enhanced capitation registration payments were introduced in April 1998 for young children from deprived areas attending dentists practising within the General Dental Service (GDS) in the United Kingdom (UK). The UK Government declared that increasing payment for GDS dentists in deprived areas for seeing children less than 6 years of age would lead to more children from these communities visiting the dentist.1
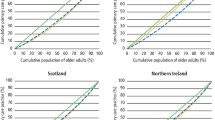
The need for initiatives directed at improving the dental health of children is well illustrated by results obtained from the annual surveys of the Scottish Health Boards' Dental Epidemiological Programme,2,3 which show a clear gradient for levels of caries experience as relative affluence decreases. The relationship holds true for different age groups. Figure 1a shows the proportion of Scottish 5-year-olds free of caries experience in 1997/982 according to the deprivation category4 of their area of residence. Figure 1b shows a similar picture for the mean number of decayed, missing and filled teeth for Scottish 12-year-olds in 1996/97.3

Percentage of Scottish 5 year olds 'free' of caries experience (d3mft = 0) by deprivation category (least deprived = 1, most deprived = 7)

Mean number of decayed, missing and filled teeth (D3MFT) for Scottish 12-year-olds by deprivation category (least deprived =1, most deprived = 7)
Aims
The choice of method of identifying the children who would attract enhanced capitation registration payments was devolved to the appropriate department in each of the four countries of the UK, in consultation with the relevant professional bodies, resulting in somewhat different approaches to this targeting. This paper compares the different approaches used, with particular reference to the use of postcodes in identifying the individuals targeted by the initiative.
There has been some debate as to whether or not the address of the dental practice attended is a satisfactory alternative to the patient's address for the identification of deprived households and their members.5 A study already underway at the Dental Health Services Research Unit at the University of Dundee, tracking a cohort of Scottish children, allowed an investigation of this issue.
Method
For the UK-wide comparative study, data on the four versions of the enhancement scheme were obtained from the relevant government departments.
For the investigation of the use of postcodes of patients and their dentists, as alternative ways of reaching children in poorer areas, the sample consisted of more than a thousand Scottish children who participated in the Children's Dental Health Survey of 1993, conducted by the Office of Population Censuses and Surveys (now the Office of National Statistics). The children were aged 5, 8, 12 and 15 years at the time of the survey. Consent to obtain subsequent dental treatment records was obtained. Data were collected for first and last attendance in the General Dental Service in the period 1993–1997.
There are various systems for categorising both individuals and regions with regard to deprivation. In Scotland, Carstairs and Morris undertook work involving the 1981 census data to produce deprivation categories for all the postcode sectors in Scotland.6 This work was updated after the 1991 census by McLoone.4 The classification uses four census variables — overcrowding, male unemployment, low social class and no car ownership — to achieve a deprivation score for each postcode sector. These scores are then assigned to deprivation categories known as DEPCATs (DEPCAT 1 for the most affluent areas to DEPCAT 7 for the most deprived areas). This categorisation has been used extensively in Scotland since the 1980s in relation to health and other issues.
For the sample of Scottish children described above, comparison was made of the deprivation category of locality of the patient's residence with the deprivation category of the locality of the dental practice visited, in order to assess the agreement between these two ways of categorising patients and, thus, their relative usefulness in the targeting of resources such as enhanced capitation registration payments. It should be emphasised that deprivation scores of the type under discussion generally refer to a district — whether an electoral ward or a postcode sector — and not to a single address. It should also be noted that this study involves older children than those currently targeted by enhanced registration payments in the GDS.
Locality of residence of the study participants was obtained from the address given on consent forms completed in 1993; information on the locality of the dental practice visited was provided by the Dental Practice Division, Edinburgh.
Results
Enhanced capitation registration payments
A comparison of the approaches taken by the four countries of the UK is shown in Table 1. The method of delivery was necessarily limited by the information that was already available, or that could be made available, for identification of the target group and that could be easily incorporated into the current payment system. It can be seen from this table that only Wales used the patient postcode as the trigger for payment in 1998/99.
Locality of residence versus locality of practice
The longitudinal study of Scottish children provided 587 first visits in the period 1993–1997 for which the required data on postcodes were available. Deprivation categories for home locality and dental practice locality were the same in the 50% of cases that make up the leading diagonal in figure 2. A further 25% of cases showed a difference of only one category. Of the 50% of cases which did not have the same value, there was almost no difference in the number of times dentist locality scored higher than patient locality and vice versa when all deprivation categories are considered. However, if one concentrates on just the most deprived localities, then a different picture emerges. For children living in areas with deprivation categories 5, 6 and 7, 52% were visiting a dentist in a more affluent locality; considering just the lowest two deprivation categories, 64% were visiting a dentist in a more affluent locality. Conversely, for dentists practising in areas with deprivation categories 5, 6 and 7, 44% of their patients came from a more affluent locality.

Deprivation categories: a comparison of locality of patient's residence with locality of dental practice attended (n = 587)
Results from last attendance in 1993–1997 gave similar results.
Monitoring the scheme
Regarding the enhanced payment scheme as currently run, quarterly registration rates should eventually indicate the extent to which the approaches used by the four countries have been successful in encouraging dental attendance.
Table 2 shows the data currently (July 1999) available. Pre-1998 quarterly rates are not included as they cannot be directly compared with later rates owing to the change in registration period to 15 months, introduced in September 1996.
Discussion
Classification systems
There are limitations in using an area classification to identify individuals. Sloggett and Joshi have estimated that 55% of the most deprived individuals in England and Wales live outside the 20% of areas that are most deprived.8 McLaren and Bain have pointed out that extrapolating these findings to Scotland would mean that half of the most deprived individuals would live in the top five deprivation category areas (ie DEPCAT 1 to 5).9 So by using area classification instead of individual classification many of the intended target group may be missed. In addition, if one also uses the area classification of the point of service rather than the place of residence, there is the obvious danger of reaching an even smaller percentage of the intended target.
The current incentive
The UK government has declared that tackling inequalities in health is a priority issue. The Departments of Health believe that, by providing what they perceive to be a financial incentive for the registration of young children from deprived areas, dental health inequality can be lessened.
This approach raises several questions:
-
Is the incentive sufficient for dentists to alter their behaviour and seek to register and re-register more of these children?
-
How will dentists identify the children in their area at whom this initiative is targeted?
-
Will the parents' actions be altered by any alterations in the dentists' behaviour?
-
Is the incentive going to the right person?
-
Will improved access lead to improved health for the target group?
The possibility exists that dentists may view the enhanced payments as merely an increase in remuneration for seeing those children that they already see and registration rates will not be altered by these enhancements.
Registration rates for 1998 and 1999
It would be unrealistic to expect substantial changes to show up in the currently available figures (Table 2), given that only England made payments from April 1998. In Scotland and Wales, the dentists were aware of the advent of the scheme and eventually received back-dated payments (see Table 1) but it is debatable how much impact the scheme would have had prior to the actual receipt of the additional payments. Future Scottish rates may be influenced by the change in April 1999 to the use of patient postcode as the trigger for the enhanced payment.
Enhanced payments may not be the only factor in any observed change in registration rates as other initiatives are known to be taking place in certain areas.10 More detailed breakdown, following a longer period of operation of the scheme and based on the criteria for enhanced payments, may offer more definitive results.
Maintenance of registration
It is known that the fairly steady registration rates observed prior to this initiative reflect a large proportion of the population dropping in and out of the system (except in the youngest age groups where, by definition, most registrations must be new ones) with just a small proportion in continuous registration and an even smaller proportion never registering.11 One way to increase the registration rates is therefore to ensure that all contracts are 'rolled-on' successfully at some time during the 15 months of each contract.
Further developments of the scheme could include:
-
Guidance on strategies for obtaining initial registrations in the target group (see, eg, Pine & Deas10)
-
Guidance on strategies for increasing the number of contracts successfully 'rolled on'
-
Incentives for the families.
Conclusion
More detailed breakdown, using the criteria for enhanced payments, may eventually offer more definitive results as to the success of the scheme as currently implemented. Further action is needed to ensure that current contracts are 'rolled-on' successfully before the end of their 15 month timespan. Guidance on local strategies for increasing registration rates and on incentives for the families should be considered in any further developments of the scheme.
For the sample of older children reviewed in this study, the deprivation category of the dental practice attended fell within one deprivation category of the patient's locality of residence for 75% of the cases examined. But this proportion fell when considering those living in the more deprived areas. For patients living in areas covered by the lowest two deprivation categories, more than 64% attended a dentist in a more affluent area.
These potential limitations in reaching the individuals who make up the targeted groups must be fully considered in both the setting up and monitoring of schemes intended to address inequalities.
References
Department of Health Press Release 98/114. One million children from deprived areas set to gain from extra £10 million NHS dentistry package. 27th March 1998.
Pitts N B, Nugent Z J, Smith P A . Scottish Health Boards' Dental Epidemiological Programme. Report of the 1997/98 Survey of 5-year-old children. Dundee: University of Dundee.
Pitts N B, Davies J A, Fyffe H E . Scottish Health Boards' Dental Epidemiological Programme. Report of the 1996/97 survey of 12-year-old children. Dundee: University of Dundee.
McLoone P . Carstairs scores for Scottish postcode sectors from the 1991 census. Glasgow: University of Glasgow, 1994.
Monaghan N, Heesterman R . Dental caries, social deprivation and enhanced capitation payments for children. Br Dent J 1999; 186: 238–240.
Carstairs V, Morris R . Deprivation and health in Scotland. Aberdeen: Aberdeen University Press, 1991.
GDS quarterly statistics. Registrations: England and Wales. Dental Practice Board, Eastbourne, 1998 and 1999.
Sloggett A, Joshi H . Higher mortality in deprived areas: community or personal disadvantage? Br Med J 1994; 309: 1470–1474.
McLaren G, Bain M . Deprivation and health in Scotland. Insights from NHS data. Edinburgh: Information and Statistics Division, National Health Service in Scotland, 1998.
Pine C M, Deas J M . A Primary Care Initiative to Increase Infant NHS Dental Registrations. J Dent Res 1997; 76: 1020.
Davies J A . Registration of children in the General Dental Service in Scotland — is continuity of care being achieved?. Community Dent Health 1997; 14: 119.
Acknowledgements
Funded by the Scottish Executive Health Department. The views expressed are those of the author and are not necessarily shared by the Scottish Executive.
Author information
Authors and Affiliations
Additional information
Refereed Paper
Rights and permissions
About this article
Cite this article
Davies, J. Enhancing dental attendance rates for children from deprived areas in the UK. Br Dent J 187, 323–326 (1999). https://doi.org/10.1038/sj.bdj.4800270
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4800270
This article is cited by
-
Evaluating “Starting Well,” the Scottish National Demonstration Project for Child Health: Outcomes at Six Months
The Journal of Primary Prevention (2005)
-
Capitation registration and social deprivation in England. An inverse 'dental' care law?
British Dental Journal (2001)
-
The role of team dentistry in improving access to dental care in the UK
British Dental Journal (2001)
