
Abstract
Cytokeratin 7 (CK 7) and cytokeratin 20 (CK 20) are low molecular weight cytokeratins. Their anatomic distribution is generally restricted to epithelia and their neoplasms. We surveyed 435 epithelial neoplasms from various organ systems by immunohistochemistry using CK 7 and CK 20 monoclonal antibodies. Expression of CK 7 was seen in the majority of cases of carcinoma, with the exception of those carcinomas arising from the colon, prostate, kidney, and thymus; carcinoid tumors of the lung and gastrointestinal tract origin; and Merkel cell tumor of the skin. The majority of cases of squamous cell carcinoma of various origins were negative for CK 7, except cervical squamous cell carcinoma, in which 87% of cases were positive. Approximately two thirds of cases of malignant mesothelioma were CK 7-positive. CK 20 positivity was seen in virtually all cases of colorectal carcinomas and Merkel cell tumors. CK 20-positive staining was also observed in cases of pancreatic carcinomas (62%), gastric carcinoma (50%), cholangiocarcinomas (43%), and transitional cell carcinomas (29%). The expression of CK 20 was virtually absent in carcinomas from other organ systems and in malignant mesothelioma. CK 7- and CK 20-negative epithelial neoplasms included adrenal cortical carcinoma, germ cell tumor, prostate carcinoma, renal cell carcinoma, and hepatocellular carcinoma.
Similar content being viewed by others


INTRODUCTION
The most common malignancies are derived from simple epithelia of the breast, lung, colon, prostate, ovaries, and endometrium. Carcinomas from these sites usually metastasize to regional lymph nodes and other organs, such as lung, brain, liver, and bone. The diagnosis of the metastatic carcinoma of unknown origin can be very difficult. The determination of the primary site of the metastasis is a challenge to both oncologists and pathologists, having potentially important clinical and therapeutic consequences.
Many tumor markers have been developed in the past two decades as immunohistochemical aids to the diagnosis of carcinoma. Some of these tumor markers, such as prostate specific antigen (PSA), are very organ specific. Others, such as carcinoembryonic antigen (CEA) and epithelial membrane antigen (EMA), although widely used, lack organ specificity. Although the expression of cytokeratins (CKs) is generally confined to epithelia and their neoplasms (1, 2, 3, 4, 5, 6), they are not specific tumor markers. However, the highly diverse expression patterns of CKs have been correlated with different pathways of epithelial differentiation, and thereby allow the accurate and sophisticated classification of epithelial cells into different subtypes (1, 7, 8). During cell transformation and tumor development, this cell type specificity of cytokeratins is largely conserved (4, 9).
The diverse and unique expression of CK 7 and CK 20 in carcinomas has been found to be useful in the differential diagnosis of some carcinomas of epithelial origin (10, 11). Studies have shown that the different expression patterns of CK 7 and CK 20 are among the most discriminant markers in: (1) the differential diagnosis between metastatic colon and ovarian adenocarcinomas (7, 10, 12, 13, 14, 15, 16, 17); (2) the differential diagnosis between Merkel cell tumor of skin and small cell carcinomas of other origins (7, 11, 18, 19, 20, 21); and (3) the differential diagnosis between lung, endometrial, and breast adenocarcinomas and colon adenocarcinoma (20, 22). Studies of CK 7 and CK 20 expression in other epithelial carcinomas have also been explored in the past ten years (11, 20, 21, 22). However, most of these studies have either involved few cases or studied limited organ systems. One relatively comprehensive study has been reported, but the reproductivity of these findings has not been confirmed in other laboratories, and even a previous large study only studied a limited number of organ systems (16).
MATERIALS AND METHODS
Cases
Four hundred thirty-five cases of carcinomas from different organs were selected from our surgical pathology files. Of 26 cases of breast adenocarcinomas, 20 cases were ductal and six were lobular carcinomas. Of 24 cases of ovarian adenocarcinomas, 12 were serous papillary, four were clear cell, and eight were endometrioid. Of 55 cases of thyroid tumors, 24 were adenomas, 16 were medullary carcinomas, five were follicular carcinomas, and 10 were papillary carcinomas. Of 10 cases of salivary gland tumors, five were mixed tumors, two were Warthin’s tumors, and two were mucoepidermoid carcinomas. Of 14 cases of germ cell tumors, six were embryonal carcinomas, four were seminomas, three were teratomas, and one was a yolk sac tumor. The diagnoses were reconfirmed; only cases of primary carcinoma were used. All tissues had been fixed in 10% neutral formalin and embedded in paraffin. The organ origins of carcinomas are listed in Tables 1 and 2.
Immunohistochemistry
Commercially available CK 7 (clone OV-TL-12/30) and CK 20 (clone IT-Ks 20.8) antibodies were purchased from DAKO (DAKO Corporation, Carpinteria, CA) and ARP (American Research Products, Inc., Belmont, MA), respectively. These two clones were selected because they have been used in our immunohistochemistry lab with better results in comparison to other commercially available keratin 7 and keratin 20 clones. Serial 5-μm sections were cut from each case. The sections were deparaffinized and rehydrated in graded alcohol. For heat-induced epitope retrieval (HIER), the sections were subjected into 100-mm EDTA buffer (pH 8.0) in a Steamer (Black & Decker, Shelton, CT) at 100° C for 20 min. The sections were then brought to an automated stainer (TechMate, Tucson, AZ), following the vendor’s protocol. Two sections were stained with CK 7 (1:200) and 20 (prediluted by vendor). Avidin-biotin complex (ABC) and peroxidase methods were used.
Cytoplasmic immunoreactivity was assessed. Only those cases showing greater than 5% tumor cell positivity were regarded as positive.
RESULTS
CK 7 in Epithelial Neoplasms
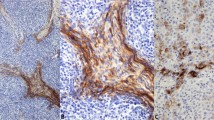
The frequency of CK 7 expression is summarized in Table 1. CK 7 positivity was generally diffuse and cytoplasmic. The vast majority of cases of adenocarcinomas were positive for CK 7, including lung (100%), ovary (100%), uterus (100%), breast (96%) (Fig. 1A), salivary gland (100%), thyroid neoplasms (100%), cholangiocarcinoma (93%), pancreas (92%), and transitional cell carcinoma (88%). In contrast, only a small percentage of cases of adenocarcinoma of colon (5%), stomach (28%), and kidney (11%) were CK 7-positive. Squamous cell carcinoma of the cervix was positive in 87% of cases (Fig. 1B). In contrast, squamous cell carcinoma of the head and neck (27%) and esophagus (21%) were positive in a minority of cases; and squamous cell carcinoma of the lung (0%) was negative in all cases. Malignant mesothelioma was positive in 65% of cases. Of neuroendocrine neoplasms, about one-half of cases of small cell carcinoma of the lung (56%) and neuroendocrine carcinomas from a variety of sites (43%) were positive for CK 7, a minority of cases of carcinoid tumor (22%) were positive, and Merkel cell tumor of skin (0%) was entirely negative. Other neoplasms that were rarely or never CK 7-positive included hepatocellular carcinoma (9%), germ cell tumor (7%), adrenal cortical carcinoma (0%), prostate adenocarcinoma (0%), thymoma (0%), and epithelioid sarcoma (0%).

Pagetoid cells in breast nipple (A) and a case of moderately differentiated cervical squamous cell carcinoma (B) are strongly cytoplasmic positive for CK 7. Note the negative staining in the non-neoplastic epithelium (A).
CK 20 in Epithelial Neoplasms
The frequency of CK 20 expression is summarized in Table 2. In Merkel cell tumor, CK 20 positivity was dot-like cytoplasmic, whereas in other neoplasms, CK 20 positivity was diffuse cytoplasmic. Unlike CK 7, CK 20 expression was restricted to a few organ systems. All cases of colon carcinoma were positive for CK 20 as were most cases of Merkel cell tumor of skin (78%) and adenocarcinoma of the pancreas (62%). One-half of cases of adenocarcinoma of the stomach were CK 20-positive, as were a subset of cases of cholangiocarcinoma of the liver (43%) and transitional cell carcinoma of the bladder (29%). All other neoplasms studied were rarely or never positive for CK 20.
Correlation of CK 7 and CK 20 Expression Patterns in Different Epithelial Neoplasms
The correlation of CK 7 and CK 20 expression in epithelial neoplasms is summarized in Table 3.
CK 7+/CK 20+ epithelial neoplasms
The majority of cases in this category were carcinomas from the gastrointestinal and genitourinary tracts. Sixty-two percent of cases of pancreatic carcinoma (Fig. 2,A-B), 43% of cases of cholangiocarcinoma (Fig. 2, C-D), 25% of cases of bladder transitional cell carcinoma (Fig. 2, E-F), and 13% of cases of gastric carcinoma were CK 7+/CK 20+. The positive cells in CK 7+/CK 20+ tumors were often overlapping (Fig. 2).

CK 7+/CK 20+ coexpression in a case of pancreatic carcinoma (A, B, respectively), a case of cholangiocarcinoma (C, D, respectively) and a case of transitional cell carcinoma (E, F, respectively). The CK 7 and CK 20 cytoplasmic positive immunostaining results were taken from the same field.
CK 7+/CK 20− carcinomas
Virtually all cases of breast (96%) (Fig. 3, A-B), ovarian adenocarcinoma (96%) (endometrioid, serous papillary and clear cell subtypes) (Fig. 3, C-D); lung (90%) (Fig. 3, E-F), endometrial (100%) (Fig. 3, G-H), and thyroid tumors (98%) (follicular, papillary, and medullary subtypes); and salivary gland tumors (100%) were CK 7+/CK 20−. In addition, approximately two-thirds (65%) of cases of malignant mesothelioma were also CK 7+/CK 20−.

CK 7+/CK 20- immunostain in a case of breast ductal carcinoma (A, B, respectively), a case of ovarian carcinoma (C, D, respectively), a case of lung adenocarcinoma (E, F, respectively), and a case endometrial adenocarcinoma (G, H, respectively). The CK 7 and CK 20 immunostaining results were taken from the same field.
CK 7−/CK 20+ carcinomas
Virtually all cases (95%) of colorectal carcinoma (Fig. 4, A-B), 78% of cases of Merkel cell tumor of skin (Fig. 4, C-D), and 37% of cases of gastric adenocarcinoma were CK 7/CK 20+. The CK 20-positive staining pattern in Merkel cell carcinoma was cytoplasmic dot-like, which was different from that seen in cases of CK 20-positive gastric and colorectal carcinoma (diffuse cytoplasmic staining).

CK 7-/CK 20+ in a case of colon adenocarcinoma (A, B, respectively), and a case of Merkel cell tumor of skin (C, D, respectively). The CK 7 and CK 20 immunostaining results were taken from the same field. Note the CK 20 cytoplasmic dot-like staining pattern (D).
CK 7−/CK 20− carcinomas
All cases of adrenal cortical carcinomas, prostatic carcinomas, thymomas, and epithelial sarcomas were CK 7/CK 20−. In addition, the majority of cases of hepatocellular carcinomas (9/11), carcinoid tumors of lung (7/9) and gastrointestinal tract (12/15), and renal cell carcinomas (17/19) were also CK 7−/CK 20−.
DISCUSSION
It is often important to determine the site of origin of a metastatic carcinoma of unknown primary site, particularly because this may affect the choice of the treatment. Determination of the primary site may take several steps. Clinical features, such as age, sex, and site of metastases may give a first indication. The histologic assessment is often very helpful, but may not differentiate adequately between various primary tumors. Immunohistochemical staining may provide a third level of data.
Intermediate filaments (7 to 11 nm) are major cytoskeletal proteins in eukaryotic cells. Unlike actin-biding microfilaments and tubulin-containing microtubules of the cytoskeleton family, the five types of intermediate filaments show some specificity in both normal tissue (4) as well as their neoplasms (23, 24). Therefore, immunohistochemistry of intermediate filaments is widely used in surgical pathology for differential diagnosis of sarcomas (vimentin), including rhabdomyosarcomas (desmin), carcinomas (cytokeratins), nervous tissue tumors (neurofilament), and gliomas (glial fibrillary acid protein). Carcinomas are a diverse group of neoplasms, and so are the cytokeratins found in these carcinomas. In the past 20 years, we have gained tremendous knowledge, both in cytokeratin biology and their distribution in normal tissue, as well as in applications in diagnostic surgical pathology. CK 7 and 20 are two of the most commonly used CKs in surgical pathology (12, 16, 17).
For comparison, the results of the current study and that of Wang, et al. (16) are summarized in Table 3. One must note that the cut-off percentage of staining for a positive result is different between the current study (5%) and that used by Wang et al. (1%), which in part may contribute to differences in the results in some groups of carcinomas between the two studies. We concur with others (17) that a 5% cut-off percentage for positivity may eliminate more “false positive” results than a 1% cut-off. In addition, the CK 20 monoclonal antibody used in the current study (American Research Products [APR], Inc., Belmont, MA) was different from that used by Wang et al. (16) (DAKO). We did a pilot comparison study of several different commercially available CK 20 antibodies, and found that the CK 20 antibody from ARP gave the best results in our laboratory. Nonetheless, our results are similar to that of Wang et al. for most major categories of carcinomas. One notable difference, however, was a much lower incidence of CK 20 positivity in transitional cell carcinoma of the bladder, 29% versus 89% in the series of Wang et al. We found that well differentiated transitional cell carcinomas were more likely to be CK 20 positive than poorly differentiated transitional cell carcinomas; thus, the difference in CK 20 expression in the present study and that of Wang et al. may be due to the selection of cases of different degrees of differentiation.
In the absence of results of other markers, the demonstration of CK 7 positivity alone has limited value in differential diagnosis of metastatic carcinoma (11). Its expression is often seen in the major categories of adenocarcinoma, including adenocarcinoma of the breast, lung, ovary, endometrium, thyroid, salivary gland, pancreas, and bile duct (21, 25, 26). However, there are circumstances in which the determination of CK 7 positivity is useful. We agree with Ramaekers et al. (11) that CK 7 immunostaining can be extremely useful when the differential diagnosis between a prostatic carcinoma and a transitional cell carcinoma of prostate or other genitourinary organs is an issue. In the current study, all cases (0/18) of prostatic carcinoma were CK 7-negative, whereas the majority of cases (21/24) of transitional cell carcinoma were CK 7-positive. CK 7 has been regarded as “bile duct keratin” because it only stains bile ducts in normal liver (27, 28). The current study showed that the majority of cases of cholangiocarcinoma (13/14) were CK-7 positive; whereas majority cases of hepatocellular carcinoma (1/11) were CK 7-negative. These results are similar to those of Maeda et al. (29) who found that over 97% of cholangiocarcinoma, whereas only 7% of hepatocellular carcinomas, were CK 7-positive. Therefore, the expression of CK 7 also can be useful in the differential diagnosis of a cholangiocarcinoma versus hepatocellular carcinoma. The further demonstration of CK 20 positivity may provide additional evidence favoring a cholangiocarcinoma, as 43% of these cases are positive for CK 20 versus 9% of cases of hepatocellular carcinoma.
CK 7 is also a very specific marker for mammary and extramammary Paget’s disease (30, 31). After comparing various markers (CK 7, CAM 5.2, CK 20, CEA, Ber-EP4), Smith et al. (32) concluded that CK 7 is the only marker exhibiting strong and specific staining within the epidermis in all cases of breast Paget’s disease. The current study further supports the conclusion made by Smith et al. (32). However, in some cases of perianal Paget’s disease associated with colorectal adenocarcinoma, the pagetoid cells are often CK 7+/CK 20+ or CK 7-/CK 20+ (33, 34).
The finding of CK 7 negativity has greater diag-nostic value (11). When a carcinoma is CK 7-negative, the differential diagnosis should include prostate, renal cell, neuroendocrine, hepatocellular, and adrenal carcinomas, carcinoid tumors, germ cell tumors, and squamous cell carcinomas of various origins with exception of cervical squamous cell carcinoma. These tumors may be distinguished by adding other markers, such as prostate specific antigen (prostate carcinoma), chromogranin (neuroendocrine carcinoma), bile-duct specific CEA or alpha-fetoprotein (hepatocellular carcinoma) and keratin AE-1 (negative in adrenocortical carcinoma), or vimentin (renal cell carcinoma).
The majority of cases of squamous cell carcinoma of various origins are CK 7-/CK 20-. However, when a squamous cell carcinoma is CK 7-positive, squamous cell carcinoma of the uterine cervix should be considered. Normal ectocervical squamous mucosa lacks CK 7 positivity (35). However, dysplastic cervical epithelium and squamous cell carcinoma in situ tends to express CK 7. We found that the majority of cases of cervical squamous cell carcinomas (13/15) were CK 7-positive, whereas the CK 7-positive rate of squamous cell carcinoma of other origins was much lower (20 to 30%).
CK 20 positivity is seen in the majority of cases of colorectal adenocarcinoma (5, 10, 17), and over one-third of cases of gastric adenocarcinoma. However, unlike regular colonic adenocarcinoma, rectal adenocarcinoma de novo is CK 7+/CK 20+ or CK 7+/CK 20- (33, 34). CK 20-positivity in carcinomas with neuroendocrine features is primarily seen in Merkel cell tumor (10, 18), as other small cell tumors, neuroendocrine carcinoma of various origins, and carcinoid tumors of gastrointestinal tract and lung are usually negative for CK 20 (Table 2). The cytoplasmic dot-like CK 20 positivity is very specific to Merkel cell tumor and is not seen in other common CK 20-positive carcinomas, such as colorectal adenocarcinoma.
CK 7 and CK 20 antibodies are best used together in the differential diagnosis of a poorly differentiated carcinoma (13, 17). When a carcinoma is CK 7+/CK 20+, the differential diagnosis should include pancreatic carcinoma, cholangiocarcinoma, transitional cell carcinoma, and intestinal-type sinonasal adenocarcinoma (36). However, not all these carcinomas are CK 20-positive. The current study, as well as several other studies, showed that approximately one-third of pancreatic adenocarcinoma are CK 20-negative (5, 16, 22). For a metastatic adenocarcinoma in which the differential diagnosis is colorectal versus ovarian (12, 14, 17, 20), breast (22), endometrial (37), or lung (20) adenocarcinoma, CK 7 and CK 20 are the most useful markers. Over 90% of colonic adenocarcinomas are CK 7-/CK 20+ (Table 4), whereas over 90% of ovarian adenocarcinomas, and over 80% of endometrial, breast, and lung adenocarcinomas are CK 7+/CK 20-. However, it should be kept in mind that ovarian mucinous tumors have a high CK 20-positive rate (14, 16, 17). Mucinous tumors of ovarian, pancreatic, or gastrointestinal tract origins were not specifically examined in the current study.
References
Cooper DS, Schermer A, Sun TT . Classification of human epithelia and their neoplasms using monoclonal antibodies to keratins: strategies, applications, and limitations. Lab Invest 1985; 52: 243–256.
Gown AM, Vogel AM . Monoclonal antibodies to human intermediate filament proteins. II. Distribution of filament proteins in normal human tissues. Am J Pathol 1984; 114: 309–321.
Gown AM, Vogel AM . Monoclonal antibodies to human intermediate filament proteins. III. Analysis of tumors. Am J Clin Pathol 1985; 84: 413–424.
Hynes RO, Destree AT . 10 nm filaments in normal and transformed cells. Cell 1978; 13: 151–163.
Moll R . Cytokeratins as markers of differentiation in the diagnosis of epithelial tumors. Subcellular Biochem 1998; 31: 205–261.
Moll R, Franke WW, Schiller DL, Geiger B, Krepler R . The catalog of human cytokeratins: pattern of expression in normal epithelia, tumor and culture cells. Cell 1982; 31: 11–24.
Moll R, Lowe A, Laufer J, Franke WW . Cytokeratin 20 in human carcinomas. A new histodiagnostic marker detected by monoclonal antibodies. Am J Pathol 1992; 140: 427–447.
Wu YJ, Rheinwald JG . A new small (40 kd) keratin filament protein made by some cultured human squamous cell carcinomas. Cell 1981; 25: 627–635.
Sun TT, Skelton HG, Green H . Keratin cytoskeletons in epithelial cells of internal organs. Proc Nat Acad Sci U S A 1979; 76: 2813–2817.
Miettinen M . Keratin 20: immunohistochemical marker for gastrointestinal, urothelial, and Merkel cell carcinoma. Mod Pathol 1995; 8: 384–388.
Ramaekers FC, van Niekerk CC, Poels LG, Schaafsma E, Huijsmans A, Robben H, et al. Use of monoclonal antibodies to keratin 7 in the differential diagnosis of adenocarcinomas. Am J Pathol 1990; 136: 641–655.
Berezowski K, Stastny JF, Kornstein MJ . Cytokeratin 7 and 20 and carcinoembryonic antigen in ovarian and colonic carcinoma. Mod Pathol 1996; 9: 426–429.
Lagendijk JH, Mullink H, van Diest PJ, Meijer GA, Meijer CJLM . Tracing, the origin of adenocarcinomas with unknown primary using immunohistochemistry: differential diagnosis between colonic and ovarian carcinomas as primary sites. Hum Pathol 1997; 29: 491–497.
Loy TS, Calaluce RD, Keeney GL . Cytokeratin immunostaining in differentiating primary ovarian carcinoma from metastatic colonic adenocarcinoma. Mod Pathol 1996; 9: 1040–1044.
Ueda G, Sawada M, Ogawa H, Tanizawa O, Tsjimoto M . Immunohistochemical study of cytokeratin 7 for the differential diagnosis of adenocarcinomas in the ovary. Gynecol Oncol 1993; 51: 219–223.
Wang NP, Zee S, Zarbo RJ, Bacchi CE, Gown AM . Coordinate expression of cytokeratins 7 and 20 defines unique subsets of carcinomas. Appl Immunohistochem 1995; 3: 99–107.
Wauters CC, Smedts F, Gerrits LG, Bosman FT, Ramaekers FC . Keratin 7 and 20 as diagnostic markers of carcinomas metastatic to the ovary. Hum Pathol 1995; 26: 852–855.
Chan JKC, Wenig BM, Tsang WYW, Chan JBK, Lau LW . Cytokeratin 20 immunoreactivity distinguishes Merkel cell (primary cutaneous neuroendocrine) carcinomas and salivary gland small cell carcinomas from small cell carcinomas of various sites. Am J Surg Pathol 1997; 21: 226–234.
Jarasch ED, Nagle RB, Kaufmann M, Maurer C, Bocker WJ . Differential diagnosis of benign epithelial proliferations and carcinomas of the breast using antibodies to cytokeratins. Hum Pathol 1988; 19: 276–289.
Loy TS, Calaluce RD . Utility of cytokeratin immunostaining in separating pulmonary adenocarcinomas from colonic adenocarcinomas. Am J Clin Pathol 1994; 102: 764–767.
van de Molengraft FJJM, van Niekerk CC, Jap PH, Poels LG . OV-TL 12/30 (keratin 7 antibody) is a marker of glandular differentiation in lung cancer. Histopathology 1993; 22: 35–38.
Kaufmann O, Deidesheimer T, Muehlenberg M, Deicke P, Dietel M . Immunohistochemical differentiation of metastatic breast carcinomas from metastatic adenocarcinomas of other common primary sites. Histopathology 1996; 29: 233–240.
Osborn M, Weber K . Intermediate filaments: cell-type-specific markers in differentiation and pathology. Cell 1982; 31: 303–306.
Osborn M, Weber K . Tumor diagnosis by intermediate filament typing: a novel tool for surgical pathology. Lab Invest 1983; 48: 372–394.
Baars JH, De-Ruijter JLM, Smedts F, van Niekerk CC, Poels LG, Seldenrijk CA, et al. The applicability of a keratin 7 monoclonal antibody in routinely Papanicolaou-stained cytologic specimens for the differential diagnosis of carcinomas. Am J Clin Pathol 1994; 101: 257–261.
van Niekerk CC, Jap PHK, Ramaekers FC, van de Molengraft F, Poels LG . Immunohistochemical demonstration of keratin 7 in routinely fixed paraffin-embedded human tissues. J Pathol 1991; 165: 145–152.
Rubio CA . The detection of bile ducts in liver biopsies by cytokeratin 7. In Vivo 1998; 12: 183–186.
West AB, Chatila R . Differential diagnosis of bile duct injury and ductopenia. Semin Diagn Pathol 1998; 15: 270–284.
Maeda T, Adachi E, Kajiyama K, Sugimachi K, Tsuneyishi M . Combined hepatocellular and cholangiocarcinoma: proposed criteria according to cytokeratin expression and analysis of clinicopathologic features. Hum Pathol 1995; 26: 956–964.
Lundquist K, Kohler S, Rouse RV . Intraepidermal cytokeratin 7 expression is not restricted to Paget cells but is also seen in Toker cells and Merkel cells. Am J Surg Pathol 1999; 23: 212–219.
Goldblum JR, Hart WR . Vulvar Paget’s disease: a clinicopathologic and immunohistochemical study of 19 cases. Am J Surg Pathol 1997; 21: 1178–1187.
Smith KJ, Tuur S, Corvette D, Lupton GP, Skelton HG . Cytokeratin 7 staining in mammary and extramammary Paget’s disease. Mod Pathol 1997; 10: 1069–1074.
Ashraf M, Zhang PJ . Cytokeratin (CK) 7 expression in rectal adenocarcinoma [abstract]. Mod Pathol 1999; 12: 187A.
Goldblum JR, Hart WR . Perianal Paget’s disease: a histologic and immunohistochemical study of 11 cases with and without associated rectal adenocarcinoma. Am J Surg Pathol 1998; 22: 170–179.
Smedts F, Ramaekers FC, Vooijs P . The dynamics of keratin expression in malignant transformation of cervical epithelium: a review. Obstet Gynecol 1993; 82: 465–474.
Krane JF, O’Connell JT, Pilch BZ, Faquin WC . Cytokeratin and mucin expression in intestinal-type sinonasal adenocarcinomas [abstract]. Mod Pathol 2000; 13: 139A.
Zemer R, Fishman A, Bernheim J, Zimlichman S, Markowicz O, Altaras M, et al. Expression of cytokeratin-20 in endometrial carcinoma. Gynecol Oncol 1998; 70: 410–413.
Brinkschmidt C, Stolze P, Fahrenkamp AG . Immunohistochemical demonstration of chromogranin A, chromogranin B, and secretoneum in Merkel cell carcinoma of the skin, an immunohistochemical study of 18 cases suggesting two types of Merkel cell carcinoma. Appl Immunohistochem 1995; 3: 37–44.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Chu, P., Wu, E. & Weiss, L. Cytokeratin 7 and Cytokeratin 20 Expression in Epithelial Neoplasms: A Survey of 435 Cases. Mod Pathol 13, 962–972 (2000). https://doi.org/10.1038/modpathol.3880175
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/modpathol.3880175
Keywords
This article is cited by
-
A review of 14 cases of perianal Paget’s disease: characteristics of anorectal cancer with pagetoid spread
World Journal of Surgical Oncology (2023)
-
Carcinoma of unknown primary (CUP): an update for histopathologists
Cancer and Metastasis Reviews (2023)
-
Identification of the most specific markers to differentiate primary pulmonary carcinoma from metastatic gastrointestinal carcinoma to the lung
Diagnostic Pathology (2022)
-
Literature review of imaging, pathological diagnosis, and outcomes of metachronous lung and pancreatic metastasis of cecal cancer
World Journal of Surgical Oncology (2022)
