
Abstract
Well-differentiated encapsulated tumors of the thyroid gland with a follicular architecture may cause diagnostic difficulties. Questionable vascular or capsular penetration may raise the possibility of a follicular carcinoma, while focal nuclear clearing and grooves may suggest a diagnosis of papillary carcinoma. A proposal has recently been made to designate cases showing suggestive but not conclusive morphological evidence of malignancy along these lines as well-differentiated or follicular tumors of uncertain malignant potential. The aim of the present study was to investigate the expression and diagnostic role in well-differentiated or follicular tumors of uncertain malignant potential of Galectin-3 and HBME-1, two malignancy-related markers. A total of 21 tumors fulfilling the criteria of well-differentiated or follicular tumors of uncertain malignant potential were collected from two institutions, including eight cases with questionable vascular and/or capsular invasion and 13 cases with some degree of nuclear changes in the form of clearing, grooves, and/or pseudoinclusions. Tumors in the first group expressed HBME-1 and Galectin-3 focally (less than 25% of tumor cells) in 5/8 and 3/8 cases, respectively, with 62.5% of cases reacting for at least one marker. Cases in the second category expressed HBME-1 and Galectin-3 in 9/13 and 10/13 cases, respectively, with 92.3% of cases having at least one marker expressed. These findings indicate that HBME-1 and Galectin-3 are heterogeneously distributed in these borderline tumors, but that a strong and diffuse expression of HBME-1 and to a lower extent of Galectin-3 was preferentially observed in the group characterized by nuclear changes which were similar but less developed than those of conventional papillary carcinoma. The relationship found between the markers investigated and these nuclear changes suggests that the tumors containing them are pathogenetically linked to papillary carcinomas.
Similar content being viewed by others

Main
Well-differentiated encapsulated tumors of the thyroid gland with a follicular architecture may cause diagnostic difficulties due to the presence of incomplete or equivocal capsular penetration—which may induce the suspicion of follicular carcinoma—or the occurrence of focal nuclear changes such as clearing, overlapping, grooves and pseudoinclusions, which may raise the possibility of the follicular variant of papillary carcinoma. Depending on the severity of these changes and the bias of the observer, terms such as atypical adenoma, ‘hybrid’ carcinoma, and—more recently—well-differentiated carcinoma not otherwise specified were proposed.1, 2, 3, 4, 5 In a recent editorial from the Chernobyl Pathologists Group the suggestion was made to label tumors with ‘borderline’ features as well-differentiated tumor of uncertain malignant potential (WDT-UMP) in the presence of questionable papillary carcinoma-type nuclear changes with or without questionable capsular penetration, or follicular tumor of uncertain malignant potential (FT-UMP) in the presence of questionable capsular penetration without nuclear changes.6, 7
Several immunocytochemical markers of malignancy have been claimed to be useful to distinguish follicular adenoma from carcinoma and also to identify papillary carcinoma and its variants, both in surgical and cytological specimens. These include Galectin-3,8, 9, 10, 11, 12 HBME-1,12, 13, 14, 15 cytokeratin 19,15, 16, 17, 18 thyroperoxidase,19 and high mobility group (HMG)-Y proteins.20
Galectin-3 is a member of a family of β-galactoside binding animal lectins. This protein is expressed in many tissues and cells at both nuclear and cytoplasmic levels and has multiple functions, including cell–cell and cell–matrix adhesion, cell growth, neoplastic transformation and spread, cell cycle regulation and apoptosis, and cell repair processes. Galectin-3 has been found to be increased in several human malignant tumors, including well-differentiated follicular-derived thyroid carcinomas.10 HBME-1 was originally described as a marker of normal and malignant mesothelial cells, since it recognizes a currently unknown antigen expressed by those cells. It was later shown to also stain most papillary thyroid carcinomas, and also a fraction of follicular carcinomas, while adenomas are generally negative.12, 13, 14, 15 In a recent study on oxyphilic tumors of the thyroid,21 Galectin-3 and HBME-1 expression were found to be related to molecular alterations such as PAX8-PPARgamma translocations22 and ras oncogene mutations.
The aim of the present study was to investigate the expression and the possible diagnostic role of these two markers in a series of well-differentiated thyroid neoplasms with a follicular architecture that fulfilled the criteria for WDT-UMP or FT-UMP, as proposed by Williams et al.6
Materials and methods
Tissues
In all, 21 cases of thyroid tumors of follicular origin and categorized as WDT-UMP or FT-UMP were collected from the consultation files of one of us (JR) or the files of the Department of Pathology of the National Cancer Institute of Milan (14 cases) (years 1996–2003), and the files of the Pathology Department of the University of Turin (seven cases) (years 2001–2003). The diagnosis was based on the proposed criteria for these tumors.6 In particular, WDT-UMP was represented by an encapsulated tumor composed of follicular cells having incompletely developed papillary carcinoma-type nuclear changes. In these tumors, no blood vessel invasion was present, while capsular penetration was either absent or questionable. FT-UMP was defined as an encapsulated tumor with follicular architecture, composed of conventional or oxyphilic cells, and having incomplete or questionable capsular penetration, but neither vascular invasion nor papillary carcinoma-type nuclear changes. Based on these criteria, 13 cases qualified as WDT-UMP (one of these was a small nodule in the context of Hashimoto's thyroiditis) and eight as FT-UMP. In all, 14 cases of follicular variant of papillary carcinoma and 15 follicular adenomas were collected from the same Institutions and served as control groups. All cases had hematoxylin & eosin (H&E) stains available for review and paraffin blocks for immunohistochemical stainings.
Immunohistochemistry
A purified monoclonal antibody to Galectin-3 was used at the dilution of 1/200, as previously described.9 This monoclonal is now commercially available (Mabtech, Naka, Sweden). HBME-1 antibody was purchased from DakoCytomation (Glostrup, Denmark) and used at the dilution of 1/50. Both markers were revealed with a biotin-free immunoperoxidase procedure23 (EnVision, DakoCytomation), preceded by heat-induced antigen retrieval (three 3-min microwave oven passages at 750 W in citrate buffer). Positive controls for immunohistochemistry were a papillary thyroid carcinoma for Galectin-3 and a pleural mesothelioma for HBME-1. Macrophages at the periphery of goiter nodules and endothelial cells served as positive internal controls in most cases. The immunoreactivity was scored as negative, focally positive (+: less than 25%), positive (++: 25–50%) or diffusely positive (+++: more than 75%), based on the extent of the reaction. A case was scored as positive only when strong signals in the cytoplasm or along the cell membrane were detected for Galectin-3 and HBME-1, respectively.
Results
The clinicopathological and immunohistochemical data on all the cases studied are summarized in Table 1. All but two of the patients were females, with a median age of 47 years. Follow-up information were available for seven cases only (nos. 15–21): all patients are currently alive and well 1–3 years after operation. The eight cases of FT-UMP were characterized by one or several areas of irregular capsular profile, with initial penetration by tumor which never reached full thickness. Two additional cases had similar features in the capsule, but also had areas with papillary carcinoma-type nuclei. The latter were the only abnormalities present in the other 11 cases, in which the capsule was intact. Four cases (three FT-UMP and one WDT-UMP nos. 6, 7, 8, 19) had oxyphilic cytoplasmic changes in more than 75% of the tumor cells.
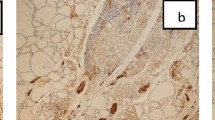
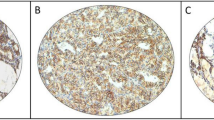
The immunohistochemical pattern of Galectin-3 and HBME-1 was slightly different among the two groups of tumors. The FT-UMP group showed Galectin-3 immunoreactivity in 3/8 cases, the reaction being usually restricted to single cells or in any case to less than 25% of the tumor cell population. HBME-1 was present in 5/8 cases, again generally limited to single cells (three cases) or present in less than 50% of the tumor in the remaining two cases (Figure 1). Overall, five cases focally expressed at least one marker (62.5%), and three cases were negative for both markers. The cases of WDT-UMP having papillary carcinoma-type nuclei expressed either Galectin-3 or HBME-1 in all but one (no. 13) cases (92.3%) (Figure 2). HBME-1 was present in 9/13 tumors and was more extensively expressed (three cases had more than 75% of the tumor area positive). Galectin-3 was expressed in 10/13 tumors, generally in less than 25% of the tumor area (two cases only showed a much wider immunoreactivity in approximately 50% of the tumor cell population).

Encapsulated follicular tumor of uncertain malignant potential (case 10). Irregular capsular profile and incomplete capsular penetration is observed (a, b). In this subcapsular area, small uniform follicles are present (c, d) and contain thyrocytes with occasional clear, ground-glass nuclei (e) and pseudoinclusions (f). These follicles are unreactive for Galectin-3 (g) and positive for HBME-1 (h). (a: H&E, × 40; b: H&E, × 100; c, d: H&E, × 320; e, f: H&E, × 1000; g, h: immunoperoxidase, × 320).

Well-differentiated tumors of uncertain malignant potential (WDT-UMP). In this well-demarcated follicular tumor (a, case 19), several follicles contain irregular and clear nuclei resembling papillary carcinoma-type nuclear changes (b). These cells diffusely express Galectin-3 (c) and HBME-1 (d). In another tumor with a follicular architecture (case 14), questionable papillary carcinoma-type nuclear changes, that is, ground-glass nuclei (e) or pseudoinclusions (f) are seen in some cells. These are strongly and diffusely positive for Galectin-3 (g) and HBME-12 (h). (a: H&E, × 40; b: H&E, × 400; e, f: H&E, × 1000; c, d, g, h: immunoperoxidase, × 400).
The control cases had the expected immunohistochemical profile (Figure 3). All 14 cases of follicular variant of papillary carcinoma were strongly positive for HBME-1. This was true for more than 75% of the tumor cell population in seven instances, and in 25–75% of tumor cells in the remaining cases. Galectin-3 was also positive in all but one case, although the extension of the immunoreactivity was more limited, and in four tumors did not exceed 25% of the neoplastic cell population. The follicular adenomas were generally unreactive for either marker, although one case had a focal staining for HBME-1, and three other adenomas had either single cells (two cases) or focal areas (one case) immunoreactive for Galectin-3 (Table 2).

The control cases of follicular variant of papillary carcinoma (a–c) and follicular adenoma (d–f), have the expected immunohistochemical profile. Galectin-3 and HBME-1 are positive in the former (b, c), and negative in the latter (e, f). A focal and weak nonspecific reactivity for HBME-1 is present at the luminal surface of some follicular cells (f). (a–d: H&E, × 200; b, c, e, f: immunoperoxidase, × 200).
Discussion
The results of these studies indicate that the pattern of immunohistochemical reactivity for Galectin-3 and HBME-1 in UMP-type thyroid tumors mirrors their ambiguous morphologic position between follicular adenomas on one side and well-differentiated carcinomas on the other. More specifically—and not surprisingly—they show that of the two defining criteria for UMP, that is, capsular discontinuity and papillary carcinoma-type nuclear changes, the correlation is largely, if not entirely, restricted to the latter (ie, those cases referred to as WDT-UMP having morphological features related to papillary carcinoma). The finding is of interest on several grounds. Firstly, it supports the notion that the nuclear changes seen, however, focal and incompletely developed, are the expression of a bonafide abnormality rather than a mere artifact of fixation. Secondly, they argue in favor of a pathogenetic link between WDT-UMP and follicular variant of papillary carcinoma, in the sense of the former possibly being a precursor or forme frustre of the latter. Thirdly, it raises an important practical question: Does the pattern of immunoreactivity for Galectin-3 and/or HBME-1 in WDT-UMP have a practical diagnostic value, in the sense of pushing the positive cases into a follicular variant of papillary carcinoma category and the negative ones into a follicular adenoma group? Unfortunately, the present study cannot answer this important question. Doing so will require the study of a larger group of cases with long-term follow-up in order to see whether the biologic attributes of malignancy (particularly the metastatic rate) differ among the various categories.
As far as the group of tumors related to follicular carcinoma (referred to as FT-UMP) is concerned (ie, the tumors with capsular discontinuities but no papillary carcinoma-type nuclear changes), they seem to exhibit, as a group, a slightly greater degree of reactivity for HBME-1 than follicular adenomas, but the magnitude of the difference is too meager for the technique to represent a useful diagnostic adjunct in this situation.
From a practical standpoint, we feel that at present the diagnosis of thyroid tumors of uncertain malignant potential should rest primarily on morphological criteria as previously defined.6 FT-UMP cases, in which the possibility of follicular carcinoma arises because of questionable capsular penetration, do not benefit from Gal-3 or HBME-1 immunoprofiling. Those cases having minor papillary carcinoma-type nuclear alterations (WDT-UMP) can be stained for these markers and the results can be incorporated into the final pathology report. If the markers are positive, a pathogenetic link with papillary carcinoma may be suggested. However, we do not believe that the diagnosis should be influenced by the immunoresults until more information on the natural history of these borderline lesions becomes available.
References
LiVolsi VA . Surgical Pathology of the Thyroid. WB Saunders: Philadelphia, 1990.
Rosai J, Carcangiu ML, De Lellis RA . Atlas of Tumor Pathology: Tumors of the Thyroid Gland. Armed Forces Institute of Pathology Publications: Washington, 1992, pp 161–182.
Castro P, Fonseca E, Magalhaes J, et al. Follicular, papillary, and ‘hybrid’ carcinomas of the thyroid. Endocrinol Pathol 2002;13:313–320.
Mai KT, Bokhary R, Yazdi HM, et al. Reduced HBME-1 immunoreactivity of papillary thyroid carcinoma and papillary thyroid carcinoma-related neoplastic lesions with Hurthle cell and/or apocrine-like changes. Histopathology 2002;40:133–142.
Tzen CY, Huang YW, Fu YS . Is atypical follicular adenoma of the thyroid a preinvasive malignancy? Hum Pathol 2003;34:666–669.
Williams ED, the Chernobyl Pathologists Group. Guest editorial: two proposals regarding the terminology of thyroid tumors. Int J Surg Pathol 2000;8:181–183.
Hirokawa M, Carney JA, Goellner JR, et al. Observer variation of encapsulated follicular lesions of the thyroid gland. Am J Surg Pathol 2002;26:1508–1514.
Orlandi F, Saggiorato E, Pivano G, et al. Galectin-3 is a presurgical marker of human thyroid carcinoma. Cancer Res 1998;58:3015–3020.
Bartolazzi A, Gasbarri A, Papotti M, et al. Thyroid Cancer Study Group. Application of an immunodiagnostic method for improving preoperative diagnosis of nodular thyroid lesions. Lancet 2001;357:1644–1650.
Saggiorato E, Cappia S, De Giuli P, et al. Galectin-3 as a presurgical immunocytodiagnostic marker of minimally invasive follicular thyroid carcinoma. J Clin Endocrinol Metab 2001;86:5152–5158.
Papotti M, Volante M, Saggiorato E, et al. Role of galectin-3 immunodetection in the cytological diagnosis of thyroid cystic papillary carcinoma. Eur J Endocrinol 2002;147:515–521.
Casey MB, Lohse CM, Lloyd RV . Distinction between papillary thyroid hyperplasia and papillary thyroid carcinoma by immunohistochemical staining for cytokeratin 19, galectin-3, and HBME-1. Endocrinol Pathol 2003;14:55–60.
Miettinen M, Karkkainen P . Differential reactivity of HBME-1 and CD15 antibodies in benign and malignant thyroid tumours. Preferential reactivity with malignant tumours. Virchows Arch 1996;429:213–219.
Sack MJ, Astengo-Osuna C, Lin BT, et al. HBME-1 immunostaining in thyroid fine-needle aspirations: a useful marker in the diagnosis of carcinoma. Mod Pathol 1997;10:668–674.
Cheung CC, Ezzat S, Freeman JL, et al. Immunohistochemical diagnosis of papillary thyroid carcinoma. Mod Pathol 2001;14:338–342.
Raphael SJ, McKeown-Eyssen G, Asa SL . High-molecular-weight cytokeratin and cytokeratin-19 in the diagnosis of thyroid tumors. Mod Pathol 1994;7:295–300.
Fonseca E, Nesland JM, Hoie J, et al. Pattern of expression of intermediate cytokeratin filaments in the thyroid gland: an immunohistochemical study of simple and stratified epithelial-type cytokeratins. Virchows Arch 1997;430:239–245.
Baloch ZW, Abraham S, Roberts S, et al. Differential expression of cytokeratins in follicular variant of papillary carcinoma: an immunohistochemical study and its diagnostic utility. Hum Pathol 1999;30:1166–1171.
De Micco C, Ruf J, Chrestian MA, et al. Immunohistochemical study of thyroid peroxidase in normal, hyperplastic, and neoplastic human thyroid tissues. Cancer 1991;67:3036–3041.
Chiappetta G, Bandiera A, Berlingieri MT, et al. The expression of the high mobility group HMGI (Y) proteins correlates with the malignant phenotype of human thyroid neoplasias. Oncogene 1995;10:1307–1314.
Nikiforova MN, Lynch RA, Biddinger PW, et al. RAS point mutations and PAX8-PPAR gamma rearrangement in thyroid tumors: evidence for distinct molecular pathways in thyroid follicular carcinoma. J Clin Endocrinol Metab 2003;88:2318–2326.
Kroll TG, Sarraf P, Pecciarini L, et al. PAX8-PPARgamma1 fusion oncogene in human thyroid carcinoma. Science 2000;289:1357–1360.
Herrmann ME, LiVolsi VA, Pasha TL, et al. Immunohistochemical expression of galectin-3 in benign and malignant thyroid lesions. Arch Pathol Lab Med 2002;126:710–713.
Acknowledgements
The skillful technical support of Dr F Bozzalla-Cassione (University of Turin) is gratefully acknowledged. This work was also supported by grants from the Italian Ministry of Education and Research (Rome; ex-60% to MP) and the Compagnia di San Paolo (Turin, Special project ‘Oncology’ to AB). RDP is recipient of a Research Fellowship from the Fondazione Internazionale di Ricerca in Medicina Sperimentale (FIRMS, Turin, Italy).
Author information
Authors and Affiliations
Corresponding author
Additional information
Duality of interest
None declared.
Rights and permissions
About this article
Cite this article
Papotti, M., Rodriguez, J., Pompa, R. et al. Galectin-3 and HBME-1 expression in well-differentiated thyroid tumors with follicular architecture of uncertain malignant potential. Mod Pathol 18, 541–546 (2005). https://doi.org/10.1038/modpathol.3800321
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/modpathol.3800321
Keywords
This article is cited by
-
Noninvasive follicular thyroid neoplasm with papillary-like nuclear features: a review for pathologists
Modern Pathology (2018)
-
RETRACTED ARTICLE: Noninvasive Follicular Thyroid Neoplasm with Papillary-Like Nuclear Features: Historical Context, Diagnosis, and Future Challenges
Endocrine Pathology (2017)
-
Galectin-3 and HBME-1 improve the accuracy of core biopsy in indeterminate thyroid nodules
Endocrine (2016)
-
Cells of Benign and Borderline Thyroid Tumor Express Malignancy Markers
Bulletin of Experimental Biology and Medicine (2016)
-
Comparing Clinicopathologic and Radiographic Findings Between TT-UMP, Classical, and Non-Encapsulated Follicular Variants of Papillary Thyroid Carcinomas
Endocrine Pathology (2016)
