
Abstract
Study Design:
A retrospective chart review at the major provincial public hospital serving patients with spinal injuries/pathology.
Objectives and setting:
To determine the incidence of spinal tuberculosis (Tb) and establish the profile of these patients treated at King George V Hospital (KGV) in KwaZulu-Natal, South Africa.
Methods:
A total of 525 medical records for the period March 2005 to April 2006 were reviewed. Data from 104 files of Tb spine cases were categorized according to demographic details, medical conditions and length of stay in hospital. The South African mid-year 2006 census was used to calculate associations and risk rates for race, gender, adulthood, urbanization and employment and analyzed using the STATA version 9.0 statistical package.
Results:
About 90% of the patients were African and 10% from other races. Females comprised 58% of the patients. The incidence of Tb spine is 1.02 per 100 000 and 3.13 per 100 000 for Africans and other races, respectively. The incidence rate is 1.17 per 100 000 females and 0.916 per 100 000 males. All the participants had a history of pulmonary Tb and 28% were human immunodeficiency virus positive. Thoracic spine was affected in 42% of the cases. About 32% presented with incomplete paraplegia. The average length of stay at this hospital for these patients was 41 days.
Conclusions:
About 20% of all patients seen for spinal conditions at KGV over the past year presented with Tb spine. A higher association between living in an urban area, adulthood (age 18+), being non-Black patients and the occurrence of spinal Tb was observed.
Similar content being viewed by others

Introduction
Tuberculosis (Tb), more prevalent in immuno-compromised persons1 is still prevalent in developing countries and on the increase in developed ones.2 Skeletal involvement occurs in approximately 10% of all patients with extrapulmonary Tb.3 The thoracic (42%) and lumbar (26%) regions are most affected with other regions less than 12% each.4
South African (SA) provinces most severely affected by Tb are KwaZulu-Natal (KZN) and the Eastern Cape.5, 6 Fifty-seven percent of the population lives in rural areas, with 87% being Black Africans,6 South Africa's previously disadvantaged people. The less educated people have a greater chance of contracting the disease.6
Almost 80% of KZN's population is serviced by KZN Department of Health facilities, divided into six districts.7 The emphasis is on primary health care offered at clinics, supported by district hospitals which refer to secondary and tertiary hospitals usually located at Ethekweni district, for example, King George V Hospital (KGV) for Tb patients.
The KZN Tb statistics is reported inaccurately with the incidence ranging from 37 to 72%.8 The estimated incidence per 100 000 population has increased from 110 in 1995/1996 to 420 in 2000/2001. In 2002 the incidence was reported at 691/100 000.8, 9 This was paralleled by an increase in human immunodeficiency virus (HIV) prevalence, and more than half of Tb patients have been estimated to be HIV positive,8, 9 the prevalence rate of latter has increased from 33.5% in 2001 to 39.1% in 2006.10 The male:female distribution of Tb was 1:5 with no available breakdown by race.8 On 24 April 2007, a budget presentation by the MEC for KZN health suggested a Tb caseload of more than 1000 per 100 000 people.11 Since no information is available on the incidence and profile of spinal Tb in KZN, the present study sought to determine the incidence of spinal Tb and establish the profile of afflicted patients treated at KGV Hospital.
Materials and methods
All medical files (525) of patients admitted to KGV presenting with any spinal condition during the study period (March 2005 to April 2006) were included in the first round of the survey. KGV is the only public hospital in KZN province that manages patients with Tb spine. Patients may be first admitted at any public hospital, but once a diagnosis of Tb spine is confirmed, the patient is transferred to KGV Hospital for further management. Few private patients may be admitted and managed at private hospitals but there is no evidence for this and Tb is typically considered to be a disease afflicting the poor in this country. A validated data abstraction sheet (DAS) was used to collect information from the patients' medical files. The DAS was devised as a single page tool to capture information on patients name, address, telephone number, age, gender, race, causes, diagnosis, medical and surgical management and neurological deficits. All new spinal Tb admissions during the study period were included. Spinal column disorders other than spinal Tb, for example, trauma, other infective conditions were excluded. Ethical clearance was obtained from the University of KwaZulu-Natal Ethics Committee. From the 525 files, only the 104 files belonging to patients with Tb spine were retrieved and analyzed. Data were analyzed using the STATA version 9.0 statistical package to categorize them according to their demographic details, medical conditions and length of stay in hospital. Figures from the mid-year 2006 SA census were used to calculate associations and risk rates for the following factors:race, gender, adulthood, urbanization and employment.
Results
During the March 2005 and April 2006 research period, 525 patients with spinal column conditions were admitted at KGV. Only 104 files were from patients with Tb spine. These patients were admitted at an average of eight patients per month during the research period (range 2–12 patients). Larger numbers of patients were admitted from January 2005 to April 2006 (mean=12 per month) compared to that for the period March 2005 to December 2005 (mean=5.7 per month).
Out of 104 patients, 90% were Africans, 8% Indians and 2% Coloreds. On average these proportions show the admission rates of the different race groups at KGV. The incidence rate of spinal Tb in Africans as obtained from this study is 1.02 per 100 000 and 3.13 per 100 000 in other races (Coloreds and Indians). The incidence rate ratio (relative risk) of spinal Tb in the other races (Coloreds and Indians) is 3.07, indicating that there is a higher association between being another race (Colored and Indian) and the occurrence of spinal Tb.
A total of 58% of the patients who met the inclusion criteria were females with the incidence rate of spinal Tb in this category being 1.17 per 100 000. The incidence rate of spinal Tb in males was 0.916 per 100 000. The incidence rate ratio (relative risk) of spinal Tb in the female population is 1.28, indicating that there is no significant difference between the incidence risk rates of spinal Tb in females when compared to males.
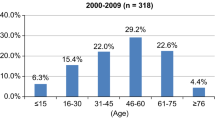
Almost 32% of the sample were children (0–17 years) with 68% being adults (≥18 years+, mean=28 years). The incidence rate of spinal Tb for adults is 1.32 per 100 000 and 724 per 100 000 for children. The incidence rate difference is 597 per 100 000. The incidence rate ratio (relative risk) of spinal Tb in the adult population is 1.82, indicating that there is a higher association between adulthood and the occurrence of spinal Tb.
From the 104 subjects, 61 patients live in urban areas. Out of the 61 patients, 51 patients were Black Africans, 8 Indians and 2 Coloreds. All 43 rural admissions were Black African. The incidence rate of spinal Tb in patients living in urban areas was 1.43 per 100 000 and 0.76 per 100 000 in patients living in rural areas with an incidence rate ratio (relative risk) of 1.88 in the urban population, implying that there is a higher association between living in an urban area and the occurrence of spinal Tb.
Unemployed patients accounted for 81% of the cohort with the spinal Tb incidence rate of 3.02 per 100 000. The incidence rate in the employed patients as per this study was 2.8 per 100 000. The incidence rate ratio (relative risk) of spinal Tb in the unemployed is 1.02, indicating that there is no significant difference between the incidence risk rates of spinal Tb in the unemployed group when compared to the employed group.
All the subjects had a history of pulmonary Tb and 28% were HIV positive. The average length of stay of these patients at the hospital was 41 days. Thoracic spine was involved in 42% of cases, lumbar spine 30% of cases, cervical spine 11% of cases, thoracolumbar 10%, lumbosacral 5% of cases and sacral 2% of cases. Thirty-two percent of the subjects presented with incomplete paraplegia, 24% with complete paraplegia and 44% had no neurological deficits.
Discussion
KGV is the public sector institution in KZN to which patients with pathologies/trauma affecting the spinal column including spinal Tb are referred. Thus the figures presented in this study are representative of all public sector spinal Tb cases for March 2005 to April 2006 in the KZN province. The incidence of spinal Tb varies across countries.12 According to the present study, pulmonary Tb was the primary site as all our subjects had a history of affected lungs. These observations are in line with the findings of Tanriverdi et al.13 who reported that pulmonary Tb is the most common cause of vertebral infection. Francis et al.1 reported that the resurgence of respiratory Tb in the United States has been paralleled by a concomitant rise in Tb of the spine.
McLain et al.3 stated that spinal Tb mostly affects children in developing countries, in accordance with Francis et al.1 who also reported that spinal Tb is generally considered to be the disease of children in developing countries and of the elderly in developed ones. However the findings of the current study do not concur due to more adults being affected. In this study, there is a higher association between adulthood and the occurrence of spinal Tb.
The province of KZN is comprised of 92% of Black Africans.14 KGV is a public institution which only receives referrals of that part of the population who make use of these public services (mainly Black Africans). This group is generally of a lower socioeconomic background. Tb (and thus spinal Tb) is widely thought of as a disease that affects that part of the community with fewer resources6 (economic, infrastructure and so on). Thus the figures compiled do not contain privately serviced patients. This cohort shows that there is a higher association between being non-Black African and the occurrence of spinal Tb. However, since one can assume that the privately serviced group has more and better resources, we can also assume a very minimal number of spinal Tb cases in this group, which requires confirmation through research.
A predominance of spinal Tb in females in this study is supported by Mulleman et al.15 However, Francis et al.1 stated that there is always a male predominance with the ratio of 4:1. In this study a higher incidence rate was also found for females, which is in keeping with the incidence of Tb in KZN.
On the basis of the findings of Statistics SA mid-year 2006,14 57% of KZN population lives in rural areas but 60% of people affected by this disease at the research site are from urban areas. This could be based on the fact that people living in urban areas have higher chances of being exposed to infections. It can also be related to the fact that since democracy in 1994 rural people have moved to urban areas in large numbers but live in informal settlements without the necessary urban sanitation.
Most of the subjects in this study were unemployed with no significant difference between the incidence rates of spinal Tb in the unemployed group when compared to the employed group.
Kumar et al.4 found the thoracic region to be the most affected area in the vertebral column, followed by the lumbar region. These findings are similar to that found in the present study. Kumar et al.4 reported the following distribution: 42% thoracic, lumbar 26%, thoracolumbar and cervical each 12%, cervicodorsal 5% and lumbosacral 3%. Our results in terms of thoracic region involvement at KGV proved to be exactly the same as that reported by Kumar et al.4 with those for the lumbar region higher by 4%. The sacral area is the least affected in the vertebral column with only 2% of cases. This could be due to the fact that the primary source of infection is respiratory Tb; hence all subjects had a history of pulmonary Tb.
McLain et al.3 reported that neurological deficits are common with long-standing thoracic and cervical involvement, and if untreated, neurological involvement may progress to complete and incomplete paraplegia. The results of our study indicate that 56% of our subjects presented with neurological deficits in which 24% had complete paraplegia and 32% incomplete paraplegia.
Conclusion and recommendations
On the basis of the population census of this province, our findings suggest that this condition affects other races more compared to Africans in KZN. Other races are three times more likely to contract spinal Tb than Africans. This is contrary to the assumption that spinal Tb affects Africans more than other races. There is a higher association between adults and the occurrence of spinal Tb. These findings suggest the need for more awareness campaigns on pulmonary Tb across all races and the importance of a multidisciplinary approach to management of its manifestations. We therefore highly recommend more studies on the incidence of this condition for monitoring purposes.
Limitations
About 17 files were missing from the archives department. Inadequate information on some of the files was reviewed. Privately serviced patients were not studied.
References
Francis IM, Das DK, Luthra UK, Sheikh Z, Sheikh M, Bashir M . Value of radiologically guided fine needle aspiration cytology (FNAC) in the diagnosis of spinal tuberculosis. Cytopathology 1999; 10: 390–400.
Dass B, Puet TA, Watanakunakan C . Tuberculosis of the spine (Pott's disease) presenting as ‘compression fractures’. Spinal cord 2002; 40: 604–608.
McLain RF, Isada C . Spinal tuberculosis deserves a place on the radar screen. Cleve Clin J Med 2004; 71: 534–549.
Kumar R, Chandra A . Gluteal abscess: a manifestation of Pott's disease. Neurol India 2003; 51: 87–88.
Weyer K . Tuberculosis and HIV in Southern Africa. Afr Health Care J 2003; 2: 6–9.
. http://users.iafrica.com/a/au/aug/YEP/tuberc.htm 26 July 2006.
. www.kznhealth.gov.za/italian.htm 26 July 2007.
Vella V . Epidemiological estimates of infectious diseases in KwaZulu-Natal. KwaZulu-Natal Epidemiology Bull 2003; 2: 19–20.
Connolly C, Davies GR, D Wilkinson D . Impact of the human immunodeficiency virus epidemic on mortality among adults with tuberculosis in rural South Africa, 1991–1995. Int J Tuberc Lung Dis 1998; 2: 919–925.
. http://www.avert.org/safricastats.htm 27 July 2007.
Nkonkeni P . KZN TB is ‘worse than an epidemic’. Health MEC-KZN, presentation 2007, April 24 http://www.news24.com/News24/South_Africa/News/0,,2-7-1442_2104050.html 26 July 2007.
Moon M-S, Moon J-L, Moon Y-W, Kim S-S, Sun D-H, Choi W-T . (2003): Pott's paraplegia in patients with severely deformed dorsal or dorsolumbar spines: treatment and prognosis. Spinal Cord 2003; 41: 164–171.
Tanriverdi T, Kizilkilic O, Hanci M, Kaymar MY, Unalan H, Oz B . Atypical intradural spinal tuberculosis. Spinal Cord 2003; 41: 403–407.
Statistics South Africa. Mid-year population estimates, South Africa 2006. P0302 1–50.
Mulleman D, Mammou S, Griffoul I, Avimadge A, Goupille P, Valat J-P . Characteristics of patients with spinal tuberculosis in a French teaching hospital. Joint Bone Spine 2006; 73: 424–427.
Acknowledgements
We thank the following for making our study possible: Ms C Connelly and Ms R Shanmugam for their help in statistics. We also thank the KGV staff for their support.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Godlwana, L., Gounden, P., Ngubo, P. et al. Incidence and profile of spinal tuberculosis in patients at the only public hospital admitting such patients in KwaZulu-Natal. Spinal Cord 46, 372–374 (2008). https://doi.org/10.1038/sj.sc.3102150
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3102150
Keywords
This article is cited by
-
Surgical management and clinical outcome of cervical, thoracic and thoracolumbar spinal tuberculosis in a middle-European adult population
Scientific Reports (2023)
-
The prevalence and profile of spinal cord injury in public healthcare rehabilitation units in Gauteng, South Africa
Spinal Cord Series and Cases (2023)
-
Characteristics of patients with spinal tuberculosis: seven-year experience of a teaching hospital in Southwest China
International Orthopaedics (2012)
-
Tuberculosis of the spine. A systematic review of case series
International Orthopaedics (2012)
