
Abstract
Objective:
The objective of this paper is to outline the proposed development process for the ICF Core Sets for Spinal Cord Injury (SCI) and to invite clinical and consumer experts to actively participate in this process. ICF Core Sets are selections of categories of the International Classification of Functioning, Disability and Health (ICF) that are relevant to persons with a specific condition or in a specific setting.
Method:
The project is a cooperation between the ICF Research Branch of the World Health Organization (WHO) Collaboration Centre of the Family of International Classifications (DIMDI, Germany), the Classification, Assessment and Terminology (CAT) team and the Disability and Rehabilitation (DAR) team at WHO, the International Spinal Cord Society (ISCoS) and International Society for Physical and Rehabilitation Medicine (ISPRM) and partner institutions across the world. The project will consist of four worldwide studies to be conducted from 2006 to 2007 with a proposed ICF Core Set Consensus Conference to be held in 2007. ICF categories relevant for SCI are to be identified by means of (I) an empirical study, (II) a systematic review of outcomes and measures used in SCI research (III) an expert survey and (IV) focus groups and semistructured interviews with persons with SCI. Consensus about items that have to be part of a Comprehensive and of a Brief ICF Core Set for SCI will be reached in a final ICF Core Set Consensus Conference. Subsequent field testing will be necessary to validate this first version of ICF Core Sets for SCI.
Invitation for participation:
The development of ICF Core Sets is an inclusive and open process. Anyone who wishes to actively participate in this process is invited to contact the project coordinator (Monika.Scheuringer@med.uni-muenchen.de or http://www.icf-research-branch.org/research/spinalcord-injuries.htm). Individuals, institutions and associations can be formally associated as partners of the project.
Similar content being viewed by others


Introduction
A spinal cord injury (SCI) refers to impairment or loss of motor and/or sensory function in the cervical, thoracic, lumbar or sacral segments of the spinal cord secondary to damage of neural elements within the spinal canal.1 Probably because of the increased survival after a traumatic SCI the prevalence of SCI has increased in the last 20 years.2, 3 Prevalence estimates range from 280/million up to 900/million persons with SCI.3, 4, 5 The likely result of this increasing prevalence is that there will be a growth in the number of persons with chronic disabling conditions. Thus, medical and functional care decisions can lead to tremendous annual and lifetime costs.6
Consequences of SCI
Long-term functional outcomes after SCI result from a combination of acute neurological recovery and medical intervention, rehabilitation and social participation.7 An important basis for the optimal acute and long-term management of SCI is an in-depth understanding, systematic consideration and sound measurement of its consequences at different levels.
With respect to body functions and body structures, SCI is multifaceted and may involve all body functions below the level of the neurological lesion.8 Improving bladder and bowel function has been found to be a shared priority for persons with para- and tetraplegia, while recovery of sexual life was a priority for those with paraplegia and recovery of hand and arm functions a priority for those with tetraplegia.9, 10 Persons with SCI may also often experience spasticity and pain, and have problems with various autonomic functions. They may experience endocrine and metabolic changes due to physical inactivity, which can increase the risk of other complications such as lower limb fractures and cardiovascular disease. In addition, because of impaired sensation, persons with SCI have an increased risk of pressure sores. Finally, they may exhibit depressive symptoms, and studies show that depressive disorders are highly prevalent in persons with SCI.11, 12, 13, 14
Persons with SCI may experience a wide range of activity limitations and participation restrictions. The typical spectrum of activity limitations and participation restriction relate to mobility such as transfers and locomotion,15, 16, 17, 18 self-care activities such as bathing, dressing and toileting,19, 20 difficulties in regaining work, maintaining social relationships, participating in leisure activities and being active members of the community.11, 21 Given the activity limitations resulting from SCI, participation restrictions that a person with SCI might experience are highly dependent on environmental factors.22 For many persons with SCI, barriers in the community are particularly related to mobility equipment and transportation.23, 24, 25 For those who are employed, transportation possibilities are of utmost importance.26 In some countries most persons with SCI have a variety of mobility aids and transportation facilities available to them to live independently and attain high life satisfaction.27, 28
Measuring consequences of SCI
A wide range of instruments is used in research to measure health, psychological and social functioning, well-being and life satisfaction of persons with SCI.29 Most of these functional status and ‘quality of life’ measures were not developed for use in SCI populations and the validity of most measures for use in this group has not been established.30 In a European survey of outcome measures used in hospital departments involved in the treatment and rehabilitation of patients with SCI over 70 measures were identified, but the majority of these were only used in few centres.31
ICF Core Sets
Disadvantages thus occur related to the large variation in currently available measures.32 These include the difficulty to carry data from one episode of care (emergency, medical, rehabilitative, outpatient and community clinical care) over to another episode of care involving a different clinical focus. In addition, for comparability of outcome data across conditions and interventions a common framework is needed that will serve as a ‘Rosetta Stone’.33 With the recent approval of the new International Classification of Functioning, Disability and Health (ICF)34 by the World Health Assembly there is now a comprehensive and universally accepted framework to classify and describe functioning, disability and health in persons with all kinds of diseases or conditions, including SCI.
Completeness and exhaustive detail are essential traits of an international language of functioning and disability; but not every user of the ICF will require the range and detail that ICF provides. Clinicians, for example, who wish to apply the bio-psycho-social model to their daily practice, will require only a fraction of health and health-related states classified in the ICF.
Realizing that the significance and power of the ICF lies in its conceptualization of functioning and disability, there is an urgent call for creating ICF-based instruments that are more appropriate to clinical information needs.35 The ICF Core Sets are responding to this need.36 To date, ICF Core Sets have been developed for 12 chronic conditions (Table 1)33, 37, 38 and others are currently being developed. To address the need for interventions in a specific setting, separate ICF Core Sets have been developed for use in the acute hospital and early postacute rehabilitation facilities.39, 40, 41
Objective
The objective of this paper is to outline the proposed development process for the ICF Core Sets for Spinal Cord Injury and to invite clinical and consumer experts to actively participate in this process.
Methods
The plan to develop ICF Core Sets for SCI was derived in a first meeting held in Nottwil, Switzerland, on 14th and 15th January 2005. This involved members from the ICF Research Branch of the WHO Collaboration Centre of the Family of International Classifications, Germany (Gerold Stucki, Monika Scheuringer), the International Spinal Cord Society (ISCoS) (Fin Biering-Sørensen, Susan Charlifue, Marcel Post), and a Swiss group for the implementation of the ICF (Michael Baumberger, Franz Michel, Hansjörg Lüthi). Starting points that were agreed upon during this meeting and issues that have to be resolved at a later stage are described in this section. These preliminary decisions may be reconsidered after completion of the initial studies.
What types of ICF Core Sets need to be developed?
A key issue when developing ICF Core Sets for SCI is the decision of what core sets should be developed for, that is, which situation and which purpose. This relates to the fact that SCI is initially an acute condition and subsequently a chronic condition that has many different consequences. Therefore, ICF Core Sets for SCI need to address the prototypical spectrum of problems encountered along the continuum from the acute situation to rehabilitation and throughout the lifetime for persons with SCI living in the community.
ICF Core Set for the acute hospital
As patients with SCI are initially not only referred to specialized centres but also to acute hospitals, there is a need for an Acute ICF Core Set to be used by physicians, nurses, therapists and other health professionals working in the acute hospital. The Acute ICF Core Set for Neurological Conditions,42 which has also included patients with SCI, has been developed for this purpose. The Acute ICF Core Set for Neurological Conditions may also be useful for the first days of a hospitalization in a specialized centre when the medical perspective is central and the functioning or rehabilitation perspective is complementary. However, it is necessary to test its applicability for patients with SCI more thoroughly and in different world regions.
ICF Core Set for early postacute rehabilitation
Following a SCI, persons require specialized rehabilitation care. In addition to their rehabilitation care, they also have needs for ongoing medical and nursing care.40 As the spectrum of problems encountered in patients with SCI is very broad, it is unlikely that one of the currently developed Post-Acute ICF Core Sets for Neurological, Musculoskeletal and Cardiopulmonary Conditions43, 44, 45 would be appropriate. Therefore, there appears to be a need to develop ICF Core Sets for SCI for early postacute rehabilitation. There may also be a need for both a Comprehensive ICF Core Set for SCI for multidisciplinary assessments and evaluation and a Brief ICF Core Set for SCI to define a minimal standard regarding what should be measured and reported in every study.
ICF Core Set for chronic SCI
Currently, there is no ICF Core Set for chronic SCI. The ICF Core Set for Chronic SCI is intended to represent the prototypical spectrum of problems that persons with SCI could experience in real life. As these consequences are many, it was decided that there should be both Brief and Comprehensive ICF Core Sets for SCI to address the chronic situation.
Methods to be used in the ICF Core Set development
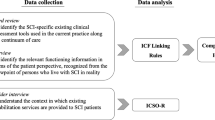
The ICF Core Sets for SCI will be defined at an ICF Core Set Consensus Conference which will integrate (I) evidence from an empirical study, (II) a systematic review of outcomes and measures used in SCI research, (III) an expert survey, and (IV) focus groups and semistructured interviews with persons with SCI. A summary of the methods of the four preliminary studies and the ICF Core Set Conference is shown in Table 2. Figure 1 shows a summary of the time schedule for the ICF Core Set development for SCI.

Time schedule of the development process of ICF Core Sets for SCI
With this study design all relevant perspectives should be addressed adequately. The researcher perspective is addressed with the systematic review. The consumer perspective is addressed both in a quantitative and structured way in the empirical study and in a qualitative way using focus groups and semistructured interviews. Finally, the expert opinion involving professionals from the different backgrounds is addressed with the expert survey.
As the development of ICF Core Sets for SCI must result in practical tools, the ICF Core Set Consensus Conference will primarily involve health professionals from different parts of the world. The maximum number of experts attending the conference was set at 35 (five groups of seven persons), which is considered necessary to address the broad interests to involve the different professions and regions of the world. It was also decided, that each group should consist of different health professionals who will work together in the spirit of partnership and the multiprofessional and interdisciplinary approach, which is typical for care and research for persons with SCI. However, when inviting experts to the conference, the Steering Committee will need to ensure that members are fluent in English to be able to contribute to the process.
Logistics
The project will be a cooperative effort of the ICF Research Branch of the World Health Organization (WHO) Collaboration Centre of the Family of International Classifications (DIMDI, Germany), the Classification, Assessment and Terminology (CAT) team and the Disability and Rehabilitation (DAR) team at WHO, the ISCoS, the International Society for Physical and Rehabilitation Medicine (ISPRM), and partner institutions across the world.
At the Nottwil planning meeting there was also a decision to establish a Steering Committee with two Chairs: Fin Biering-Sørensen for ISCoS and Gerold Stucki for the ICF Research Branch Munich, Germany. The current members are Michael Baumberger (for the Swiss Paraplegic Foundation), Susan Charlifue and Marcel Post (for the Executive Committee for the International SCI Data Sets Committee of ISCoS), Federico Montero (for the WHO DAR Team), and Nenad Kostanjsek (for the WHO CAT Team).
Discussion
ICF Core Sets are practical tools for different purposes. They allow clinicians and researchers to classify and describe individual's functioning using the most relevant ICF codes. A Brief ICF Core Set may facilitate international studies and studies comparing the consequences of different conditions. A Comprehensive ICF Core Set can be used in the clinic as a checklist to assess patient's needs, to formulate rehabilitation goals and to evaluate progress. A general reference framework may be powerful both with regard to communication between health professionals within specific settings and when communicating between health professionals and persons with SCI and between settings.
The goal of the ICF Core Sets to specify what is relevant to study and report for persons with SCI is very much in line with the broader goal of the approach taken by ISCoS and ASIA to define a Core Data Set of variables that can be collected in any study in persons with SCI, as well as various Basic and Extended SCI Data Sets and Modules for specific topics related to persons with SCI.46
As in any scientific endeavour, there are uncertainties that have to be resolved during the process. As mentioned, the preliminary studies will provide the necessary information to guide decisions on (a) which type of ICF Core Sets for SCI to proceed with, and (b) necessary stratification by a number of variables of the ISCoS Core Data Set, for example, between persons with different neurological level or completeness of the SCI. Active contributions by the SCI community to the preliminary studies and the ICF Core Set Consensus Conference will be necessary to make this project successful. It is important to realize that the ICF Core Set Consensus Conference will provide only a first, best possible version of ICF Core Sets for SCI, which will then need to be tested worldwide.
Invitation for participation
The development of ICF Core Sets is an inclusive and open process. Therefore, the authors of this paper encourage clinical and consumer experts to actively participate in the process. Anyone who wishes to actively participate in this process is invited to contact the international project coordinator (Monika.Scheuringer@med.uni-muenchen.de or http://www.icf-research-branch.org/research/spinalcord-injuries.htm). Individuals, institutions and associations can be formally associated as partners of the project.
References
Marino RJ et al. International standards for neurological classification of spinal cord injury. J Spinal Cord Med 2003; 26 (suppl 1): S50–S56.
Frankel HL et al. Long-term survival in spinal cord injury: a fifty year investigation. Spinal Cord 1998; 36: 266–274.
O’Connor PJ . Survival after spinal cord injury in Australia. Arch Phys Med Rehab 2005; 86: 37–47.
Dahlberg A, Kotila M, Leppänen P, Kautiainen H, Alaranta H . Prevalence of spinal cord injury in Helsinki. Spinal Cord 2005; 43: 47–50.
National Spinal Cord Injury Statistical Center. Spinal Cord Injury: Facts and Figures at a Glance. Alabama: Birmingham 2005.
Ackery A, Tator C, Krassioukov A . A global perspective on spinal cord injury epidemiology. J Neurotrauma 2004; 21: 1355–1370.
McKinley W, Meade MA, Kirshblum S, Barnard B . Outcomes of early surgical management versus late or no surgical intervention after acute spinal cord injury. Arch Phys Med Rehab 2004; 85: 1818–1825.
Ditunno JF, Young W, Donovan WH, Creasey G . The international standards booklet for neurological and functional classification of spinal cord injury. Paraplegia 1994; 32: 70–80.
Anderson KD . Targeting recovery: priorities of the spinal cord-injured population. J Neurotrauma 2004; 21: 1371–1383.
Snoek GJ, IJzerman MJ, Hermens HJ, Maxwell D, Biering-Sørensen F . Survey of the needs of patients with spinal cord injury: impact and priority for improvement in hand function in tetraplegics. Spinal Cord 2004; 42: 526–532.
Bombardier CH, Scott RJ, Krause JS, Tulsky D, Tate DG . Symptoms of major depression in people with spinal cord injury: implications for screening. Arch Phys Med Rehab 2004; 85: 1749–1756.
Elliott TR, Frank RG . Depression following spinal cord injury. Arch Phys Med Rehab 1996; 77: 816–823.
Frank RG, Elliott TR, Corcoran JR, Wonderlich SA . Depression after spinal cord injury: is it necessary? Clin Psychol Rev 1987; 7: 611–630.
Krause SJ, Coker JL, Charlifue SW, Whiteneck GG . Health outcomes among American Indians with spinal cord injury. Arch Phys Med Rehab 2000; 81: 924–931.
Waters RL, Adkins RH, Yakura JS, Sie I . Motor and sensory recovery following incomplete tetraplegia. Arch Phys Med Rehab 1994; 75: 306–311.
Penrod LE, Hedge SK, Ditunno JF . Age effect on prognosis for functional recovery in acute, traumatic central cord syndrome. Arch Phys Med Rehab 1990; 71: 963–968.
Crozier KS, Cheng LL, Graziani V, Zorn G, Herbison GH, Ditunno JF . Spinal cord injury: prognosis for ambulation based on quadriceps recovery. Paraplegia 1992; 30: 762–767.
Crozier KS, Graziani V, Ditunno JF, Herbison GH . Spinal cord injury: prognosis for ambulation based on sensory examination in patients who are initially motor complete. Arch Phys Med Rehab 1991; 72: 119–121.
Gerhart K, Bergstrom E, Charlifue SW, Menter R, Whiteneck GG . Long-term spinal cord injury: functional changes over time. Arch Phys Med Rehab 1993; 74: 1030–1034.
Thompson L . Functional changes in persons aging with spinal cord injury. Assist Technol 1999; 11: 123–129.
Schonherr MC, Groothoff JW, Mulder GA, Schoppen T, Eisma WH . Vocational reintegration following spinal cord injury: expectations, participation and interventions. Spinal Cord 2004; 42: 177–184.
Whiteneck GG, Meade MA, Dijkers M, Tate DG, Bushnik T, Forchheimer MB . Environmental factors and their role in participation and life satisfaction after spinal cord injury. Arch Phys Med Rehab 2004; 85: 1793–1803.
Cox RJ, Amsters DI, Pershouse KJ . The need for a multidisciplinary outreach service for people with spinal cord injury living in the community. Clin Rehab 2001; 15: 600–606.
Dunn M, Love L, Ravesloot C . Subjective health in spinal cord injury after outpatient healthcare follow-up. Spinal Cord 2000; 38: 84–91.
Johnson RL, Gerhart KA, McCray J, Menconi JC, Whiteneck GG . Secondary conditions following spinal cord injury in a population-based sample. Spinal Cord 1998; 36: 45–50.
Conroy L, McKenna K . Vocational outcome following spinal cord injury. Spinal Cord 1999; 37: 624–633.
Biering-Sørensen F, Hansen RB, Biering-Sørensen J . Mobility aids and transport possibilities 10–45 years after spinal cord injury. Spinal Cord 2004; 42: 699–706.
Post MW, van Asbeck FW, van Dijk AJ, Schrijvers AJ . Services for spinal cord injured: availability and satisfaction. Spinal Cord 1997; 35: 109–115.
Meyers AR, Andresen EM, Hagglund KJ . A model of outcomes research: spinal cord injury. Arch Phys Med Rehab 2000; 81 (Suppl 2): S81–S90.
Wood-Dauphinee S et al. Quality of life in patients with spinal cord injury: basic issues, assessment, and recommendations. Restorat Neurol Neurosci 2002; 20: 135–149.
Haigh R et al. The use of outcome measures in physical medicine and rehabilitation within Europe. J Rehab Med 2001; 33: 273–278.
Dijkers MP . Quality of life of individuals with spinal cord injury: a review of conceptualization, measurement and research findings. J Rehab Res Develop 2005; 42 (Suppl 1): 87–110.
Üstün B, Chatterji S, Konstansjek N . Comments from WHO for the journal of rehabilitation medicine special supplement on ICF core sets. J Rehab Med 2004; 36 (Suppl 44): 7–8.
World Health Organization. International Classification of Functioning, Disability and Health: ICF. WHO: Geneva 2001.
Stucki G, Ewert T, Cieza A . Value and application of the ICF in rehabilitation medicine. Disab Rehab 2002; 24: 932–938.
Stucki G, Cieza A, Ewert T, Kostanjsek N, Chatterji S, Üstün TB . Application of the International Classification of Functioning, Disability and Health (ICF) in clinical practice. Disab Rehab 2002; 24: 281–282.
Stucki G, Grimby G . Foreword: applying the ICF in medicine. J Rehab Med 2004; 36 (Suppl 44): 5–6.
Cieza A, Ewert T, Üstün B, Chatterji S, Konstansjek N, Stucki G . Development of ICF core sets for patients with chronic conditions. J Rehab Med 2004; 36 (Suppl 44): 9–11.
Stucki G, Üstün BT, Melvin J . Applying the ICF for the acute hospital and early postacute facilities. Disab Rehab 2005; 27: 349–352.
Stucki G, Stier-Jarmer M, Grill E, Melvin J . Rationale and principles of early rehabilitation care after an acute injury or illness. Disab Rehab 2005; 27: 353–360.
Grill E, Ewert T, Chatterji S, Kostanjsek N, Stucki G . ICF Core Set development for the acute hospital and early post-acute rehabilitation facilities. Disab Rehab 2005; 27: 361–366.
Ewert T et al. ICF Core Set for patients with neurological conditions in the acute hospital. Disab Rehab 2005; 27: 367–374.
Scheuringer M et al. ICF Core Set for patients with musculoskeletal conditions in early post-acute rehabilitation facilities. Disab Rehab 2005; 27: 405–410.
Stier-Jarmer M et al. ICF Core Set for patients with neurological conditions in early post-acute rehabilitation facilities. Disab Rehab 2005; 27: 389–396.
Wildner M et al. ICF Core Set for patients with cardiopulmonary conditions early post-acute rehabilitation facilities. Disab Rehab 2005; 27: 397–404.
Biering-Sørensen F et al. International Spinal Cord Injury Data Sets Spinal Cord 2006 (in press).
Acknowledgements
We wish to acknowledge Franz Michel and Hansjörg Lüthi for contributing to the development strategy for the ICF Core Sets for SCI in the first meeting on 14th and 15th January 2005 in Nottwil. We also acknowledge Alarcos Cieza and Eva Grill, who have been leading the efforts to develop ICF Core Sets for chronic conditions and the acute hospital and early postacute rehabilitation facilities for their advice on the study design and the careful review of this paper.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Biering-Sørensen, F., Scheuringer, M., Baumberger, M. et al. Developing core sets for persons with spinal cord injuries based on the International Classification of Functioning, Disability and Health as a way to specify functioning. Spinal Cord 44, 541–546 (2006). https://doi.org/10.1038/sj.sc.3101918
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101918
Keywords
This article is cited by
-
Assessment of pain symptoms and quality of life using the International Spinal Cord Injury Data Sets in persons with chronic spinal cord injury
Spinal Cord Series and Cases (2019)
-
Content comparison of the Spinal Cord Injury Model System Database to the ICF Generic Sets and Core Sets for spinal cord injury
Spinal Cord (2019)
-
Development of the International Spinal Cord Injury Activities and Participation Basic Data Set
Spinal Cord (2016)
-
Quality of life after spinal cord injury: a comparison across six countries
Spinal Cord (2013)
-
Aspects of functioning and environmental factors in medical work capacity evaluations of persons with chronic widespread pain and low back pain can be represented by a combination of applicable ICF Core Sets
BMC Public Health (2012)
