
Abstract
Study design:
Cross-sectional and longitudinal postal survey.
Objectives:
To (1) compare the severity of pain in persons with spinal cord injury (SCI) to national norms, (2) examine the association between pain and measures of (a) psychological functioning, (b) community integration and (c) pain interference with daily activities, and (3) examine the change in the prevalence and intensity of pain over time.
Setting:
Community.
Methods:
A total of 147 adults with SCI were surveyed twice, 2–6 years apart. Main outcome measures included presence/absence of pain in general and at specific body sites, 0–10 numerical rating scale of average pain intensity, modified Brief Pain Inventory Pain Interference scale, SF-36 Bodily Pain scale, SF-36 Mental Health scale, Community Integration Questionnaire.
Results:
Pain was more severe, on average, in this sample of patients with SCI than it is in normative samples. The presence of pain was associated with trends towards poorer psychological functioning and social integration, and the intensity of pain was associated with interference with a number of important basic activities of daily living. Little systematic change was found in pain over a 2–6-year-period, although there was evidence that the prevalence of shoulder pain increases over time.
Conclusion:
The current findings underscore the serious nature of pain in persons with SCI and provide additional support for the need to identify effective treatments for SCI-related pain.
Similar content being viewed by others

Introduction
A growing body of research is beginning to clarify the nature and scope of pain in persons with spinal cord injury (SCI). A recent review of this research concluded that about one-third of patients with SCI report experiencing severe pain, but also noted that a consensus has not yet been reached for how best to treat the pain problems in patients with SCI.1 This same review identified a number of important unanswered questions concerning the nature, scope, and impact of pain in persons with disabilities, including those with SCI. Three of these unanswered questions include: (1) What is the severity of pain in persons with SCI relative to national norms? (2) To what extent does pain interfere with function over and above the effects of the SCI itself? and (3) What is the course of pain in persons with SCI over time?1
Concerning the first question, to our knowledge, and despite the large number of studies that describe the severity of pain in different samples of individuals with SCI, no study has yet compared pain severity in persons with SCI to the pain severity found in normative samples. While pain appears to be common in persons with SCI, pain is also common in the population at large.2, 3, 4 A direct comparison of the pain severity reported by persons who have an SCI with that reported by normative groups is necessary to better understand the relative seriousness of pain problems in SCI populations.1
A second important unanswered question concerns the impact of pain on functioning in persons with SCI. Most previous survey research on pain in persons with SCI has reported on its frequency and severity; although its quality, location(s), and correlates are also often reported.5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15 However, only a limited number of studies have compared persons with SCI who report pain with those who do not report pain on measures of functioning. The little research that has been performed to address this question indicates the following: (1) individuals with SCI and chronic pain are at greater risk for poorer psychological functioning,5, 11, 13, 16, 17 poorer sleep17, 18 and, for those with shoulder pain, perhaps a higher frequency of unemployment and a greater need of physical assistance,19 than those patients with SCI who do not have chronic pain.
However, much is still not known concerning the impact of chronic pain on the lives of persons with SCI. For example, with the exception of one study that suggests that the presence of shoulder pain is associated with higher levels of unemployment,19 we do not know if there are any differences between those with and those without chronic pain on measures of community integration; that is, the ability to perform normal role functions in and outside of the home. Little is also known about the association between pain intensity and the extent to which pain interferes with a large number of specific activities of daily living, such as self-care activities, relations with others, and mobility. More detailed knowledge concerning these associations, as well as the replication of the previously reported association between psychological dysfunction, sleep problems, and the presence of pain, would help clarify the role that pain has in daily functioning in persons with SCI. Ultimately, this knowledge may be used to help identify those functioning or interference domains that should be the focus of pain-related SCI rehabilitation.
Finally, little research has examined the changes in pain over time in persons with SCI. In one retrospective survey, very few respondents indicated that pain had decreased in intensity (6.6%) or frequency (7.1%), while many more indicated increases in both intensity and frequency since the onset of their SCI (47.2 and 33.5%, respectively)13 (see also Nepomuceno et al9). Another study found that time since injury predicted the prevalence of shoulder pain in a sample of men with SCI, with greater time since injury associated with a greater frequency of shoulder pain,6 and one study found that time since injury was associated with a higher prevalence of elbow and shoulder pain, but not with ankle pain or pain in general.20 However, Dalyan et al7 did not find an association between time since injury and the prevalence of upper extremity pain. A number of other retrospective survey studies have found no significant associations between time since SCI and the prevalence or severity of pain, in general,8, 11, 21, 22 although the findings from one study suggested that different types of pain problems may have different onset times.23 In this study, and 5 years following their initial injury, patients with SCI reported that the average onset time of at-level neuropathic pain was 1.2 years following injury, similar to the average onset time of musculoskeletal pain (mean 1.3 years). However, below level neuropathic pain (mean 1.8 years) and visceral pain (mean 4.2 years) were reported to have developed later following injury, on average.
Only a few longitudinal studies have addressed the question of change in pain in persons with SCI over time. In one of these, Kennedy et al24 assessed the presence and intensity of pain at 6 weeks and then again at 1 year following SCI. They found a dramatic increase in both measures over this time period, with 23% reporting severe pain at 6 weeks, and 41% reporting severe pain at 1 year post-SCI. On the other hand, Cairns et al25 found no change in the prevalence of pain from admission to rehabilitation (on average, 19 days following injury) to discharge from rehabilitation (on average, 65 days of rehabilitation for subjects with paraplegia and 124 for subjects with tetraplegia), but they did report that the intensity of pain in those who reported pain at admission decreased significantly over this time period. In another longitudinal study, Weitzenkamp et al26 found that the chances of developing or resolving a pain problem in a sample of patients with established SCI (over 20 years post-SCI) varied as a function of pain site: an increased risk over time was found for developing elbow pain or stiffness, shoulder pain or stiffness, and hand pain or stiffness, and a decreased risk over time was found for developing hip pain or stiffness. Siddall et al23 found moderate (rs range, 0.36–0.48) associations between the severity of below-level and at level neuropathic pain problems assessed at 1 month, 1 year, 2 years, and 3 years following injury, and the severity of pain at 5 years following injury. However, they found no significant associations between the severity of musculoskeletal pain or visceral pain at previous time points (up to 3 years postinjury) and the severity of these pain problems at 5 years postinjury.
As a group, these studies provide some preliminary support for the hypotheses that, (1) there is a great deal of variability in change in pain during the first months and perhaps first years following SCI, with perhaps some initial decrease in pain severity in the first few weeks after injury, and then a progressive increase in the prevalence and severity of pain in the months and immediate years following this; (2) once pain problems emerge in the first months or years following an SCI, the prevalence or intensity of pain, in general, does not appear to increase or decrease dramatically, although (3) there is some possibility that the prevalence of pain in some specific sites (eg, shoulder, wrist, or elbow) may increase over time in patients with established SCI. Further research is needed to clarify the time course of pain in persons with SCI using longitudinal research designs and different samples of patients with SCI.
The purpose of the current study was to fill some of the gaps in our knowledge in the three specific areas concerning pain in persons with SCI discussed above: (1) the severity of pain in persons with SCI relative to national norms; (2) the association between pain and measures of some specific areas of patient functioning and interference with daily activities that have not yet been adequately examined, and (3) change in the prevalence (at specific sites) and intensity of pain over time.
Methods
Participants
Participants for the current survey study were recruited from a sample of patients who had responded to one of two previous surveys of chronic pain problems in persons with SCI14, 15 2–6 years prior to the initiation of the current study, and who had indicated on that previous survey that they were willing to be contacted in the future about research opportunities. Questionnaires were mailed to 339 individuals. Each questionnaire was accompanied by a consent form and a cover letter inviting the potential study participants to participate in the study. Subjects were paid $25 for completing and returning the consent forms and survey. Individuals who failed to return the survey after 2 weeks were called up to three times (if phone numbers were available and current) and reminded to return the survey. The study procedures were approved by the University of Washington Human Subjects review Committee.
Measures
The survey questionnaire included a number of questions assessing demographic (age, education level, employment status, race/ethnicity, marital status) and SCI-related (time since SCI, SCI level) descriptive information. The survey also contained a measure of psychological functioning, a measure of community integration, and, for those reporting a pain problem, measures of pain intensity, pain site, and pain interference.
The SF-36 Mental Health scale (SF-36 MH27) was used as the measure of psychological functioning, and was completed by all study participants (ie, both those reporting and those not reporting a pain problem). This widely used measure has demonstrated reliability, as shown by high internal consistency coefficients (0.81–0.9527) and test–retest stability coefficients (0.75–0.8027). Its validity as a measure of psychological functioning is supported by its association with other measures of psychological functioning.27 The SF-36 MH items are scored so that they have a possible range of 0–100, with higher scores indicating better mental health.
The Community Integration Questionnaire (CIQ28) is a 13-item measure of the lack of handicap (ability to perform normal role functions in and outside of the home) in three domains of functioning: home (participating in shopping, meal preparation, housework, child care (if applicable), personal finance management, and social planning), social (participating in activities outside of the home, travel outside the home, leisure activities with others, and existence/availability of a ‘best friend’), and productive activity (employment status) domains. The CIQ scales evidence good reliability29 and an internal structure supporting their measure of three distinct domains of integration and function.28 The CIQ scales have demonstrated validity through their association with other measures of functioning.25
The two-item Bodily Pain scale from the SF-36 was used as the measure of pain severity (SF-36 BP27). This scale includes a 6-level categorical scale of pain intensity (ranging from ‘None’ to ‘Very severe’), and a 5-level categorical scale of pain interference (that asks respondents to rate the extent to which pain interferes with normal work, including work both outside the home and housework, with responses ranging from ‘Not at all’ to ‘Extremely’), which are combined into a single composite score of pain severity and transformed to a 0–100 scale, with lower scores indicating higher levels of pain severity.
Survey respondents were also asked to indicate the presence or absence of any recent pain problems using the following question: ‘Are you currently experiencing, or have you in the past 3 months experienced, any pain (other than occasional headaches or menstrual cramps)’? Respondents who answered ‘yes’ to this question were then asked to rate the average intensity of this pain during the past week on an 0–10 numerical rating scales, with 0=‘No pain’ and 10=‘Pain as bad as could be’. Such 0–10 scales have demonstrated their validity as measures of pain by their strong association with other measures of pain intensity, as well as by their responsivity to treatments known to impact pain.30
Pain site was assessed using a pain site checklist developed by the researchers that asked respondents to rate the presence or absence of pain in 17 different sites, including the head, neck, shoulder, upper back, lower back, arms, elbows, wrists, hands, buttocks, hips, chest, abdomen/pelvis, legs, knees, ankles, and feet. Most of these sites (all except head and chest) were collapsed into seven site categories (neck, shoulders, arms/hands, back, abdomen, buttocks/hips, legs/feet) to make them comparable to the site lists used in the previous surveys, and therefore to allow an evaluation of change in pain site over time.
Finally, pain interference in specific activities of daily living was assessed using a modified version of the Brief Pain Inventory Pain Interference scale (BPI31, 32). The original version of this scale asks respondents to rate the degree to which pain interferes with seven daily activities, including general activity, mood, walking ability, normal work, relations with other people, sleep, and enjoyment of life. As in our previous studies where we used this scale for assessing pain interference in persons with disabilities,33, 34 we modified the BPI in two ways. First, we changed item 3 (‘Walking ability’) to read ‘Mobility, that is, your ability to get around,’ to be more appropriate for the participants in the current study, many of whom cannot walk. Second, we added three items to assess interference of pain with self-care, recreational activities, and social activities, to obtain a broader-based assessment of areas that could potentially be affected by pain. The original BPI Pain Interference scale has demonstrated validity through its strong association to pain severity across a number of samples of cancer patients32 (see also Cleeland and Ryan31), and the modified version of this scale has demonstrated high levels of internal consistency (Cronbach's α=0.89) and validity through its strong association with pain intensity in samples of persons with disabilities.33, 34
Data analyses
To address the first purpose of the study concerning the difference in pain severity in the current sample and that found in a national normative sample, we compared the subjects' scores on the SF-36 BP scale in the current sample with the published national norms for this same scale27 using a t-test. Two sets of analyses were performed to address the second study purpose; that is, to examine the association between pain and functioning. First, to determine the association between the presence of pain and psychological functioning and community integration, the SF-36 MH and the CIQ scale scores were compared between patients who reported having a pain problem and those who did not report having a pain problem in the past 3 months using t-tests. Second, to examine the association between pain intensity and activities, Pearson correlation coefficients were computed between the 0–10 NRS average pain intensity ratings and the modified BPI pain interference ratings for each of 10 pain interference domains. Finally, to address the third study purpose, that is, to examine the prevalence (at specific sites) and intensity of pain over time, we examined change in pain status from the initial to the current survey using a paired t-test for the continuous variable (average pain intensity) and χ2 tests for the dichotomous variables (presence/absence of pain in general and presence/absence of pain at each of the seven specific body sites).
Results
Response rate
Of the 339 questionnaires mailed, 187 (57%) were returned. Of that number, 27 were returned because the subject was no longer at the address on record, two were returned with a note indicating that the subject was deceased, one was returned with information indicating that the patient was not available for the study (eg, in the hospital and unable to participate), and two were returned with a note indicating that the patient declined participation. The survey return rate was 49% (147 completed questionnaires divided by the number of surveys sent excluding patients who were no longer at their previous address or who were deceased).
Subject characteristics and comparison of survey responders to nonresponders
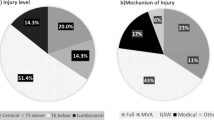
Demographic and SCI-related descriptive information of the 147 survey respondents are presented in Table 1. The mean age of the study subjects was 48.8 years (SD, 13.0; range, 21–88). As previously reported in the samples from which the current subjects were drawn,14, 15 there was a wide degree of variability in the number of years since SCI (range, 3.2–57.4 years; SD, 10.4; mean, 16.6).
In total, 117 (79.6%) of the survey respondents reported that they were experiencing, or had experienced in the past 3 months, a pain problem (Table 2). Among these subjects reporting pain, the most common pain sites were shoulder (60.7%) and back (58.1%), although pain in all sites of the body areas were reported by some subjects. The average pain intensity (in the past week) of the 117 respondents who reported a pain problem was 5.08 (SD, 2.32) on the 0–10 NRS, with 44 (37.6%) reporting mild pain (ie, 1–4 on the 0–10 scale,35, 36), 33 (28.2%) reporting moderate pain (5–6 on the 0–10 scale), and 38 (32.5%) reporting severe pain (7–10 on the 0–10 scale), on average. Two respondents (1.7%) reported that, although they had experienced a pain problem in the prior 3 months, their average pain intensity during the past week was 0.
Given the relatively low response rate, we compared the responders to nonresponders on demographic, pain, and SCI-related variables that were available for all patients who were sent surveys to determine if they differed on any of these variables, using t-tests for continuous variables (age, pain intensity) and χ2 tests for categorical variables (presence of pain, sex/gender, education level, employment status, race/ethnicity, marital status, cause of SCI, level of SCI, and completeness of SCI). The only significant difference to emerge was for education level. Responders reported a higher frequency of education beyond high school (84.4%) when first surveyed then nonresponders (72.7%; (χ2 (1)=6.31, P<0.05).
Study question 1: pain severity comparison with national norms
The results of the analysis comparing SF-36 BP scale scores in the current sample and those from published norms indicated that the patients in the current sample reported greater pain severity, on average (as indicated by a lower score on the SF-36 BP scale; mean, 52.04; SD, 26.82), than a sample drawn from the US population as a whole (mean, 75.15; SD, 23.6927). The difference between these pain severity scores was significant (t (2619)=11.40, P<0.001). The effect size for this difference (d, as calculated by the difference in means divided by the SD of the SF-36 BP scale in the SCI sample37) is 0.86, representing a substantial difference (Cohen's37 standards for small, medium, and large effects are 0.20, 0.50, and 0.80, respectively).
Study question 2: association between pain and functioning
The results of the analyses comparing scores on the SF-36 MH and the CIQ scales between patients with and without pain suggest poorer psychological functioning and social integration among patients reporting pain than among those who did not signify having a pain problem (Table 3). However, if a Bonferroni correction were made for multiple comparisons (0.05/4=0.0125), neither of these differences would be deemed to be statistically significant. There was no significant difference, or even trend for any difference, in the productivity or general home competency integration domains.
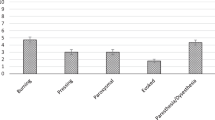
The Pearson correlation coefficients representing the association between average pain intensity and pain interference are presented in Table 4. As can be seen, pain intensity showed a strong association with each of the 10 domains of pain interference assessed by the modified BPI, with correlation coefficients ranging from 0.50 to 0.59 (all P's<0.001; still below the level of significance required if a Bonferroni correction were made in light of the fact that 10 coefficients were computed).
Study question 3: change in the frequency and intensity of pain over time
The average time between the previous and the current surveys was 4.81 years (range, 2–6 years). In the initial surveys, 114 of the subjects in the current study reported having a pain problem and 33 reported that they did not have a pain problem; these numbers were 117 and 30 in the current sample. Change in pain status occurred for 23 subjects; 13 changed from reporting no pain (initial survey) to reporting a pain problem (current survey), and 10 changed from reporting a pain problem to reporting no pain. Overall, the change in the prevalence of pain over time was not statistically significant (χ2 (1)=0.38, P=0.54). Of the 77 subjects for whom average pain intensity ratings (during the past week) were available from both the previous and current surveys, the change in average pain intensity was not large or statistically significant (initial mean (SD), 5.21 (2.13); current mean (SD), 5.40 (2.22); t (76)=0.85, P=0.40). An examination of change in the rates of pain at specific body sites yielded only one statistically significant finding: there were a larger number of patients who reported having shoulder pain in the current survey of 147 participants (48.3%) than who reported having shoulder pain in the previous surveys (34.7%). The net increase in the rate of shoulder pain of individuals from the initial to the current survey was statistically significant (χ2 (1)=12.01, P=0.001; still below the level of significance required if a Bonferroni correction were made for the seven analyses associated with testing changes in the presence of pain at each site).
Discussion
The current study extends the findings from previous research on the nature and scope of pain in persons with SCI. In this first comparison of the pain severity between a sample of individuals with SCI and US national norms, we found pain to be statistically and substantially greater in the former compared with the latter. In addition, we found that the presence of pain was associated with trends towards lower levels of psychological functioning and social integration, and that pain intensity showed strong and consistent associations with ratings of pain interference in a large number of daily activities. Finally, measures of pain prevalence and intensity, in general, did not appear to increase or decrease substantially over time. However, there is some indication that shoulder pain may increase in frequency over the course of 2–6 years. The implications of these findings for understanding pain in persons with SCI are discussed below.
The significant and substantial differences in pain severity between the current sample of persons with SCI and a normative sample underscores the seriousness of pain problems in persons with SCI. Although it might be argued that pain problems are common in many, if not most, samples of patient and nonpatient groups, the current findings indicate that pain problems are particularly severe among many persons with SCI. This is consistent with the hypothesis that there are factors in SCI that contribute to the development and maintenance of chronic pain. Such factors might include, but are not necessarily limited to, the neuropathic pain that develops in the initial months and years following the original injury that is the direct result of the damage to the spinal cord.5, 9, 10, 13, 24 In addition, new, musculoskeletal pain problems may develop over time that are caused by abnormal ‘wear and tear’ associated with the repeated physical efforts required for mobility (eg, stress on the shoulder joint associated with use of a manual wheelchair).38, 39 Regardless of the causes and mechanisms of pain in persons with SCI, the current results showing high levels of pain severity in many persons with SCI provide important additional support for the need to identify the causes of, and effective treatments for, these pain problems.
Pain can have important negative impacts on the quality of life of persons with SCI. Previous findings concerning the negative impact of pain on psychological functioning5, 11, 13, 16 were replicated in this study. Extending this research into a new domain of functioning, we found nonsignificant (when significance level was corrected using a Bonferroni correction) trends for an association between the presence of pain and lower levels of social integration. However, very weak associations were found between the presence of pain and measures of productive activity and home competency. These findings suggest the possibility that pain may begin to impact activities associated with social functioning (eg, participating in activities outside of the home, travel outside the home, and leisure activities with others) before it impacts the more basic activities associated with employment and homemaking; given limited resources to manage pain, patients with SCI may choose to allow pain to stop them from socializing before they allow pain to stop them from working or shopping for groceries.
On the other hand, among those study participants who did report a pain problem, strong and consistent associations were found between the average intensity of pain and interference in 10 different basic activities of daily living assessed by the modified BPI Pain Interference scale. This finding suggests that as pain becomes severe, it can have a substantial negative impact on even very basic activities such as sleep, mood, mobility, and self-care activities.
If the associations found between pain and these functioning domains are replicated in future research, then they would support the need to not only identify effective analgesic treatments for pain in persons with SCI, but also, perhaps, the need to develop and test interventions that minimize the impact of pain on functioning in persons with SCI, even when the pain itself does not respond to treatment. For example, behavioral and cognitive-behavioral treatments have been developed and been shown to benefit people with chronic pain as a primary presenting problem.40, 41 Preliminary research suggests that such interventions might also benefit persons with chronic pain and physical disabilities, such as SCI.42, 43
For example, in one preliminary study, 18 individuals with disabilities (including 10 with SCI) were provided with either eight 90-min sessions of a cognitive-restructuring intervention designed to minimize negative cognitions in response to pain (‘catastrophizing’ responses) or eight 90-min sessions of a control intervention (education about chronic pain).42 The participants who received cognitive-restructuring reported greater pre to post-treatment decreases in pain intensity than those in the control condition. In a separate preliminary study, 33 adults with chronic pain and a disability (including 13 with SCI) were given 10 sessions of self-hypnosis training for decreasing perceived pain.43 As a group, the participants in this study reported significant pre to post-treatment decreases in pain intensity that were maintained at 3-month follow-up. Among the 26 participants who completed all 10 sessions of treatment, 10 (37%) reported clinically meaningful (30% or greater) decreases in average daily pain intensity. Although controlled trials of these interventions are needed to prove their efficacy in persons with SCI beyond the effects that might occur because of expectancy alone, these preliminary studies suggest the possibility that these interventions have the potential for benefiting patients with both chronic pain and SCI. The current findings suggest that appropriate additional targets of such interventions might also include (but perhaps not be limited to) psychological functioning/depressive symptoms, social integration, and, among those with severe pain, basic activities of daily living.
The findings from the longitudinal analyses are consistent with previous research that has found no significant associations between the duration of the SCI and the prevalence of pain.8, 11, 21, 22 This high degree of stability in pain across time might be considered good news for patients with SCI who have not developed a chronic pain problem in the first years following the SCI, but might be considered bad news for those who do experience pain; especially those who experience severe pain. On the other hand, the current findings replicate those of others6, 20 indicating an increase in the incidence of shoulder pain in persons with SCI. Our replication of the stability of pain in general, and the increase of shoulder pain specifically, provides even greater support for the need to identify and develop effective pain treatments for pain in persons with SCIs.
A primary limitation of the current study is the relatively low response rate (49%). Analyses comparing responders and nonresponders suggest similarity on all available demographic, pain-related, and SCI-related variables except for education level; responders reported a greater frequency of education beyond high school than nonresponders. This suggests that the finding may be somewhat more generalizable to individuals with SCI who are more educated. In any case, there is a need for replication in other samples of persons with SCI to help determine which of the findings replicate across samples and settings. In addition, we performed seven tests to determine if any changes in pain occur specific sites over time. Although the single significant finding that emerged (an increase in the incidence of shoulder pain over time) was still statistically significant even when controlling for multiple tests using a Bonferroni correction, and this finding is consistent with previous research, it remains possible that this finding could have been spurious in the current sample. Additional replications of this finding in other samples of persons with SCI would help establish its generalizability. Finally, although the study examined the association between pain prevalence and severity and patient functioning in some functioning domains that have not yet been adequately examined (specifically, community integration and some specific daily activities), a number of patient functioning domains were not included in the survey, limiting our ability to examine the impact of pain in these other domains. Future researchers could perhaps cast a wider net in their assessment of patient functioning, which would allow for a more detailed examination of the areas of functioning that are more, or less, impacted by pain.
Conclusion
Despite the limitations of the current study, the findings provide new information about the nature and scope of pain in persons with SCI. First, pain was found to be, on average, more severe in this sample of patients with SCI compared with a normative sample of individuals without SCI. Also, the presence of pain showed a trend to be associated with poorer psychological functioning and social integration, and the intensity of pain was associated with interference with a number of important basic activities of daily living. Finally, little systematic change was found in pain over a 2–6-year period, although there was some evidence that the prevalence of shoulder pain increases over time. The current findings underscore the serious nature of pain in persons with SCI, and provide additional support for the need to identify effective treatments for the prevention and management of SCI-related pain.
References
Ehde DM, Jensen MP, Engel JM, Turner JA, Hoffman AJ, Cardenas DD . Chronic pain secondary to disability: a review. Clin J Pain 2003; 19: 3–17.
Bergman S et al. Chronic musculoskeletal pain, prevalence rates, and sociodemographic associations in a Swedish population study. J Rheumatol 2001; 28: 1369–1377.
Elliott AM, Smith BH, Penny KI, Smith WC, Chambers WA . The epidemiology of chronic pain in the community. Lancet 1999; 354: 1248–1252.
Picavet HS, Schouten JS . Musculoskeletal pain in the Netherlands: prevalences, consequences and risk groups, the DMC(3)-study. Pain 2003; 102: 167–178.
Anke AGW, Stenejem AE, Stanghelle JK . Pain and life quality within 2 years of spinal cord injury. Paraplegia 1995; 33: 555–559.
Ballinger DA, Rintala DH, Hart KA . The relation of shoulder pain and range-of-motion problems to functional limitations, disability, and perceived health of men with spinal cord injury: a multifactoral longitudinal study. Arch Phys Med Rehabil 2000; 81: 1575–1581.
Dalyan M, Cardenas DD, Gerard B . Upper extremity pain after spinal cord injury. Spinal Cord 1999; 37: 191–195.
Demirel G, Yllmaz H, Gencosmanoglu B, Kesiktas N . Pain following spinal cord injury. Spinal Cord 1998; 36: 25–28.
Nepomuceno C et al. Pain in patients with spinal cord injury. Arch Phys Med Rehabil 1979; 60: 605–609.
Ravenscroft A, Ahmed YS, Burnside IG . Chronic pain after SCI: a patient survey. Spinal Cord 2000; 38: 611–614.
Rintala DH et al. Chronic pain in a community-based sample of men with spinal cord injury: prevalence, severity, and relationship with impairment, disability, handicap, and subjective well-being. Arch Phys Med Rehabil 1998; 79: 604–614.
Siddall PJ et al. Pain report and the relationship to physical factors in the first 6 months following spinal cord injury. Pain 1999; 81: 187–197.
Störmer S et al. Chronic pain/dysaesthesiae in spinal cord injury patients: results of a multicentre study. Spinal Cord 1997; 35: 446–455.
Turner JA, Cardenas DD . Chronic pain problems in individuals with spinal cord injuries. Sem Clin Neuropsychiat 1999; 4: 186–194.
Turner JA, Cardenas DD, Warms CA, McClellan CB . Chronic pain associated with spinal cord injuries: a community survey. Arch Phys Med Rehabil 2001; 82: 501–508.
Rintala DH, Hart KA, Priebe MM . Predicting consistency of pain over a 10-year period in persons with spinal cord injury. J Rehabil Res Devel 2004; 41: 75–88.
Budh CN, Hultling C, Lundeberg T . Quality of sleep in individuals with spinal cord injury: a comparison between patients with and without pain. Spinal Cord 2005; 43: 85–95.
Biering-Sørenson F, Beiring-Sørenson M . Sleep disturbance in the spinal cord injured: an epidemiological questionnaire investigation, including a normal population. Spinal Cord 2001; 39: 505–513.
Gerhart KA, Bergstrom E, Charlifue SW, Menter RR, Whiteneck GG . Long-term spinal cord injury: functional changes over time. Arch Phys Med Rehabil 1993; 74: 1030–1034.
Vogel LC, Krajci KA, Anderson CJ . Adults with pediatric-onset spinal cord injury. Part 2: musculoskeletal and neurological complications. J Spinal Cord Med 2002; 25: 117–123.
Pentland W, McColl MA, Rosenthal C . The effect of aging and duration of disability on long-term health outcomes following spinal cord injury. Paraplegia 1995; 33: 367–373.
Widerström-Noga EG, Duncan R, Felipe-Cuervo E, Turk DC . Assessment of the impact of pain and impairments associated with spinal cord injuries. Arch Phys Med Rehabil 2002; 83: 395–404.
Siddall PJ, McClelland JM, Rutkowski SB, Cousins MJ . A longitudinal study of the prevalence and characteristics of pain in the first 5 years following spinal cord injury. Pain 2003; 103: 249–257.
Kennedy P, Frankel H, Gardner B, Nuseibeh I . Factors associated with acute and chronic pain following traumatic spinal cord injuries. Spinal Cord 1997; 35: 814–817.
Cairns DM, Adkins RH, Scott MD . Pain and depression in acute traumatic spinal cord injury: origins of chronic problematic pain? Arch Phys Med Rehabil 1996; 77: 329–335.
Weitzenkamp DA, Jones RH, Whiteneck GG, Young DA . Ageing with spinal cord injury: cross-sectional and longitudinal effects. Spinal Cord 2001; 39: 301–309.
Ware JE, Snow KK, Kosinski M . SF-36 Health Survey: Manual and Interpretation Guide. Quality Metric Incorporated: Lincoln, RI 2000.
Sander AM et al. The Community Integration Questionnaire revisited: an assessment of factor structure and validity. Arch Phys Med Rehabil 1999; 80: 1303–1308.
Willer B, Rosenthal M, Kreutzer JS, Gordon WA, Rempl R . Assessment of community integration following rehabilitation for traumatic brain injury. J Head Trauma Rehabil 1993; 8: 75–87.
Jensen MP, Karoly P . Self-report scales and procedures for assessing pain in adults. In: Turk DC, Melzack R (eds). Handbook of Pain Assessment, 2nd edn. Guilford Publications: New York 2001, pp 15–34.
Cleeland CS, Ryan KM . Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med 1994; 23: 129–138.
Daut RL, Cleeland CS, Flannery RC . Development of the Wisconsin Brief Pain Questionnaire to assess pain in cancer and other diseases. Pain 1983; 17: 197–210.
Hanley MA et al. Psychosocial predictors of long-term adjustment to lower-limb amputation and phantom limb pain. Disabil Rehabil 2004; 26: 882–893.
Tyler EJ, Jensen MP, Engel JM, Schwartz L . The reliability and validity of pain interference measures in persons with cerebral palsy. Arch Phys Med Rehabil 2002; 83: 236–239.
Jensen MP, Smith DG, Ehde DM, Robinson LR . Pain site and the effects of amputation pain: further clarification of the meaning of mild, moderate, and severe pain. Pain 2001; 91: 317–322.
Serlin RC, Mendoza TR, Nakamura Y, Edwards KR, Cleeland CS . When is cancer pain mild, moderate or severe? Grading pain severity by its interference with function. Pain 1995; 61: 277–284.
Cohen J . Statistical power analysis for the behavioral sciences 2nd edn. Lawrence Erlbaum: Hillsdale, NJ 1989.
Kemp B, Thompson L . Aging and spinal cord injury: medical, functional, and psychosocial changes. SCI Nursing 2002; 19: 51–60.
Finley MA, Rodgers MM . Prevalence and identification of shoulder pathology in athletic and nonathletic wheelchair users with shoulder pain: a pilot study. J Rehabil Res Dev 2004; 41: 395–402.
Sanders SH . Operant conditioning with chronic pain: back to basics. In: Turk DC, Gatchel RJ (eds). Psychological Approaches to Pain Management. Guilford: New York 2002, pp 128–137.
Turk DC . A cognitive-behavioral perspective on treatment of chronic pain patients. In: Turk DC, Gatchel RJ (eds). Psychological Approaches to Pain Management. Guilford: New York 2002, pp 138–158.
Ehde DM, Jensen MP . A pilot study of the effects of a cognitive restructuring intervention on chronic pain in persons with disabilities. Rehab Psychol 2004; 49: 254–258.
Jensen MP et al. Hypnotic analgesia for chronic pain in persons with disabilities: a case series. Int J Clin Exp Hyp 2005; 53: 198–228.
Acknowledgements
This research was supported by Grant no. P01 HD33988 from the National Institutes of Health, National Institute of Child Health and Human Development, National Center for Rehabilitation Research, and by Grant no. H133N00003 from the National Institute on Disability and Rehabilitation Research, Office of Special Education and Rehabilitative Services, US Department of Education. We gratefully acknowledge the contributions of Lindsay Washington, Laura Nishimura, Kevin Gertz, Emily Phelps, Kristin McArthur, Silvia Amtmann, and Noel Peryra-Johnston, University of Washington Department of Rehabilitation Medicine, in data collection and database management.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Jensen, M., Hoffman, A. & Cardenas, D. Chronic pain in individuals with spinal cord injury: a survey and longitudinal study. Spinal Cord 43, 704–712 (2005). https://doi.org/10.1038/sj.sc.3101777
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101777
Keywords
This article is cited by
-
Examining the complexity of functioning in persons with spinal cord injury attending first rehabilitation in Switzerland using structural equation modelling
Spinal Cord (2020)
-
Validation and psychometric evaluation of the Italian version of the Spinal Cord Injury Secondary Conditions Scale
Spinal Cord (2020)
-
Assessment of pain symptoms and quality of life using the International Spinal Cord Injury Data Sets in persons with chronic spinal cord injury
Spinal Cord Series and Cases (2019)
-
Reliability of the Italian version of the International Spinal Cord Injury Pain Basic Data Set
Spinal Cord (2019)
-
Relationships between type of pain and work participation in people with long-standing spinal cord injury: results from a cross-sectional study
Spinal Cord (2018)
