
Abstract
Study design: Prospective before–after trial.
Objective: To examine the changes of natural killer (NK) cell activity in response to orthotic gait exercise in thoracic level of spinal cord-injured (SCI) patients.
Setting: National Rehabilitation Center for Persons with Disabilities, Japan.
Methods: In all, 10 thoracic level of SCI patients (ranging Th5–Th12), who experienced orthotic gait training, participated in this study. NK cell activity at an effector:target (E/T) ratio (20:1) was examined in a sample of peripheral blood taken before and just after orthotic gait exercise for 20 min. On a separate day, to evaluate the physical intensity of the orthotic gait exercise, cardiorespiratory responses at rest and during exercise were measured.
Results: The resting value of the NK cell activity in our SCI patients was remarkably lower than that in normal subjects reported in previous studies. The NK cell activity was significantly increased through a 20 min orthotic gait exercise (pre versus post; 12.7±5.28 versus 17.76±6.71, P<0.05). The steady-state value of oxygen () and heart rate (HR) were 18.13±3.92 ml/kg and 142.53±19.84 b/min, respectively. It was noteworthy that a patient who showed decrement of NK cell activity in response to exercise had the highest level of injury (Th5), and showed the higher energy cost of orthotic gait.
Conclusion: These findings suggested that the orthotic gait exercise has the potential to enhance the immune function for SCI persons, although patients with a higher level of SCI may have some difficulties.
Sponsorship: Mitsui Sumitomo Insurance Welfare Foundation
Similar content being viewed by others


Introduction
Natural killer (NK) cells have been proposed as a major factor in the first-line defense system against viral infection.1, 2 Previous investigations demonstrated that spinal cord injury (SCI) brings depression of the immune system including decreased NK cell activities, and also reported restoration of the immune function through the rehabilitation therapy.3
Orthotic gait training is usually prescribed for paraplegic patients with SCI in the therapeutic phase to promote their general health. On the other hand, there are several obstacles to achieving locomotion for paraplegic patients, in particular the high-energy cost of orthotic gait leads to exhaustion within a few minutes of walking (for a review, see Nene et al4). Although some positive effects of orthotic gait have been reported,5 it is still unclear whether the physical intensity of the orthotic gait is suitable for SCI patients to promote their health or not.
We previously examined the physiological characteristics of orthotic gait in thoracic level of SCI patients, and our findings suggested that the physical intensity during walking exercise is suitable to promote the aerobic capacity of SCI patients.6 In the present study, we designed a direct approach to clarify the effect of orthotic gait exercise on the general health of SCI patients, particularly in terms of exercise-induced changes in NK cell activity. Previous investigations revealed that moderate intensity exercise can enhance NK cell activity.1, 7, 8 Therefore, we focused on whether orthotic gait exercise in particular could enhance NK cell activity.
Methods
Subjects
In all, 10 SCI patients who met the following criteria participated in this study: (i) injured at thoracic level, (ii) complete motor paralysis in the lower limb muscle (ASIA classification; grade A or B), (iii) no history of cardiorespiratory disease. All patients were at least 6 months since time of injury, with time since injury ranging from 8 to 32 months (Table 1). Each subject gave his or her informed consent to the experimental procedure, which was approved by the local biological ethics committee of the National Rehabilitation Center for the Persons with Disabilities (NRCD).
Orthotic gait training
All patients had undergone a standard rehabilitation program, consisting of muscle stretching, balance training, and transfer activity, and participated in orthotic gait training with a weight-bearing control orthosis (WBC) or advanced reciprocating gait orthosis (ARGO). Eight of 10 patients have kept the orthotic gait training for 15 weeks, and the other two patients have kept for 10 (patient E) and 4 weeks (patient G), respectively. Although there is individual variation, in many cases, lower thoracic level of paraplegic patients could walk after 10 weeks of gait training independently, while it needs more practice for higher thoracic level of patients. After the training period, each subject could perform the orthotic gait (patients F and G still required light support to avoid falling) independently, and were able to walk continuously for at least 20 min.
Apparatus
Appearance and sequential picture of walking with WBC and ARGO were shown in Figure 1. The mechanical features of the WBC have been fully described elsewhere.11, 12 This orthosis consists of a rigid frame that supports the user's body weight, a special hip joint device that reciprocally propels each leg forward, a gas-powered foot device that varies the sole thickness of the device for foot/floor clearance, and a control system of the orthosis. As a whole these mechanical features enable a user to ambulate at a faster speed and with less energy expended.6 The ARGO also has a special hip joint device named ‘hip driving cable’ which connects both sides of the leg frame. With this device a torque exerted by the right (left) hip joint is mechanically transmitted to the left (right) hip joint, resulting in the torque to the opposite direction exerted by the left (right) hip joint.

Appearance and sequential picture of walking with weight-bearing control orthosis (WBC; above) and advanced reciprocating gait orthosis (ARGO; below)
Physical intensity during orthotic gait
On a separate day, cardiorespiratory responses at rest and during orthotic gait were measured. Subjects were asked to abstain from alcohol and caffeine for at least 12 h before the experiment. The temperature and humidity on the experiment were 23.5±4.2°C and 68.3±3.3%, respectively. The experimental procedure was as follows: 5 min at rest in the sitting position, 20 min of continuous walking at the most comfortable speed. The cardiorespiratory parameters at rest and during walking were measured continuously with a telemetric device (K4 Cosmed, Italy) and were analyzed in real time. The telemetric device consists of a transmitting unit, a face mask to sample the expired gas, a heart rate chest strip, a battery, and a receiving unit. The following cardiorespiratory parameters were obtained: oxygen uptake () and heart rate (HR). Walking speed in the steady state during walking and rating of perceived exertion (RPE) score were also recorded. After the experiments, the energy consumption and walking energy cost were calculated. The terms adopted were those of Nene and Patrick9 and calculations performed according to their protocol:


where K=20.19 J/ml, since 1 ml O2=4.825 cal and 1 cal=4.184 J.
NK cell activities
Blood samples were drawn from an antecubital vein with the patient in the seated position before and just after orthotic gait exercise. The exercise consisted of 20 min of continuous walking at the most comfortable speed in the inside of the hospital ward.
NK cell activity was determined by (superscript: 51) Cr-release cytotoxicity assay using the K562 cell-line which derived from cells with chronic myelogenous leukemia as targets, and calculated using the following formula: %NK cell activity={(experiment mean − spontaneous mean)/(total mean − spontaneous mean)} * 100. In all NK cell activity testing, percent of spontaneous release was less than 5% of total release. Effector:target (E:T) ratios used were 20:1. Controls included cultures of untreated cells (spontaneous release) and cells treated with 3% sodium dodecyl sulfate (SDS) (total release).
Statistical analysis
Values are given as the mean±SD. Statistical difference in NK cell activity between pre- and postexercise was tested by paired t-test. Significance was accepted at P<0.05.
Results
Physical intensity during orthotic gait
The average walking speed during orthotic gait was 18. 01±2.22 m/min. Eight of 10 patients were able to walk continuously, without stumbling, for 20 min. Table 2 shows the cardiorespiratory responses, energy consumption, energy cost, walking speed, and RPE during orthotic gait. During walking, cardiorespiratory parameters clearly showed a significant increase compared with resting rate. The steady-state value of the () ranged from 14.20 to 24.83 ml/kg (average value=18.13±3.92 ml/kg), and HR was 99.2–166.4 b/min (average value=142.53±19.84 b/min). The energy consumption and energy cost during walking were 5.94±1.16 J/kg/s and 19.63±5.04 J/kg/m, respectively. The RPE score just after exercise ranged from 13 to 19 (median value: 15).
NK cell activity
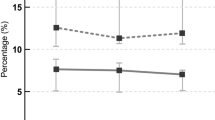
The average value of NK cell activity in the SCI patients at rest (12.7±5. 28; ranging from 7.6 to 23.4) was remarkably lower than the standard value in the healthy nondisabled persons (32.9±15.8). Nine of 10 patients showed enhancement of NK cell activity in response to the 20 min of orthotic gait exercise. The total average value of the postexercise NK cell activity was significantly higher than that of the pre-exercise (pre versus post; 12.7±5.28 verses 17.76±6.71, P<0.05, Table 3, Figure 2).

Natural killer (NK) cell activity in response to 20 min of orthotic gait exercise. Thick and thin lines indicate the total averaged (n=10) and each subject's value, respectively. NK cell activity was represented by an E/T ratio (20:1)
Discussion
In the present study, we aimed to examine the effect of orthotic gait exercise on the NK cell activity in SCI patients. The main observations made here were as follows: (i) the NK cell activity in SCI patients was remarkably lower than the standard value in healthy persons; (ii) the NK cell activity was significantly increased through 20 min of orthotic gait exercise, and (iii) the one patient who showed decrement of NK cell activity in response to exercise had an injury of the highest level (Th5) and showed the higher energy cost during orthotic gait exercise.
Previous investigations have reported that SCI was accompanied by depression of immune system including decrement of NK cell activities.3 These findings, taken together with the fact that paraplegic patients have significantly reduced peak values as a consequence of the reduction in the daily activity levels,10 suggest that the decrements of NK cell activity may be the result of limitation of the patient's physical activity.
Because immune resistance is generally regarded as an essential factor for health care, it is conceivable that enhancement of immune function is important for SCI patients to maintain decent physical condition. In this regard, many investigations have reported the possibility of enhancement of immune function through moderate exercise not only in normal persons1, 7, 8 but also in SCI patients.11 Kliesch et al3 demonstrated restoration of immune function through rehabilitation therapy in treated subjects by comparison with those not receiving treatment. The present result of exercise-induced enhancement of NK cell activity is in good agreement with these reports. In the present study, the steady-state value of the during orthotic gait was 18.13±3.92 ml/kg, and HR was 142.53±19.84 b/min (Table 2). The level of physical intensity implied by these values was considered to be suitable for promoting the general health of SCI patients. Further, all of our subjects, with the exception of patient F, could walk for a considerable time and distance without exhaustion. It is therefore considered that the enhancement of NK cell activities was the result of the suitable aerobic condition during orthotic gait.
Finally, we considered why only patient F showed a decrement in the NK cell activity in response to the orthotic gait exercise. As mentioned above, this patient showed the higher energy cost during orthotic gait and had the highest level of injury in all eight patients. The orthotic gait for SCI patients requires compensatory motion of the residual trunk and upper limbs to swing the paralyzed leg.12, 13 Patient F, who was injured at Th5, could not contract his trunk muscles due to motor paralysis. Consequently, the excess energy expenditure and burden on his upper limbs made it impossible for him to achieve suitable exercise intensity for enhancement of immune function during orthotic gait. His higher RPE score (19: very very hard, Table 2) reflects greater energy consumption than that of the other patients during orthotic gait.
To date, many researchers have reported extremely high-energy requirements of orthotic gait.4, 14, 15 Although many devices have been developed to improve this problem to date, it is still unknown whether the orthotic use contribute to facilitate the health care for SCI persons. The present result provides evidence of the effectiveness of the orthotic gait exercise for promotion of the general health of these SCI patients. However, the question remains whether regular exercise training leads to chronically elevated NK cell activity. Further study will be needed to clarify this issue.
References
Shephard RJ, Shek PN . Effects of exercise and training on natural killer cell counts and cytolytic activity. Sports Med 1999; 28: 177–195.
Welsh RM . Regulation of virus infections by natural killer cells: A review. Nat Immun Cell Growth Regul 1986; 5: 169–199.
Kliesch WF, Cruse JM, Lewis RE, Bishop GR, Brackin B, Lampton JA . Restoration of depressed immune function in spinal cord injury patients receiving rehabilitation therapy. Paraplegia 1996; 34: 82–90.
Nene AV, Hermens HJ, Zilvold G . Paraplegic locomotion: a review. Spinal Cord 1996; 34: 507–524.
Thoumie P et al. Restoration of functional gait in paraplegic patient with the RGO-II hybrid orthosis. A multicenter controlled study. II: physiological evaluation. Paraplegia 1995; 33: 654–659.
Kawashima N, Sone Y, Nakazawa K, Akai M, Yano H . Energy expenditure during walking with weight bearing control orthosis (WBC) in thoracic level of paraplegic patients. Spinal Cord 2003; 41: 506–510.
Nieman DC et al. The effects of moderate exercise training on natural killer cell and acute upper respiratory tract infections. Int J Sports Med 1990; 11: 467–473.
Nieman DC et al. Moderate exercise training and natural killer cell cytotoxic activity in breast cancer patients. Int J Sports Med 1995; 16: 334–337.
Nene AV, Patrick JH . Energy cost of paraplegic locomotion using the parawalker electrical stimulation hybrid orthosis. Arch Phys Med Rehabil 1990; 71: 116–120.
Janssen TW, van Oers CA, Rozendaal EP, Willemsen EM, Hollander AP, van der Woude LH . Changes in physical strain and physical capacity in men with spinal cord injuries. Med Sci Sports Exerc 1996; 28: 551–559.
Klokker M, Mohr T, Kjaer M, Galbo H, Pedersen BK . The natural killer cell responses to exercise in spinal cord injured individuals. Eur J Appl Physiol 1998; 79: 106–109.
Yano H . Weight bearing control orthosis for paraplegics. Organized session. 33rd Annual Scientific Meeting International Medical Society of Paraplegia: Monograph 1994, pp 1–16.
Yano H, Kaneko S, Nakazawa K, Yamamoto S, Bettoh A . A new concept of dynamic orthosis for paraplegia: the weight bearing control (WBC) orthosis. Prosthetics Ortho Int 1997; 21: 222–228.
Bernardi M, Canale I, Castellano V, Di Filippo L, Felici F, Marchetti M . The efficiency of walking of paraplegic patients using a reciprocating gait orthosis. Paraplegia 1995; 33: 409–415.
Massucci M, Brunetti G, Piperno R, Betti L, Franceschini M . Walking with the advanced reciprocating gait orthosis (ARGO) in thoracic paraplegic patients: energy expenditure and cardiorespiratory performance. Spinal Cord 1998; 36: 223–227.
Acknowledgements
This work was supported by Research Grants from the Mitsui Sumitomo Insurance Welfare Foundation.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Kawashima, N., Nakazawa, K., Ishii, N. et al. Potential impact of orthotic gait exercise on natural killer cell activities in thoracic level of spinal cord-injured patients. Spinal Cord 42, 420–424 (2004). https://doi.org/10.1038/sj.sc.3101625
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101625
Keywords
This article is cited by
-
Does 20-min arm crank ergometer exercise increase plasma interleukin-6 in individuals with cervical spinal cord injury?
European Journal of Applied Physiology (2012)
-
Impaired immune response to voluntary arm-crank ergometer exercise in patients with cervical spinal cord injury
Spinal Cord (2010)
-
Effect of lesion level on the orthotic gait performance in individuals with complete paraplegia
Spinal Cord (2006)
