
Abstract
Study design: Comparative study of the effectiveness of walking exercise with a newly developed gait orthosis, the weight-bearing control (WBC) orthosis, for thoracic level of paraplegic patients.
Objectives: To test its feasibility as a rehabilitation alternative for paraplegic patients, the energy consumption and cost during walking with WBC were calculated and compared with the values of conventional orthoses given in previous reports.
Setting: National Rehabilitation Center for the Disabled, Japan.
Methods: Four paraplegic patients with traumatic spinal cord injuries ranging from T8 to T12 participated. Experiments were conducted after 3 months of the orthotic gait training with WBC. The cardiorespiratory parameters were continuously measured at rest and during walking with a telemetric device. The steady-state value of the oxygen uptake (), heart rate (HR), the energy consumption (J/kg/s) and energy cost (J/kg/m) were calculated.
Results: The average walking speed was 19.0±2.58 m/min. The steady-state value of the and HR were 16.08±1.93 ml/kg and 147.3±10.94 b/min, respectively. The energy cost during orthotic walking tended to be better than the values of conventional orthoses, whereas the energy consumption was almost similar.
Conclusion: WBC enables thoracic level of paraplegic patients to walk at relatively higher speed than conventional orthoses under similar energy expenditure. The special devices equipped with WBC are therefore considered to lead to improvement of the energy cost of walking. The physical intensity presumed by cardiorespiratory responses during walking with WBC is suited to promote their aerobic capacity. Therefore, it is concluded that the WBC orthosis could be an effective alternative in rehabilitation for thoracic level of paraplegic patients.
Similar content being viewed by others

Introduction
Previous studies have pointed out that the high energy cost has been one of the major problems of the orthotic gait for paraplegic patients.1,2,3,4,5 Although many devices have been developed to improve this problem to date, it is still difficult to satisfy the requirements of both paraplegic patients and therapists. The futile energy cost should lead to exhaustion in a few minutes of walking. As a consequence, orthotics are frequently abandoned after being used for only a short time in therapeutic phase.6 Especially for thoracic level of paraplegic patients, a considerable effort of their upper limb and trunk above the paralysis is required during orthotic gait, and this is the main reason of the limitation of the orthotic use.2,7
One of the major purposes of the orthotic gait for paraplegic patients is the promotion of their health. Since previous studies have suggested the positive effects of walking exercise on secondary disorders, such as the urodynamics8 and digestive functions,9 paraplegic patients should make efforts to facilitate their own physical activities in daily life not only with a wheelchair, but also with walking exercise. To this end, the energy cost of orthotic gait should be lowered. Then, the users also need to make an appropriate level of physical intensity to promote their aerobic capacity with walking.
The weight-bearing control (WBC) orthosis was based on the concept to allow more dynamic reciprocal gait pattern for patients, especially those who could not swing their leg voluntarily.10,11,12 This orthosis has a reciprocal guide assistance and movable foot plates, which facilitate leg swing and make a clearance between the foot's sole and the floor, respectively. We hypothesized that the special devices equipped with the WBC orthosis would enable thoracic level of paraplegic patients to walk easily with less effort. To ascertain this hypothesis, energy consumption and cost of walking with WBC orthosis were evaluated and compared with other types of orthoses in previous reports.
Methods
Subjects
Four traumatic spinal cord injury patients who satisfied the following criteria were selected: (1) age <30 years, (2) with a thoracic level injury and (3) postinjury time of >6 months. All of them were male, ages ranging from 21 to 28 years (mean 24.5 years). One subject had an incomplete spinal cord injury grade B according to the ASIA scale at a T12 level, other subjects had complete injuries grade A with lesion levels varying from T8 to T12 (details are listed in Table 1). None of the subjects had any symptoms related to cardiopulmonary function. Subjects gave their informed consent to the experimental procedure. Each subject had completed a standard rehabilitation program, which included muscle strengthening, taking the orthosis on and off, balancing in a standing position, after which, they had practiced the gait training with the WBC orthosis. After this training program, each subject could perform the orthotic gait smoothly and was able to walk continuously at least for 20 min.
WBC orthosis
This device was developed for thoracic level of paraplegic patients to walk independently with less effort. It aims to take appropriate physical intensity considering the following major needs: a rigid frame that supports the user's body weight, a special hip joint devise that reciprocally propels each leg forward, a gas-powered foot device that varies the sole thickness of the device for foot/floor clearance, and a control system of the orthosis.
Experiment procedure
The cardiorespiratory parameter at rest and during walking was measured continuously with a telemetric device (K4 Cosmed, Italy). This device consists of a transmitting unit, a face mask to sample expired gas, a heart rate (HR) chest strip, a battery and a receiving unit. The experimental procedure was: 5 min at rest in the sitting position, 20 min of continuous walking at the most comfortable speed on a field. During walking, data were continuously acquired and analyzed in real time. The following cardiorespiratory parameters were acquired: oxygen uptake () and HR. Walking speed in the steady state during walking was also recorded. The measurements were conducted at 3 months after the onset of training. After the experiments, the energy consumption and walking energy cost were calculated. The terms adopted were those of Nane and Patrick3 and calculations performed according to their protocol:

where K=20.19 J/ml, since 1 ml O2=4.825 cal and 1 cal=4.184 J.
Results
All subjects could walk continuously without exhaustion and stumbling throughout the walking session for 20 min. They did not take a break except for the time of direction converting. The total distance traveled in 20 min was 269±32 m. The average walking speed with WBC was 19±2.58 m/min.
Table 2 shows the cardiorespiratory responses at rest and during orthotic gait. During walking, cardiorespiratory parameters clearly showed a significant increase compared with resting rate. The steady-state value of the was ranged from 14.20 to 18.05 ml/kg (average value=16.08±1.93 ml/kg), and HR was 132.9–157.3 b/min (average value=147.3±10.94 b/min).
Table 3 shows the energy consumption and energy cost. The energy consumption during walking was about three times greater than during rest (rest versus exercise: 1.99±0.40 versus 5.41±0.65 J/kg/s). The average value of the energy cost during walking was 17.12±0.72 J/kg/m.
Table 4 summarized the value of the energy consumption, energy cost and walking speed in previous reports using reciprocating gait orthosis, that is, HGO, RGO and ARGO. While the energy consumption during walking with WBC was slightly larger than that in previous report (median value=4.37 J/kg/s), the energy cost tended to be better than the value of previous reports (present versus previous: 17.12 versus 21.16 J/kg/m).
Discussion
The present results show that the energy cost during walking with WBC was better than the values given in previous reports of conventional orthoses, such as HGO, RGO and ARGO for thoracic level of paraplegic patients (Table 4). In the following discussion, our results of energy consumption and cost will be compared with previous reports. Then, the feasibility of the walking with WBC as the rehabilitation alternatives for thoracic level of paraplegic patients will be discussed.
Since the pioneering study by Gordon and Vanderwalde,1 many researchers have reported extremely higher energy requirements of orthotic gait.2,3,4,5,6,7 Although paraplegic patients with high thoracic level lesions found it difficult to achieve orthotic gait in the early stages of researches,13 later improvement enabled them to walk independently and reciprocally.4,5,14 However, the high energy cost is still the major reason for the limitation of the orthotic use.4,5 As Waters et al15 pointed out, there was a high correlation between the lower extremity muscle scores and the energy cost of the orthotic walking. Actually, considerable effort of their upper limb and trunk above the paralysis is required to accomplish walking for thoracic level of paraplegic patients.3,7 This loss of the energy expenditure prevents the achievement of aerobic condition during orthotic gait. To promote general health for paraplegic patients, it is necessary to facilitate aerobic condition. In this vein, the decrement of the energy cost is the primary problem.
WBC was designed on the concept of allowing more dynamic reciprocal gait pattern for patients, especially those who could not swing their leg voluntarily.10,11,12 Figure 1 shows the relation between the energy consumption and energy cost in each previous investigation.3,4,5,7,14,16,17,18 Since the walking speed was delivered to divide the energy consumption by the energy cost, the slope of line from zero to each plot reflects the walking speed of each orthosis. This figure clearly shows that the WBC enables paraplegic patients to walk at relatively higher speed than other reports under almost relatively lower energy cost. It is considered that the special devices equipped with WBC would lead to the improvement of energy cost. As mentioned above, it needs both of lower energy cost and adequate energy consumption to acquire an aerobic conditioning. To this end, those on the upper and left side of the figure can be considered as having suitable physical intensity for patients.

The relation between the energy consumption and cost in each investigations
It is well known that paraplegic patients have significantly reduced peak values as a consequence of the reduction in the daily activity levels.19 In addition, the isolation of the upright standing and walking should lead to various secondary disorders, for example, the decrement of the bone mineral density20,21 and malfunction of the peripheral circulation in paralyzed areas.22 Although there is little agreement of the effect on the above point, there is no doubt that some purposeful effects should be offered by orthotic gait. Previous studies have demonstrated that orthotic gait provides some benefits to the physical functions for paraplegic patients, such as the improvement of the urodynamics8 and digestive functions.9 Therefore, paraplegic patients should make efforts to facilitate their own physical activities in daily life, not only with wheelchair but also walking. Today, the benefits of walking exercise for paraplegic patients are well recognized. However, there are several obstacles in achieving locomotion for paraplegic patients. As we have mentioned, conventional gait orthoses require a very high energy expenditure that usually leads to exhaustion in a few minutes of walking.
In this study, we investigated the energy expenditure and energy cost during orthotic walking with WBC, and showed that paraplegic patients could walk at relatively higher speed and lower energy cost compared with the conventional orthoses. Using WBC, all of our subjects could walk more than 20 min without exhaustion at the end of their training period. Further, the physical intensity presumed by the cardiorespiratory responses was considered to be suited to promote their general health. It is therefore concluded that the WBC orthosis could be an effective alternative in rehabilitation for thoracic level of paraplegic patients to promote their health conditions. In further investigation, a more direct approach, such as the clinical or physiological evaluation, will be needed to clarify the effectiveness of the orthotic gait for paraplegic patients.
References
Gordon EE, Vanderwalde H . Energy requirements in paraplegic ambulation. Arch Phys Med Rehabil 1956; 37: 276–285.
Chantraine A, Crielaard JM, Onkelinx A, Pirnay F . Energy expenditure of ambulation in paraplegics: effects of long term use of bracing. Paraplegia 1984; 22: 173–181.
Nene AV, Patrick JH . Energy cost of paraplegic loco-motion using the parawalker-electrical stimulation ‘hybrid’ orthosis. Arch Phys Med Rehabil 1990; 71: 116–120.
Bernardi M et al. The efficiency of walking of paraplegic patientss using a reciprocating gait orthosis. Paraplegia 1995; 33: 409–415.
Massucci M et al. Walking with the advanced reciprocating gait orthosis (ARGO) in thoracic paraplegic patients: energy expenditure and cardiorespiratory performance. Spinal Cord 1998; 36: 223–227.
Solomonow M, Baratta RV, D'Ambrosia R . Standing and walking after spinal cord injury: experience with the reciprocating gait orthosis powered by electrical muscle stimulation. Top Spinal Cord Injury Rehabil 2000; 5: 29–53.
Hirokawa S et al. Energy consumption in paraplegic ambulation using the reciprocating gait orthosis and electric stimulation on the thigh muscles. Arch Phys Med Rehabil 1990; 71: 687–694.
Giannantoni A et al. Urodynamics in spinal cord injured patients walking with reciprocating gait orthosis. J Urol 2000; 164: 115–117.
Thoumie P et al. Restoration of functional gait in paraplegic patient with the RGO-II hybrid orthosis. A multicenter controlled study. II: physiological evaluation. Paraplegia 1995; 33: 654–659.
Yano H . Weight bearing control orthosis for paraplegics. Organized Session, 33rd Annual Scientific Meeting International Medical Society of Paraplegia: Monograph, 1994, pp 1–16.
Yano H et al. The rhythm and amplitude of the EMG activities of paralyzed muscle groups using a new style of walking orthosis for paraplegia. The eighth World Congress of the International Rehabilitation Medicine Association, International Proceedings Division, 1997, pp 1457–1463.
Yano H et al. A new concept of dynamic orthosis for paraplegia: the weight bearing control (WBC) orthosis. Prosthet Orthot Int 1997; 21: 222–228.
Miller NE, Merritt JE, Merkel KD, Westbrook PR . Paraplegic energy expenditure during negotiation of architectural barriers. Arch Phys Med Rehabil 1984; 65: 778–779.
Felici F et al. Rehabilitation of walking for paraplegic patients by means of a treadmill. Spinal cord 1997; 35: 383–385.
Waters RL, Adkins RH, Yakura JS, Vigil D . Prediction of ambulatory performance based on motor scores derived from standards of the American Spinal Injury Association. Arch Phys Med Rehabil 1994; 75: 756–760.
Winchester PK et al. A comparison of paraplegic gait performance using two types of reciprocating gait orthoses. Prosthet Orthot Int 1993; 17: 101–106.
Nane AV, Patrick JH . Energy cost of paraplegic locomotion with the ORLAU ParaWaker. Paraplegia 1989; 27: 5–18.
Merati G et al. Paraplegic adaptation to assisted-walking: energy expenditure during wheelchair versus orthosis use. Spinal Cord 2000; 38: 37–44.
Janssen TW et al. Changes in physical strain and physical capacity in men with spinal cord injuries. Med Sci Sports Exerc 1996; 28: 551–559.
Frey-Rindova P et al. Bone mineral density in upper and lower extremities during 12 months after spinal cord injury measured by peripheral quantitative computed tomography. Spinal Cord 2000; 38: 26–32.
Szollar SM et al. Bone mineral density and indexes of bone metabolism in spinal cord injury. Am J Phys Med Rehabil 1998; 77: 28–35.
van Beekvelt MCP, van Asten WNJC, Hopman MTE . The effect of electrical stimulation on leg muscle pump activity in spinal cord-injured and able-bodied individuals. Eur J Appl Physiol 2000; 82: 510–516.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Kawashima, N., Sone, Y., Nakazawa, K. et al. Energy expenditure during walking with weight-bearing control (WBC) orthosis in thoracic level of paraplegic patients. Spinal Cord 41, 506–510 (2003). https://doi.org/10.1038/sj.sc.3101494
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101494
Keywords
This article is cited by
-
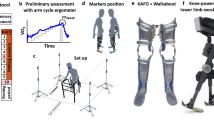
Comparing walking with knee-ankle-foot orthoses and a knee-powered exoskeleton after spinal cord injury: a randomized, crossover clinical trial
Scientific Reports (2022)
-
Stair-ascent strategies and performance evaluation for a lower limb exoskeleton
International Journal of Intelligent Robotics and Applications (2020)
-
The influence of orthosis options on walking parameters in spinal cord-injured patients: a literature review
Spinal Cord (2016)
-
Comparison of new medial linkage reciprocating gait orthosis and isocentric reciprocating gait orthosis on energy consumption in paraplegic patients: a case series
Spinal Cord Series and Cases (2015)
-
The effect of ankle joint mobility when using an isocentric reciprocating gait orthosis (IRGO) on energy consumption in people with spinal cord injury: preliminary results
Spinal Cord Series and Cases (2015)
