
Abstract
The purpose of the present study was to determine whether positron emission tomography (PET) studies in monkeys with the dopamine (DA) D2 receptor ligand [18F]fluoroclebopride (FCP) would be significantly influenced by anesthetic induction with isoflurane (∼5.0%) compared to induction with 10 mg/kg ketamine. Five experimentally-naive adult male cynomolgus monkeys (Macaca fascicularis) were trained to sit calmly in a primate restraint chair. Before the first PET scan, each monkey was anesthetized, by mask, with isoflurane. After complete sedation, the monkey was intubated and anesthesia was maintained throughout the PET study by isoflurane (∼1.5%). At least 1 month later, a second PET study was conducted in which anesthesia was induced with ketamine and maintained by isoflurane (∼1.5%). Irrespective of induction anesthetic, there was a high uptake of [18F]FCP and a linear rate of washout from the basal ganglia for all monkeys. There were also no differences in time to peak uptake (∼25 min), in clearance half-life (t1/2 = 140–164 min) or in D2 binding (distribution volume ratios of 2.48 vs. 2.50). These results indicate that induction anesthetic did not differentially affect D2 binding of [18F]FCP in monkeys. Furthermore, the low variability between studies indicates that [18F]FCP is an excellent ligand for longitudinal studies of D2 receptors in nonhuman primates.
Similar content being viewed by others
Main
The dopamine (DA) system has been implicated in the etiology and maintenance of many affective disorders (see reviews by Baldessarini 1997; Efange and Mach 1993; Jaber et al. 1996). Receptors within the dopamine system have been divided into two families, D1 and D2 receptors, based on anatomic and functional criteria (Kebabian and Calne 1979). Much in vivo research on the central mechanisms of these disorders has been conducted using positron emission tomography (PET) and radioligands selective for the D2 receptor subtype (see Efange and Mach 1993). For example, there is evidence of differences in postsynaptic D2 receptor density in individuals suffering from schizophrenia (Pearlson et al. 1995; Seeman 1987; Tune et al. 1993; Wong et al. 1986, 1997), Parkinson's disease (Hagglund et al. 1986; Rinne et al. 1990) and cocaine abuse (Volkow et al. 1990, 1993), as compared to age-matched controls.
Currently, much of the PET D2 receptor imaging research has utilized animal models, because they allow the subject's environment to be strictly controlled and interventions to be made that are not otherwise allowable in humans. In the majority of these studies, anesthesia is required to prevent the animal from moving during the imaging period. A common part of the anesthetic protocol is the use of ketamine as a pre-anesthetic to sedate the animal for transport to the imaging facility and to allow anesthesia to be induced. There is, however, some controversy regarding the effects of ketamine on the dopamine system. In a recent PET study in human subjects, a subanesthetic dose of ketamine (0.5 mg/kg, IV) decreased dopamine receptor availability as determined by [11C]raclopride binding (Smith et al. 1998). The investigators concluded that ketamine increased striatal dopamine concentrations, which resulted in decreased binding of [11C]raclopride to D2 receptors. In other experiments using animals, ketamine has been shown to increase DA release (e.g., Irifune et al. 1997; Keita et al. 1996; Lindefors et al. 1997; Moghaddam et al. 1997) or to have no significant effect on striatal levels of DA (e.g., Bacopoulos et al. 1979; Mantz et al. 1994; Torres et al. 1994).
The goal of the present study was to evaluate the effects of ketamine induction on D2 receptor binding in monkeys. The ligand used was fluoroclebopride (FCP), an F-18 labeled ligand of the D2 receptor, which we have previously demonstrated to be effective in imaging studies in nonhuman primates (Grant et al. 1998; Mach et al. 1996, 1997). In this study, the within-subject effects of ketamine- vs. isoflurane-induced anesthesia on D2 receptor density were examined in five monkeys. We found that the variability between studies was extremely low, indicating that ketamine induction did not influence D2 binding of [18F]FCP.
METHODS
Subjects
Five experimentally-naive adult male cynomolgus monkeys (Macaca fascicularis) served as subjects. Body weights of all monkeys were maintained at approximately 95% of their free-feeding weight by daily feeding of Purina Monkey Chow (range of weights were 3.23 to 5.21 kg). Monkeys were weighed each week and, if necessary, their diet (100 to 120 g/day) was adjusted to maintain stable weights. In addition, monkeys were given a chewable multiple vitamin tablet and fresh fruit 3 days/week; water was always available in the home cage.
Experimental Procedure
Each monkey was fitted with a nylon collar (Model B008, Primate Products, Redwood City, CA) and trained to approach the front of the cage when the investigator was present. A stainless steel rod (Model R011, Primate Products), with a latch on the end, was attached to the collar and the monkey was guided into the monkey chair. Within 3 weeks of training, monkeys sat calmly in the primate restraint chair for approximately 20 to 30 min each day. Next, each monkey was acclimated to having an anesthesia mask placed over its face by rewarding it with Tang solution after several seconds of mask placement. This procedure was conducted daily, with the amount of time that the mask remained on the face gradually increasing to approximately 1 min. Within 1 week of training, all monkeys remained calm during this procedure.
PET Study 1: Isoflurane Induction
For the first PET study (Study 1), each monkey was removed from its home cage, placed into a single cage, and transported to the animal holding room of the PET Center on the day before the study. Before the start of the PET study, the monkey was placed in a primate chair, and anesthesia was induced with 4 to 5% isoflurane (in O2) by placing an anesthesia mask over the monkey's face. Once sedated, the monkey was removed from the primate chair, intubated (∼3.5-mm endotrachea tube), and maintained on ∼1.5% isoflurane anesthesia throughout the procedure.
The monkey was then placed in the PET scanner, and its head was positioned within the scanner. During the scan, the temperature of the monkey was maintained through the use of a heating pad (temperature of the circulating water = 40°C). The following vital signs were monitored throughout the scanning procedure: heart rate, blood pressure, respiration, and body temperature. Arterial blood gases were monitored periodically for PO2 and PCO2 levels by testing blood samples using an Instrumentation Laboratory Model 1306 pH/Blood Gas Analyzer.
PET Study 2: Ketamine Induction
For the second PET scan (Study 2), which occurred at least 1 month after Study 1, each monkey was anesthetized with 10 mg/kg ketamine, transported to the PET Center, intubated, and maintained on isoflurane anesthesia (∼1.5%) for the remainder of the study. Maintenance of anesthesia by isoflurane occurred within 30 min of ketamine induction, and the PET scan started approximately 2 h after ketamine administration. All other procedures were identical to those described above for Study 1.
PET Procedures
Once the monkey was anesthetized and placed into the PET scanner, catheters (22-gauge angiocath; Becton Dickinson Vascular Access, Sandy, UT) were placed in an external artery and vein by percutaneous sticks, and fluids were delivered to the monkey (approximately 12 drops/min, lactated Ringer's solution, IV) throughout the study. To ensure that the monkey did not move during the PET study, a paralytic (0.07 mg/kg vecuronium Br, IV) was administered, and respiration was maintained on a ventilator. Supplemental doses of vecuronium Br (0.1 mg/h) were administered throughout the study.
All PET scans were performed with a Siemens/CTI ECAT 951/31 PET scanner. This imaging device has 16 contiguous detector rings that provide 31 image planes with a slice thickness approximately equal to 3.4 mm. The Bismuth Germanate (BGO) block detector architecture of the scanner provides a measured resolution full width at half maximum (FWHM) in the center of the field of view (FOV) of 5.6 × 5.6 mm in the radial and tangential directions and 5.5 mm axially, to about 6.0 to 6.5 mm, 10 cm from the center.
The synthesis of [18F]FCP was accomplished via N-alkylation of the corresponding des-benzyl precursors with [18F]-fluorobenzyliodide, as previously described (Mach et al. 1993a, b). At the start of the scan, approximately 4 mCi of [18F]FCP was injected, followed by 3 ml of heparinized saline. At appropriate times, arterial blood samples were withdrawn and placed into preheparinized minicentrifuge tubes for analysis (as described in detail in Mach et al. 1996). Images were taken for the following time frames: 5 × 1 min, 5 × 2 min, 5 × 5 min, 8 × 10 min, and 3 × 20 min. The completed scan contained a total of 26 frames over 180 min. Regions of interest were drawn over the basal ganglia and cerebellum, and tissue-time activity curves were constructed by plotting the percentage injected dose per cubic centimeter of tissue (%i.d./cc) vs. time post IV injection of radiotracer. The distribution volume (DV) for the basal ganglia and cerebellum was determined using the graphic technique of Logan et al. (1990). The linear portion of the Logan plot was used to determine the DV for each region, which in all cases included the last 80 min of the scan (five frames). The ratio of the DV for the basal ganglia and the cerebellum, the distribution volume ratio (DVR), was used as a metric of specific binding and is related to the binding potential (Mintun et al. 1984) by the formula DVR − 1 = binding potential (Logan et al. 1990). The basal ganglia:cerebellum ratio was calculated by dividing the %i.d./cc of the basal ganglia by the value obtained from the cerebellum.
Statistical Analysis
Data are presented for each subject and as group means (±SEM). Paired t-tests were used to determine differences between PET studies with isoflurane- and ketamine-induced anesthesia (Study 1 vs. Study 2), with p < .05 defined as statistically significant. For measures of time to peak uptake (Table 1), the group value represents the time in which the overall mean for %i.d.cc tissue was maximal.
RESULTS
Mean body weights for the five monkeys were not significantly different (t[4] = 1.75, p > .15) between Study 1 (4.34 kg) and Study 2 (4.55 kg). There were no significant differences in the dose of FCP injected during the first and second studies (t[4] = 0.34, p > .74), with mean values of 3.58 mCi and 3.47 mCi, respectively. On average, there were approximately 55 days (range = 35 to 75 days) between the isoflurane- and ketamine-induced anesthesia PET studies.
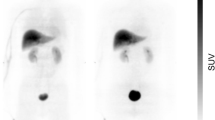
Mean tissue–time activity curves for the basal ganglia (BG) and cerebellum (Cb), the two regions of interest, from the first PET study (n = 5 monkeys) are shown in Figure 1 (top panel, closed symbols). For all monkeys initially anesthetized with 5% isoflurane and maintained on 1.5% isoflurane (Study 1), there was a high uptake of [18F]FCP and a linear rate of washout from the BG, a region with a high density of D2 receptors. Uptake of [18F]FCP in the Cb, a region devoid of D2 receptors, was lower, and the rate of washout was faster than that observed in the BG. When the monkeys were initially anesthetized with 10 mg/kg ketamine (Study 2) before the PET study (Figure 1, top panel, open symbols), there were no apparent differences in tissue–time activity curves compared to the first PET scan.

Tissue-time activity curves (top panel) of [18F]FCP in basal ganglia (circles) and cerebellum (triangles) and the basal ganglia:cerebellum ratios (bottom panel) of [18F]FCP for cynomolgus monkeys initially anesthetized with isoflurane (Study 1; filled symbols) or 10 mg/kg ketamine (Study 2; open symbols). Each point is the mean of data from five monkeys
Normalized peak uptake values (%i.d./cc), postinjection time at which peak uptake occurred and linear half life (t1/2) clearance rates from the BG were determined from the mean tissue–time activity curves. For PET Study 1, the average peak uptake in the BG occurred at about 27.5 min postinjection (Table 1), with a mean normalized peak uptake value of approximately 0.085 (±0.012)%i.d./cc tissue for all test studies. Only monkey 5397 had peak uptake in the striatum later than 27.5 min. In Study 1, [18F]FCP cleared from the BG in a linear manner, with a t1/2 of 140.20 (±6.99) min (Table 1). The between-subject range of washout was 123 to 160 min. When retested with ketamine induction (Study 2), the average peak uptake in the BG occurred at approximately 27.5 min postinjection (Table 1), with a mean normalized uptake value of approximately 0.082 (±0.005)%i.d./cc tissue. In Study 2, the linear rate of washout of [18F]FCP from the BG had a t1/2 of 164.20 (±15.7) min (Table 1), with a between-subjects range of 132 to 215 min. There were no statistically significant differences between Study 1 and Study 2. The time of peak uptake was later in Study 2 as compared to Study 1 in three of the five monkeys, although the %i.d./cc tissue values were not significantly different between the studies (t[4] = 0.10, p > .92). Although there was a trend for higher t1/2 values following ketamine induction (Study 2) as compared to isoflurane induction (Study 1), these differences were not statistically significant (t[4] = 2.51, p > .06).
The mean BG:Cb distribution volume ratio (DVR) of [18F]FCP for Study 1 was 2.48 (±0.12), with a between-subject range of 2.29 to 2.89 ( Table 2). The mean DVR of [18F]FCP for Study 2 was 2.50 (±0.10), with a between-subject range of 2.27 to 2.83 (Table 2). Direct comparisons between Study 1 and Study 2 revealed within-subject variability of DVRs of approximately 2%; these differences were not statistically significant (t[4] = 0.64, p > .55). Graphical representation of BG:Cb time activity curve ratios for the isoflurane- and ketamine-induced anesthesia studies is shown in Figure 1 (bottom panel). As reported previously for this ligand (Mach et al. 1996), the rapid rate of washout of [18F]FCP from the BG and Cb resulted in a high BG:Cb ratio, reaching a peak value of 3.46 (±0.31) at approximately 65 min postinjection in Study 1, when anesthesia was induced by isoflurane. In Study 2, the mean peak BG:Cb ratio was 3.42 (±0.22) at 65 minutes postinjection. There were no statistically significant differences in the BG:Cb ratios (t[4] = 0.23, p > .82) between Study 1 and Study 2. Arterial plasma radioactivity curves and metabolite corrected plasma curves were not significantly different between the first and second PET studies (data not shown) and are similar to data reported previously for this ligand (Mach et al. 1996).
DISCUSSION
The use of PET imaging has allowed for the systematic study of changes in receptor density or function in the same subject over long periods of time (e.g., Dewey et al. 1993; Mach et al. 1997; Volkow et al. 1993). The primary goal of the present study was to compare the effects of inducing anesthesia with ketamine (10 mg/kg) vs. inducing anesthesia with isoflurane (∼5.0%) in monkeys. We found no statistically significant differences in [18F]FCP binding to D2 receptors attributed to the method of anesthesia induction (ketamine vs. isoflurane). Furthermore, the variability between the two studies was approximately 2%, indicating that this ligand is ideal for labeling D2 receptors.
Previous research has shown that ketamine anesthesia can affect D2 binding in PET studies. For example, the effects of ketamine anesthesia on N-[11C]methylspiperone (NMSP) binding were examined in rhesus monkeys (Onoe et al. 1994). In that study, monkeys were placed into a specially designed primate restraint chair that allowed PET studies to be conducted while the animals were awake. The investigators found that 5 mg/kg ketamine, administered 30 min before the start of the PET study, increased the binding for [11C]NMSP as compared to values in conscious monkeys. There were no differences in NMSP uptake in the cerebellum, indicating that blood flow changes could not account for their results. These results are in contrast to the findings of the present study, in which ketamine had no effect on [18F]FCP binding in cynomolgus monkeys. The most likely explanation for the discrepant results involves the study of conscious monkeys by Onoe et al. (1994). The higher binding of [11C]NMSP in the ketamine-treated monkeys as compared to the conscious monkeys may be attributable to higher levels of stress in the latter group, which may have elevated levels of DA in the striatum (see Cabib and Puglisi-Allegra 1996 for review). Increases in synaptic DA levels would be consistent with a decrease in binding (e.g., Mach et al. 1997). Unfortunately, no measures of stress, such as cortisol levels, were reported, which would have provided an interpretation for this discrepancy.
A second possible explanation for the different results of Onoe et al. (1994) as compared to the present findings may involve the radioligands used to label D2 receptors. Compared to FCP, NMSP is less selective for D2 receptors, also binding with high affinity to the serotonin 5-HT2 receptor (Leysen et al. 1978). Ketamine has been shown to decrease the concentration of the 5-HT metabolite 5-hydroxyindoleacetic acid (5-HIAA) in the striatum of rodents (Irifune et al. 1997), which may have contributed to the elevated NMSP binding reported by Onoe et al. (1994). Consistent with this observation was the finding that [11C]-NMSP binding in the striatum of monkeys was higher when anesthesia was maintained by ketamine versus isoflurane (Kobayashi et al. 1995).
The present results can also be contrasted with recent PET studies that have examined the effects of ketamine on D2 receptor binding in humans (Breier et al. 1998; Smith et al. 1998). In the Smith et al. (1998) study, two groups of subjects were scanned twice in one day: an initial baseline scan and a second scan following administration of a subanesthetic dose of ketamine (0.5 mg/kg, IV), administered over 20 min. In one group, ketamine was injected immediately before the start of the PET study, whereas in the second group, [11C]raclopride was injected 10 min into the ketamine infusion, and the ketamine infusion continued for the initial 10 min of the PET study. For both groups, the distribution volume in the striatum was significantly lower following ketamine, as compared to the baseline levels. In the Breier et al. (1998) study, a bolus infusion imaging protocol was used with [11C]raclopride. The results of this study revealed an 11% reduction in D2 receptor binding, which is consistent with a decrease in D2 receptor availability caused by an elevation of synaptic DA levels. However, the possibility that the subanesthetic doses of ketamine were stressful to the human subjects cannot be ruled out, because ketamine significantly increased cortisol levels (Smith et al. 1998) and resulted in a significant elevation in positive (i.e., “psychotic”) and negative (i.e., blunted affect) symptom scores (Breier et al. 1998) as determined by the Brief Psychiatric Rating Scale (BPRS).
Another possibility for the discrepant results between the two recent human studies and the present findings may involve the sensitivity of the radioligands to extracellular DA levels. However, both raclopride and FCP have reversible binding kinetics at D2 receptors, so that the binding is influenced by fluctuations in extracellular DA levels (e.g., Dewey et al. 1992; 1993; Mach et al. 1997). For example, administration of indirect acting DA agonists, such as d-amphetamine or cocaine, increased the rate of washout of [18F]FCP from the basal ganglia of rhesus monkeys, indicating that the binding of FCP is influenced by synaptic DA levels (Mach et al. 1997). Thus, the lack of effect of ketamine in the present study cannot be attributed to an inability of synaptic DA to compete with FCP for D2 receptors. Taken together, these findings suggest that the most likely explanation for the differences in results between the present study and the previous human studies (Breier et al. 1998; Smith et al. 1998) involves when the ketamine was administered in relation to the start of the PET study.
Although the present results suggest that ketamine anesthesia does not differentially affect [18F]FCP binding compared to anesthesia induced by isoflurane, it should be pointed out that a systematic study of ketamine's effects on D2 binding was not conducted. Others have shown that under much more extreme conditions, 8-day treatment with the NMDA antagonist dizocilpine enhanced DA turnover (Reith et al. 1998), thereby suggesting that the dopaminergic system can be modified by long-term NMDA blockade. The primary goal of the present study was to determine whether, under the conditions employed, induction by ketamine would differentially affect our PET results. Only one dose of ketamine was examined (10 mg/kg), and it was administered approximately 2 h before the start of the PET study. PET studies in baboons using [11C]-ketamine reported a high uptake into the brain with a rapid washout from the striatum and cerebellum (Shiue et al. 1997). In microdialysis studies in rodents, ketamine elevated striatal DA levels in a time-dependent manner, with peak values occurring at 20 to 60 min after ketamine administration and returning to control values within 140 min (Lindefors et al. 1997). Thus, it is possible that if ketamine were given closer to the start of the PET study, differences between induction methods would have been observed.
In summary, the present findings add to a growing body of evidence that [18F]FCP is an excellent PET radiotracer for the study of D2 receptors in nonhuman primates. Previous results have shown that [18F]FCP has a low between-subject variability (Grant et al. 1998; Mach et al. 1996), which was replicated in the present study. The present results extended these findings to show that, under the conditions used in this experiment, ketamine-induced anesthesia does not significantly influence [18F]FCP binding to D2 receptors compared to anesthesia induced by isoflurane. Although the present experiment did not specifically evaluate the test–retest variability of FCP, the low between-study variability indicates that this ligand should be an excellent PET radiotracer for the longitudinal study of changes in D2 receptors in nonhuman primate models of disease.
References
Bacopoulos NG, Redmond DE, Roth RH . (1979): Serotonin and dopamine metabolites in brain regions and cerebrospinal fluid of a primate species: Effects of ketamine and fluphenazine. J Neurochem 32: 1215–1218
Baldessarini RJ . (1997): Dopamine receptors and clinical medicine. In Neve KA, Neve RL (eds), The Dopamine Receptors. Totowa, NJ, Humana Press Inc, pp 457–498
Breier A, Adler CM, Weisenfeld N, Su T-P, Elman I, Picken L, Malhotra AK, Pickar D . (1998): Effects of NMDA antagonism on striatal dopamine release in healthy subjects: Application of a novel PET approach. Synapse 29: 142–147
Cabib S, Puglisi-Allegra S . (1996): Stress, depression, and the mesolimbic dopamine system. Psychopharmacology 128: 331–342
Dewey SL, Smith GS, Logan J, Brodie JD, Yu DW, Ferrieri RA, King PT, MacGregor RR, Martin TP, Wolf AP, Volkow ND, Fowler JS, Meller E . (1992): GABAergic inhibition of endogenous dopamine release measured in vivo with 11C-raclopride and positron emission tomography. J Neurosci 12: 3773–3780
Dewey SL, Smith GS, Logan J, Brodie JD, Simkowitz P, MacGregor RR, Fowler JS, Volkow ND, Wolf AP . (1993): Effects of central cholinergic blockade on striatal dopamine release measured with positron emission tomography in normal human subjects. Proc Nat Acad Sci 90: 11816–11820
Efange S, Mach RH . (1993): In vivo detection of receptors. J Clin Immunoassay 16: 311–329
Grant KA, Shively CA, Nader MA, Ehrenkaufer RL, Line SW, Morton TE, Gage HD, Mach RH . (1998): The effect of social status on striatal dopamine D2 receptor binding characteristics in cynomolgus monkeys assessed with positron emission tomography. Synapse 29: 80–83
Hagglund J, Aquilonius S-M, Bergstron K, Eckernas S-A, Hartvig P, Lundqvist H, Langstrom B, Malmborg P, Nagren K . (1986): Regional kinetics of [11C]methylspiperone in the brain studies by positron emission tomography in patients with Parkinson's disease. Adv Neurol 45: 99–101
Irifune M, Fukuda T, Nomoto M, Sato T, Kamata Y, Nishikawa T, Mietani W, Yokoyama K, Sugiyama K, Kawahara M . (1997): Effects of ketamine on dopamine metabolism during anesthesia in discrete brain regions in mice: Comparison with the effects during the recovery and subanesthetic phases. Brain Res 763: 281–284
Jaber M, Robinson SW, Missale C, Caron MG . (1996): Dopamine receptors and brain function. Neuropharmacology 35: 1503–1519
Kebabian JW, Calne DB . (1979): Multiple receptors for dopamine. Nature 277: 93–96
Keita H, Lecharny JB, Henzel D, Desmonts JM, Mantz J . (1996): Is inhibition of dopamine uptake relevant to the hypnotic action of i.v. anaesthetics?. Br J Anaesth 77: 254–256
Kobayashi K, Inoue O, Watanabe Y, Onoe H, Langstrom B . (1995): Difference in response of D2 receptor binding between 11C-N-methylspiperone and 11C-raclopride against anesthetics in rhesus monkey brain. J Neural Transm 100: 147–151
Leysen JE, Niemgeers CJE, Tollenaere JP, Laduron PM . (1978): Serotonergic component of neuroleptic receptors. Nature 272: 168–171
Lindefors N, Barati S, O'Connor WT . (1997): Differential effects of single and repeated ketamine administration on dopamine, serotonin and GABA transmission in rat medial prefrontal cortex. Brain Res 759: 205–212
Logan J, Fowler JS, Volkow ND, Wolf AP, Dewey SD, Schlyer DJ, MacGregor RR, Hitzemann R, Bendriem B, Gatley SJ, Christman DR . (1990): Graphical analysis of reversible radioligand binding from time-activity measurements applied to [N-11C-methyl]-cocaine PET studies in human subjects. J Cerebral Blood Flow Metab 10: 740–747
Mach RH, Elder ST, Morton TE, Nowak PA, Evora PH, Scripko JG, Luedtke RR, Unsworth CD, Filtz T, Rao AV, Molinoff PB, Ehrenkaufer RLE . (1993a): The use of [18F]4-fluorobenzyliodide (FBI) in PET radiotracer synthesis: Model alkylation studies and its application in the design of dopamine D1 and D2 receptor-based imaging agents. Nucl Med Biol 20: 777–794
Mach RH, Luedtke RR, Unsworth CD, Boundy VA, Nowak PA, Scripko JG, Elder ST, Jackson JR, Hoffman PL, Evora PH, Rao AV, Molinoff PB, Childers SC, Ehrenkaufer RL . (1993b): 18F-labeled benzamides for studying the dopamine D2 receptor with positron emission tomography. J Med Chem 36: 3707–3720
Mach RH, Nader MA, Ehrenkaufer RLE, Line SW, Smith CR, Gage HD, Morton TE . (1997): Use of positron emission tomography to study the dynamics of psychostimulant-induced dopamine release. Pharmacol Biochem Behav 57: 477–486
Mach RH, Nader MA, Ehrenkaufer RLE, Line SW, Smith CR, Leudtke RR, Kung M-P, Kung HF, Lyons D, Morton TE . (1996): Comparison of two fluorine-18 labeled benzamide derivatives that bind reversibly to dopamine D2 receptors: In vitro binding studies and positron emission tomography. Synapse 24: 322–333
Mantz J, Varlet C, Lecharny JB, Henzel D, Lenot P, Desmonts JM . (1994): Effects of volatile anesthetics, thiopental, and ketamine on spontaneous and depolarization-evoked release of dopamine from striatal synaptosomes in the rat. Anesthesiology 80: 352–363
Mintun MA, Raichle ME, Kilbourn MR, Wooten GF, Welch MJ . (1984): A quantitative model for the in vivo assessment of drug binding sites with positron emission tomgoraphy. Ann Neurol 15: 217–227
Moghaddam B, Adams B, Verma A, Daly D . (1997): Activation of glutamatergic neurotransmission by ketamine: A novel step in the pathway from NMDA receptor blockade to dopaminergic and cognitive disruptions associated with the prefrontal cortex. J Neurosci 17: 2921–2927
Onoe H, Inoue O, Suzuki K, Tsukada H, Itoh T, Mataga N, Watanabe Y . (1994): Ketamine increases the striatal N-[11C]methylspiperone binding in vivo: Positron emission tomography study using conscious rhesus monkey. Brain Res 663: 191–198
Pearlson GD, Wong DF, Tune LE, Ross CA, Chase GA, Links JM, Dannals RF, Wilson AA, Ravert HT, Wagner HN Jr, DePaulo R . (1995): In vivo D2 dopamine receptor density in psychotic and nonpsychotic patients with bipolar disorder. Arch Gen Psychiat 52: 471–477
Reith J, Cumming P, Gjedde A . (1998): Enhanced [3H]DOPA and [3H]dopamine turnover in striatum and frontal cortex in vivo linked to glutamate receptor antagonism. J Neurochem 70: 1979–1985
Rinne JO, Laihinen A, Nagren K, Bergman J, Solin O, Haaparanta M, Ruotsalainen U, Rinne UK . (1990): PET demonstrates different behaviour of striatal dopamine D-1 and D-2 receptors in early Parkinson's disease. J Neurosci Res 27: 494–499
Seeman P . (1987): Dopamine receptors and the dopamine hypothesis of schizophrenia. Synapse 1: 133–152
Shiue C-Y, Vallabhahosula S, Wolf AP, Dewey SL, Fowler JS, Schlyer DJ, Arnett CD, Zhou Y-G . (1997): Carbon-11 labeled ketamine - synthesis, distribution in mice and PET studies in baboons. Nucl Med Biol 24: 145–150
Smith GS, Schloesser R, Brodie JD, Dewey SL, Logan J, Vitkun SA, Simkowitz P, Hurley A, Cooper T, Volkow ND, Cancro R . (1998): Glutamate modulation of dopamine measured in vivo with positron emission tomography (PET) and 11C-raclopride in normal human subjects. Neuropsychopharmacology 18: 18–25
Torres G, Rivier C, Weiss F . (1994): A ketamine mixture anesthetic inhibits neuroendocrine and behavioral consequences of cocaine administration. Brain Res 656: 33–42
Tune LE, Wong DF, Pearlson GD, Strauss ME, Young T, Shaya EK, Dannals RF, Wilson AA, Ravert HT, Sapp J, Cooper T, Chase GA, Wagner NH Jr . (1993): Dopamine D2 receptor density estimates in schizophrenia: A positron emission tomography study with 11C-methylspiperone. Psychiat Res 49: 219–237
Volkow ND, Fowler JS, Wolf AP, Schlyer D, Shiue C-Y, Alpert R, Dewey SL, Logan J, Bendriem B, Christman D, Hitzemann R, Henn F . (1990): Effects of chronic cocaine abuse on postsynaptic dopamine receptors. Am J Psychiat 147: 719–724
Volkow ND, Fowler JS, Wang G-J, Hitzemann R, Logan J, Schlyer DJ, Dewey SL, Wolf AP . (1993): Decreased dopamine D2 receptor availability is associated with reduced frontal metabolism in cocaine abusers. Synapse 14: 169–177
Wong DF, Wagner HN, Tune LE, Dannals RF, Pearlson GD, Links JM, Tamminga CA, Broussolle EP, Ravert HT, Wilson AA, Young TK, Malat J, Williams J, O'Tuama LA, Snyder SH, Kuhar MJ, Gjedde A . (1986): Positron emission tomography reveals elevated D2 dopamine receptors in drug-naive schizophrenics. Science 234: 1558–1563
Wong DF, Young D, Wilson PD, Meltzer CC, Gjedde A . (1997): Quantification of neuroreceptors in the living human brain. III. D2-like dopamine receptors: Theory, validation and changes during normal aging. J Cerebral Blood Flow Metab 17: 316–330
Acknowledgements
This study was supported by NIH grants DA-10584 and DA-08468 from the National Institute on Drug Abuse. The authors acknowledge the technical efforts of Nancy Buchheimer, Thomas Morton, Dr. Ann Line, Osric Prioleau, Amy Johnston, Clifford Hubbard, and Susan Nader. We also thank Dr. Drake Morgan, Rachna Sinnott, and Joshua Lile for comments on an earlier version of this manuscript. This research was carried out in accordance with the Declaration of Helsinki and with the Guide for the Care and Use of Laboratory Animals, as adopted by the NIH. The animal protocol was approved by the Wake Forest University Animal Care and Use Committee.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Nader, M., Grant, K., Gage, H. et al. PET Imaging of Dopamine D2 Receptors with [18F]Fluoroclebopride in Monkeys: Effects of Isoflurane- and Ketamine-Induced Anesthesia. Neuropsychopharmacol 21, 589–596 (1999). https://doi.org/10.1016/S0893-133X(98)00101-8
Received:
Revised:
Accepted:
Issue Date:
DOI: https://doi.org/10.1016/S0893-133X(98)00101-8
Keywords
This article is cited by
-
PET imaging of dopamine transporters and D2/D3 receptors in female monkeys: effects of chronic cocaine self-administration
Neuropsychopharmacology (2023)
-
Effects of social reorganization on dopamine D2/D3 receptor availability and cocaine self-administration in male cynomolgus monkeys
Psychopharmacology (2017)
-
Effects of repeated treatment with the dopamine D2/D3 receptor partial agonist aripiprazole on striatal D2/D3 receptor availability in monkeys
Psychopharmacology (2014)
-
Differences in D2 dopamine receptor availability and reaction to novelty in socially housed male monkeys during abstinence from cocaine
Psychopharmacology (2010)
-
Characterization of the dopamine receptor system in adult rhesus monkeys exposed to cocaine throughout gestation
Psychopharmacology (2010)
