
Abstract
Response to psychomotor stimulants is highly variable across individuals. Such inconsistencies are influenced by many factors including drug dose and polymorphic differences in genes that encode proteins, such as the dopamine transporter (DAT1), which are relevant to the site of action of these substances. The current study used a double blind, crossover (methylphenidate vs placebo) design to assess DAT1 genotype differences on appetite ratings to a snack-food cue in subjects with binge eating disorder (BED) (n=32) and healthy age-matched controls (n=46). ANOVA results indicated a significant genotype × diagnostic group interaction whereby BED subjects with at least one copy of the 9-repeat allele showed a significant suppression of appetite in response to methylphenidate compared with controls with this allele, or to subjects with the 10/10 genotype (irrespective of diagnosis) whose drug response was indistinguishable from placebo. The most probable explanation for these findings is that some, currently unknown, genetic variant, which is overrepresented in those with BED, interacts with DAT1 to suppress appetite in response to stimulant administration. The current findings have implications for treatment response to drugs currently in use (or being developed) for the treatment of overeating and overweight.
Similar content being viewed by others


INTRODUCTION
By most accounts, dopamine (DA) release in the nucleus accumbens (NAc) is both necessary for, and sufficient to promote, an appetitive/approach response to environmental cues that signal reward and that are contingent on carrying out a specific action to receive it (Nicola et al, 2005). More generally, the mesolimbic DA pathways regulate our emotional capacity to feel pleasure and our desire and motivation to seek out such experiences (Berridge, 2003). For example, inactivation of the ventral tegmental area (the major dopaminergic input to the striatum) abolishes neuronal firing in the NAc, and reward-seeking responses to a reinforcing stimulus-like food (Yun et al, 2004). These responses can also be reduced by administration of DA receptor antagonists (Nicola et al, 2005). On the other hand, a stimulant injection in the NAc potentiates DA release and reward-related behavioral responding (Zangen et al, 2006).
As with all biological systems, however, there is considerable response variability across individuals. In the case of the mesolimbic reward pathways, those with inherently higher levels of DA availability are likely to have a greater hedonic capacity and a stronger motivation to approach potentially pleasurable outcomes. The strength of the DA signal and level of DA availability are under polygenetic control and therefore influenced by many factors such as the dopamine transporter (DAT), the density of DA receptors, the ability of the cell to synthesize DA, and its ability to secrete DA into the synapse. Alternatively, a sluggish DA system is reflected in an anhedonic demeanor and a relative insensitivity to reward (Cohen et al, 2005; Depue and Collins, 1999; Evans et al, 2006). Consequent on individual differences in reward sensitivity, people also differ in their responses to addictive drugs, which act on the same brain pathways that subserve natural rewards like food and novelty. This variation can be attributed—at least in part—to the genetically determined function of the proteins involved in the action and availability of mesocorticolimbic DA (Lott et al, 2005; Stein et al, 2005).
DAT1 Genotypes and Behavioral Responding
The DAT is of particular genetic interest because the mechanism of action for psychomotor stimulant drugs such as cocaine, methylphenidate (MP), and amphetamine is to bind to the DAT, thereby inhibiting the reuptake of DA into the cell, and increasing its availability in the synapse. The DAT is especially highly expressed in the human striatum (an integral part of the mesolimbic reward pathways) where it is a critical regulator of synaptic DA and the duration of DA activity. The DAT1 gene that encodes the DAT protein is polymorphic, and in most human populations occurs with greatest frequency in the 9- and 10-repeat forms (Vandenbergh et al, 1992).
Although there have been some conflicting findings concerning the functional effect of the DAT1 VNTR polymorphism on the DAT, the best evidence suggests that the DAT binding site density for the 10-repeat VNTR is elevated approximately 50% over that of the 9-repeat allele (VanNess et al, 2005). In other words, the 10-repeat allele yields the greatest amount of DAT protein, with the net result of relatively less DA in the synapse because of heightened transportation back into the cell. Because of its pivotal role in the regulation of striatal DA availability—a key influence on aspects of personality and motivation—DAT1 genotypic variation has been widely investigated in the risk profile for certain psychiatric syndromes and conditions.
1. The psychotic symptoms sometimes associated with cocaine intoxication are generally attributed to an excess of synaptic DA activity (Kreek et al, 2005). Genetic variation in the DAT is therefore likely to influence risk for this condition among cocaine users (Cubells et al, 2000). Indeed, in one study cocaine-induced paranoia was significantly more prevalent in those with the 9/9 and 9/10 genotypes compared with those homozygous for the 10-repeat (Gelernter et al, 1994). Such links are explainable by the relative reduction of DAT protein density, and the consequent higher synaptic DA availability in those with a copy of the 9-repeat allele. For these individuals, it seems that cocaine increases, to a subjectively aversive level, a system that is already abundantly activated.
2. Because the reinforcing effects of stimulant drugs and palatable foods are regulated, in large part, by the same DA pathways (Corwin, 2006; Kelley et al, 2005; Wang et al, 2004), it is not surprising that the DAT1 gene has also been investigated in the context of both these behaviors. In a case–control study of Japanese women with clinically significant binge-eating behaviors, the frequency of the short alleles (7- or 9-repeat) was significantly higher in the patient group (Shinohara et al, 2004). This could imply that a strong DA signal, because of a relative reduction in the DAT protein, increased the reinforcing value of food and the tendency to binge eat. Similarly, ‘never smokers’ and ‘current nonsmokers’ had an excess prevalence of the 9-repeat allele compared with regular smokers (Timberlake et al, 2006). The authors suggest that the 9-repeat might confer a protective effect to addictive substances like nicotine because of enhanced synaptic DA availability in people who possess this allele. A study by Epstein et al (2004) produced rather different results. They found that subjects who were high on food reinforcement (as assessed by a behavioral choice questionnaire) and who had the 10/10 genotype consumed significantly more calories than subjects in the other groups. However, all the subjects were regular (>10 cigarettes a day) smokers, which limits, to some degree, the generalizability of the findings.
3. At the other end of the spectrum of DA availability, several lines of converging evidence underscore the importance of the DAT1 gene to risk for attention-deficit hyperactivity disorder (ADHD). In numerous studies, the 10-repeat allele has been associated with the clinical ADHD phenotype (see Bellgrove et al, 2005 for a review). Although the most common treatment for ADHD is MP, recent studies have also reported a variable treatment response to this drug, which is linked to patient differences in the DAT1 genotype (eg Bellgrove et al, 2005; Stein et al, 2005). Those who were homozygous for the 9-repeat showed the poorest treatment response, whereas those who were homozygous for the 10-repeat showed the best. It was concluded that MP may be most effective in the 10-repeat group because it ameliorates a hypodopaminergic state mediated by the DAT1. Brain imaging research has also confirmed these findings by showing that ADHD adults with low DAT levels (analogous to the 9-repeat allele) were nonresponders to MP compared with those with elevated DAT availability (Krause et al, 2005).
In a related study, Lott et al (2005) also found that participants who were homozygous for the 9-repeat reported a diminished subjective response to amphetamine, especially on measures related to feeling euphoric and generally affected by the drug. Like the previous ADHD studies, these results may be attributed to the relative diminution of available synaptic DA in the 10/10 group, and therefore a more pronounced subjective response to the drug.
A summary of the proposed inter-relationships among DAT1 genotype, DA signal strength, and psychobehavioral responding is presented in Table 1.
The Present Study
The present study is a continuation of our previous research investigating the influence of DA-based reward sensitivity on overeating behaviors. Its purpose was to use a case–control design to examine the role of DAT1 genotypes in appetite response to a palatable food cue in adults with binge eating disorder (BED). Evidence suggests that women who have high sensitivity to reward report stronger food cravings (Franken and Muris, 2005) and are more likely to overeat (Davis et al, 2004, 2007) and binge eat (Davis and Woodside, 2002; Davis et al, 2005) compared with their less hedonic counterparts. Amplification of the DA signal in human participants via a small dose of oral MP has also been shown to increase desire to eat in response to a palatable food cue (Volkow et al, 2002). However, because DA activation level and subjective response are likely to have an inverted-U relationship (Volkow et al, 1999), it is probable that very high stimulation of DA pathways will curb appetite, as is typically seen in the case of chronic drug abuse (Cochrane et al, 1998). In other words, an increase of the DA signal within the moderate/normal range is likely to foster appetitive motivation, whereas augmentation to very high levels is likely to do the opposite—in the case of eating—to cause a suppression effect. Some of the apparent contradictions in the literature concerning the relationship between DA activation and food intake may be better understood by consideration of such a nonlinear relationship.
We used a MP drug challenge to investigate whether appetite for a palatable food stimulus would be differentially affected by DAT1 genotype. Although Lott et al (2005) found a stronger feeling of euphoria in those with the 10/10 genotype, it is unknown whether the effect on appetite will parallel these findings. We also set out to test the hypothesis that adults with BED—a group defined by chronic and nonhomeostatic, overeating—would have a greater prevalence of the 9-repeat allele than an age-matched, normal weight, healthy comparison group. Our reasoning for this prediction was that a relatively robust DA signal (promoted by a less expressed DAT) would promote a relatively strong appetitive response to natural rewards like food.
MATERIALS AND METHODS
Subjects
Adults between the ages of 25 and 45 years who met criteria for BED (n=32), and an age-matched sample of healthy adult men and women (n=46), were recruited from posters placed at universities, local hospitals, and other public institutions. (Five additional subjects took part in the study, three BED and two controls, but were not included in any of the analyses because each had one rare allele.) Advertisements were also placed in local newspapers. Control participants were first screened during a structured telephone interview and excluded if they had any serious medical condition, were taking any prescription medication except oral contraceptives, were pregnant or had recently given birth, or were currently being treated for any Axis I psychiatric disorder including an eating or substance-dependent disorder (American Psychiatric Association, 1994, DSM IV). They were also required to be fluent in English.
BED participants were required to meet an operational definition of the disorder using ratings on the Eating Disorder Examination (Fairburn and Cooper, 1993), a research assessment interview. This definition was based on that provided in the main body of the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (American Psychiatric Association, 1994, p 550) where BED is defined as follows: ‘recurrent episodes of binge eating in the absence of the regular use of inappropriate compensatory behaviors characteristic of bulimia nervosa’. This definition was operationalized in the following way. Participants had to report at least weekly objective binge episodes over the previous 3 months, but over this period they must not have vomited, fasted, or taken laxatives or diuretics as a means of controlling their shape or weight. Nor must they have met DSM IV diagnostic criteria for bulimia nervosa or anorexia nervosa. BED diagnosis was established during a telephone interview carried out by trained personnel. The same exclusion criteria were applied to BED adults as to the control subjects, except that we included BED subjects who were being treated for unipolar depression without psychotic symptoms (confirmed by a clinical interview before the beginning of the study) because of the high comorbidity between BED and depression. However, subjects taking antidepressant medication contraindicated for MP (such as Wellbutrin) were excluded. All subjects obtained an electrocardiogram before the drug challenge.
Design
This study employed a three-session, double-blind, crossover design, during which each subject received a dose of oral MP equivalent to 0.5 mg per kg of body weight (up to a dose of 50 mg), or an identical placebo capsule, in an order randomized by the dispensing pharmacy. Subjects were monitored for 2 h after administration of the capsule. Genotyping was performed blind to any of the clinical or behavioral data reported in this study.
Procedure
The procedures employed in this study were approved by the three Research Ethics Boards relevant to the institutional affiliations of the authors, and were carried out in accordance with the Declaration of Helsinki.
On the first day of testing, informed consent was obtained, and all the demographic information was obtained in a face-to-face interview. Height and weight were measured and blood pressure was taken. For BED subjects, the structured clinical interview was carried out, and for control subjects a briefer nonpatient psychiatric screening took place, which included questions about substance use and disordered eating. At this session, the electrocardiogram was obtained as well as the blood sample for genotyping and to confirm the absence of pregnancy in female subjects. In preparation for the food challenge, subjects were asked to indicate their ‘favorite snack food’ with the constraint that it did not need to be cooked (like french fries) or kept frozen (like ice cream). If the subject first indicated a ‘healthy’ option like an apple, the interviewer probed further until the subject selected a conventional sweet or salty snack. The most common choices were chocolate bars, potato chips, and cookies. At this session, subjects also completed certain computerized neuropsychological tests and were given a questionnaire package comprising personality and eating behavior inventories. Details of these measures will be reported elsewhere.
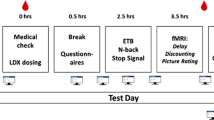
For each subject, the two drug-challenge testing sessions were scheduled at the same time of day, and the same day of the week, separated by 1 week. Subjects were instructed to eat a normal meal 2 h before their appointment, and to abstain from drinking a caffeine beverage or smoking a cigarette on the testing day. Upon arriving at the laboratory, blood pressure was taken and a baseline mood rating inventory completed before the capsule was ingested. As the peak uptake of MP is approximately 1 h, subjects were seated comfortably for 75 min in a quiet room after ingesting the capsule, and provided with light reading materials. Every 15 min, the mood rating checklist was completed to monitor any adverse reactions. Seventy-five minutes after administration of the capsule, the snack was presented to the subject.
Dependent Measure
Subjects were given their ‘favorite snack’ by the experimenter and asked to respond verbally to the following questions using a scale from 1–10 (1=‘not at all’ and 10=‘a great deal’). They were also encouraged to try and answer each question without concern for calories or whether they would normally eat such snacks at that time of day.
-
1
How hungry does it make you feel to see your favorite snack?
-
2
How much would you like to eat some of this snack—even just a small portion? (at this point the participant was asked to eat a piece of the snack).
-
3
Now that you’ve had a taste of your favorite snack, how strong is your desire to have some more?
The ratings for the three appetite questions were summed for the placebo day and the drug day, and a difference score was calculated by subtracting the placebo score from the drug score. Therefore, negative scores reflect appetite suppression, whereas positive scores reflect appetite enhancement on the drug day.
Genotyping
A venous blood sample (20–30 ml) was collected from each subject. Genomic DNA was extracted by the high-salt method. Amplification of a 40 bp repetitive element (plus 80 bp of flanking sequence) in the 3′ untranslated region (UTR) of the dopamine transporter gene (DAT1) was performed according to conditions previously described by Vandenbergh et al (1992). DNA bands were separated on 3.5% agarose gel (Bioshop Canada, Burlington, ON, Canada) and sized by comparing them with a standard 100 bp ladder (MBI Fermentas, Burlington, ON, Canada). The allele names indicate the number of 40 bp repeats present in the amplified fragment.
Data Analysis
Subjects were genotyped at the 3′-UTR VNTR polymorphism of the DAT1 and classified as 9/9, 9/10, and 10/10. In the first analysis, a 2 Group (BED vs Control) × 3 Genotype (9/9, 9/10, 10/10) ANCOVA was carried out, with the snack-rating difference score as the dependent measure, and BMI, gender, and education level as covariates. Education level was treated as a binary variable as seen in Table 3. Those with an undergraduate degree or higher were in one category and the remaining subjects in another. The dependent variable was roughly normally distributed with low values for skewness (−0.88) and kurtosis (1.03). Owing to the low occurrence of the rare 9/9 genotype, the 9/9 and 9/10 groups were combined and a subsequent 2 × 2 ANCOVA was conducted with the same dependent variable. All post hoc analyses were carried out with independent samples t-tests (SPSS 14.0, Chicago, IL, USA).
RESULTS
Subject Characteristics
Allele and genotype frequencies for the 9-repeat and 10-repeat alleles are shown in Table 2, and match closely with values found in other studies with equivalent samples (eg Lott et al, 2005; Timberlake et al, 2006). There were no differences between BED and control subjects in terms of age, ethnicity, or current use of alcohol and nicotine. However, there were more female subjects in the control group, a greater percentage of them had an undergraduate degree or higher, and they had a lower BMI than the BED subjects (Table 3).
Genotype Differences in Appetite-Suppression Effects to MP
We first examined whether there were baseline differences on appetite ratings by conducting a 2 (Group) × 3 (Genotype) ANCOVA with the total appetite rating score in the placebo condition as the dependent variable. Results indicated no significant main effects, nor a significant interaction. In the following ANCOVA analyses, we used the drug–placebo difference score as the dependent variable.
Summary statistics for the 2 × 3 ANCOVA are presented in Table 4. Both main effects were statistically significant and there was a significant Group × Genotype interaction. Simple post hoc t-tests indicated that BED subjects with the 9/10 genotype showed a greater degree of appetite suppression (t=2.0, p=0.05) than those from the control group, which did not differ from either of the 10/10 genotype groups. Data for the 9/9 Group difference were not analyzable because there was only a single subject with this genotype in the BED subjects. Figure 1 displays the results graphically.

Snack-rating difference scores as a function of diagnostic group (BED vs Control) and three DAT1 genotype groups.
Owing to the rare occurrence of the 9-repeat homozygote, many studies have combined individuals with at least one copy of the 9-repeat (ie 9/9 and 9/10) and compared them with the frequently occurring 10/10 group (eg Bellgrove et al, 2005; Kirley et al, 2003). Following this approach, we reanalyzed the data using a 2 (Group) × 2 (Genotype) ANCOVA with the snack-rating difference score as the dependent variable. Again the results indicated a significant Group × Genotype interaction (Table 5), and post hoc t-tests showed a greater appetite suppression effect in the BED subjects with 9-repeat than in the 9-repeat control subjects (t=2.19, p=0.039), who also did not differ from the 10/10 BED and control subjects. These results are displayed graphically in Figure 2.

Snack-rating difference scores as a function of diagnostic group (BED vs Control) and two DAT1 genotype groups.
DISCUSSION
DA is one of the most salient neurotransmitters in the reinforcement value of food and the regulation of its intake (Epstein et al, 2002). Although drugs that substantially increase brain DA tend to induce anorexia in animals (eg Bina and Cincotta, 2000; Kuo, 2002), there is considerable variation in response magnitude across human subjects. In a recent study with a small group of obese adults, Leddy et al (2004) found that approximately equal numbers showed either a large decrease, a small/moderate decrease, and even an increase in calorie intake from baseline following a large dose of MP (1 mg/kg of body weight). And, these effects did not correlate with initial body weight.
Individual differences in appetite response to MP are most likely regulated by polygenetic factors that influence brain DA availability. To our knowledge, the present study is the first to have examined the suppression of appetite ratings to MP in relationship to DAT1 genotype variation. As a first-step investigation, this was an appropriate candidate gene to select, as MP's mechanism of action is to bind to the DAT. Adults with BED were also an interesting group to examine, as they represent a phenotype with excessive overeating and difficulty in suppressing appetite. It is noteworthy that the Food and Drug Administration in the US currently endorses certain weight-loss medications, most of which stimulate norepinephrine and DA release in a manner similar to MP (Moyers, 2005).
At baseline (the placebo condition), we found no difference between diagnostic groups or among genotypes in appetite ratings to a palatable food cue. This null finding may have occurred because there was no significant group difference in DAT1 genotype frequencies. It may also reflect a ceiling effect, as the ratings were relatively high in both groups in the placebo condition. Recall that the food cue was each individual's personally selected ‘favorite snack’, and participants were approximately 3 h food deprived at the time of presentation. However, when we examined drug vs placebo appetite difference scores, there was a significant interaction of the two main effects. In both analyses, BED subjects with at least one copy of the 9-repeat allele showed a significant decrease in appetite ratings in the drug condition compared with controls with the 9-repeat, or to BED and controls with the 10/10 genotype—all three of whom showed negligible rating differences between drug and placebo conditions.
These findings are a challenge to explain, as there are two possible, but competing, theoretical hypotheses for the MP appetite responses and DAT1. On the one hand, as Leddy et al (2004) have suggested, the 10/10 genotype (those believed to have enhanced DAT) might have a stronger response to MP because this drug would have more influence on reducing DA reuptake, would maintain brain DA activation for longer, and could, therefore, induce an anorexic response. To the contrary, however, our findings indicated virtually no effect on appetite ratings for subjects with the 10/10 genotype, irrespective of diagnostic group. On the other hand, it could be argued that those with the 9-repeat (because of the diminished expression of DAT) have a high tonic level of DA activation, and so the administration of MP could overstimulate the brain reward pathways that regulate food intake, and thereby suppress appetite. Our results support this latter possibility, but only in those with BED.
The most probable explanation for the BED/9-repeat effect assumes the presence of some (currently unknown) genetic variant, which is overrepresented in this clinical group, and which interacts with the 9-repeat allele to suppress appetite. There is good evidence from the field of addiction research that small and single gene effects can greatly exceed their additive influence when they occur in combination (eg Lerman and Berrettini, 2003). Unfortunately, genetic studies of BED are still in their infancy so it is difficult to speculate on what additional genetic effects might have influenced our results. Individual differences in DA receptor availability, or the absorption and metabolism of MP, are reasonable candidates for future investigation. The BED subjects were also, on average, obese compared with the control subjects who were of normal weight—a factor that may in some way contribute to differences in DA signalling.
One of the implications of our study is that MP may be a useful treatment for certain individuals with BED. This is a particularly interesting consideration in light of recent evidence linking AD(H)D to overeating/binge eating and obesity (see Davis et al, 2006 for a review). Our findings demonstrated that BED individuals with the 10/10 genotype showed no appetite suppression to MP, whereas other research has found that in patients with AD(H)D, this genotype showed the best treatment response to MP (Bellgrove et al, 2005; Stein et al, 2005). Future studies will do well to examine the AD(H)D status of patients with BED, and whether comorbidity is related to genotype, and treatment response to MP.
Contrary to prediction, we also did not find a significant difference in DAT1 genotype frequencies between BED subjects and the healthy control group. It is worth noting, however, that the results were in the expected direction, 50% of BED subjects compared with 39% of controls carried at least one copy of the 9-repeat allele. From a statistical perspective, it is possible that our results reflect a Type II error and that a sample with greater power would find support for our hypothesis. To the best of our knowledge, this is the first study to report DAT1 data for adults with BED, and therefore provides a promising direction for future and more comprehensive studies with larger samples.
It is important to emphasize that our data can only be viewed as preliminary and suggestive, as the sample size precluded an adequate investigation of the 9/9 genotype—a group who appears from previous studies to have a different (or more pronounced) stimulant drug response than the other DAT1 genotypes (eg Lott et al, 2005; Stein et al, 2005). Owing to the rarity of the 9/9 genotype, however, relatively large samples will be necessary to find adequate representation of this group. A limitation of the study is also the fact that we only assessed subjective sensations of hunger and desire to eat, rather than objective food intake. Although some research reports a weak or absent relationship between these two variables, other studies have reported relatively strong correlations (see Parker et al, 2004a, 2004b for reviews). However, to the best of our knowledge, no research has assessed this association in BED—a factor of considerable importance given the clinical evidence that binge eating in BED is typically not triggered by hunger. In other words, the correlation between food intake and appetite ratings may be very different in this group than among the general non-eating disordered population. For these reasons, future research in this area should monitor actual consumption as well as appetite ratings following the food-cue presentation. Nevertheless, our findings provide interesting preliminary evidence that the DAT might be implicated in appetite suppression to stimulant medication, and as such have relevance for therapeutic pharmacologic agents currently in use (or being developed) to assist in weight loss. It will also behoove future researchers in this area to consider gene–gene effects and how these interact with relevant symptoms of disordered eating such a binge eating and strong food cravings.
References
American Psychiatric Association (1994). Diagnostic and Statistical Manual—Version IV. American Psychiatric Association Press: Washington.
Bellgrove MA, Hawi Z, Kirley A, Fitzgerald M, Gill M, Robertson IH (2005). Association between dopamine transporter (DAT1) genotype, left-sided inattention, and an enhanced response to methylphenidate in attention-deficit hyperactivity disorder. Neuropsychopharmacology 30: 2290–2297.
Berridge KC (2003). Pleasures of the brain. Brain Cogn 52: 106–128.
Bina KG, Cincotta AH (2000). Dopaminergic agonists normalize elevated hypothalamic neuropeptide Y and corticotropin-releasing hormone, body weight gain, and hyperglycemia in ob/ob mice. Neuroendocrinology 71: 68–78.
Cochrane C, Malcolm R, Brewerton T (1998). The role of weight control as a motivator for cocaine abuse. Addict Behav 23: 201–207.
Cohen MX, Young J, Baek J-M, Kessler C, Ranganath C (2005). Individual differences in extraversion and dopamine genetics predict neural reward responses. Cogn Brain Res 25: 851–861.
Corwin RL (2006). Bingeing rats: a model of intermittent excessive behavior? Appetite 46: 11–15.
Cubells JF, Kranzler HR, McCance-Katz E, Anderson GM, Malison RT, Price LH et al (2000). A haplotype at the DBH locus, associated with low plasma dopamine β-hydroxylase activity, also associates with cocaine-induced paranoia. Mol Psychiatry 5: 56–63.
Davis C, Levitan RS, Smith M, Tweed S, Curtis C (2006). Associations among overeating, overweight, and attention deficit/hyperactivity disorder: a structural equation modelling approach. Eating Behav 7: 266–274.
Davis C, Patte K, Levitan RS, Reid C, Tweed S, Curtis C (2007) From motivation to behavior: a model of reward sensitivity, overeating, and food preferences in the risk profile for obesity. Appetite 48: 12–19.
Davis C, Strachan S, Berkson M (2004). Sensitivity to reward: Implications for overeating and overweight. Appetite 42: 131–138.
Davis C, Tweed S, Curtis C (2005). Decision-making deficits and personality risk factors: an addiction model of binge eating. Presentation at the Annual Meeting of the Eating Disorder Research Society, Toronto, September.
Davis C, Woodside DB (2002). Sensitivity to rewarding effects of food and exercise in the eating disorders. Compr Psychiatry 43: 189–194.
Depue RA, Collins PF (1999). Neurobiology of the structure of personality: dopamine, facilitation of incentive motivation, and extraversion. Behav Brain Sci 22: 491–517 (Discussion 518–569).
Epstein LH, Jaroni JL, Paluch RA, Leddy JJ, Vahue HE, Hawk L et al (2002). Dopamine transporter genotype as a risk factor for obesity in African-American smokers. Obes Res 10: 1232–1240.
Epstein LH, Wright SM, Paluch RA, Leddy JJ, Hawk Jr LW, Jaroni JL et al (2004). Relation between food reinforcement and dopamine genotypes and its effect on food intake in smokers. Am J Clin Nutr 80: 82–88.
Evans AH, Lawrence AD, Potts J, MacGregor L, Katzenschlager R, Shaw K et al (2006). Relationship between impulsive sensation seeking traits, smoking, alcohol and caffeine intake, and Parkinson's disease. J Neurol Neurosurg Psychiatry 77: 317–321.
Fairburn CG, Cooper Z (1993). The eating disorder examination. In: Fairburn CG, Wilson GT (eds). Binge Eating: Nature, Assessment, and Treatment. Guilford Press: New York. pp 317–360.
Franken IHA, Muris P (2005). Individual differences in reward sensitivity are related to food craving and relative body weight in healthy women. Appetite 45: 198–201.
Gelernter J, Kranzler HR, Satel SL, Rao PA (1994). Genetic association between dopamine transporter protein alleles and cocaine-induced paranoia. Neuropsychopharmacology 11: 195–200.
Kelley AE, Schiltz CA, Landry CF (2005). Neural systems recruited by drug- and food-related cues: studies of gene activation in corticolimbic regions. Physiol Behav 86: 11–14.
Kirley A, Lowe N, Hawi Z, Mullins C, Daly G, Waldman I et al (2003). Association of the 489 bp DAT1 allele with methylphenidate response in a sample of Irish children with ADHD. Am J Med Genet Part B 121B: 50–54.
Krause J, la Fougere C, Krause K-H, Ackenheil M, Dresel SH (2005). Influence of striatal dopamine transporter availability on the response to methylphenidate in adult patients with ADHD. Eur Arch Psychiatry Clin Neurosci 255: 428–431.
Kreek MJ, Bart G, Lilly C, LaForge KS, Nielson DA (2005). Pharmacogenetics and human molecular genetics of opiate and cocaine addictions and their treatments. Pharmacol Rev 57: 1–26.
Kuo DY (2002). Co-administration of dopamine D-1 and D-2 agonists additively decreases daily food intake, body weight and hypothalamic neuropeptide y level in rats. J Biomed Sci 9: 126–132.
Leddy JJ, Epstein LH, Jaroni JL, Roemmich JN, Paluch RA, Goldfield GS et al (2004). Influence of methylphenidate on eating in obese men. Obes Res 12: 224–232.
Lerman C, Berrettini W (2003). Elucidating the role of genetic factors in smoking behavior and nicotine dependence. Am J Med Genet 118B: 48–54.
Lott DC, Kim S-J, Cook Jr EH, de Wit H (2005). Dopamine transporter gene associated with diminished subjective response to amphetamine. Neuropsychopharmacology 30: 602–609.
Moyers SB (2005). Medications as adjunct therapy for weight loss: approved and off-label agents in use. J Amer Diet Assoc 105: 948–959.
Nicola SM, Taha SA, Kim SW, Fields HL (2005). Nucleus accumbens dopamine release is necessary and sufficient to promote the behavioral response to reward-predictive cues. Neurosci 135: 1025–1033.
Parker BA, Ludher AK, Loon TK, Horowitz M, Chapman IM (2004a). Relationships of rating of appetite to food intake in healthy older men and women. Appetite 43: 227–233.
Parker BA, Sturm K, MacIntosh CG, Feinle C, Horowitz M, Chapman IM (2004b). Relation between food intake and visual analogue scale ratings of appetite and other sensations in healthy older and younger subjects. Eur J Clin Nutr 58: 212–218.
Shinohara M, Mizushima H, Hirano M, Shioe K, Nakazawa M, Hiejima Y et al (2004). Eating disorders with binge-eating behaviour are associated with the s allele of the 3′-UTR VNTR polymorphism of the dopamine transporter gene. J Psychiatry Neurosci 29: 134–137.
Stein MA, Waldman ID, Sarampote CS, Seymour KE, Robb AS, Conlon C et al (2005). Dopamine transporter genotype and methylphenidate dose response in children with ADHD. Neuropsychopharmacology 30: 1374–1382.
Timberlake DS, Haberstick BC, Hopfer C, Lessem JM, Smolen A, Ehringer M et al (2006). An association between the DAT1 polymorphism and smoking behavior in young adults from the National Longitudinal Study of Adolescent Health. Health Psychol 25: 190–197.
Vandenbergh DJ, Persico AM, Hawkins AL, Griffin CA, Li X, Jans EW et al (1992). Human dopamine transporter gene (DAT1) maps to chromosome 5p15.3 and displays a VNTR. Genomics 14: 1104–1106.
VanNess SH, Owens MJ, Kilts CD (2005). The variable number of tandem repeats element in DAT1 regulates in vitro dopamine transporter density. BMC Genetics 5: 55 doi:10.1186/1471-2156-6-55.
Volkow ND, Wang G-J, Fowler JS, Logan J, Gatley SJ, Gifford A et al (1999). Prediction of reinforcing responses to psychostimulants in humans by brain dopamine D2 receptor levels. Am J Psychiatry 156: 1440–1443.
Volkow ND, Wang G-J, Fowler JS, Logan J, Jayne M, Francesschi D et al (2002). ‘Nonhedonic’ food motivation in humans involves dopamine in the dorsal striatum and methylphenidate amplifies this effect. Synapse 44: 175–180.
Wang GJ, Volkow ND, Thanos PK, Fowler JS (2004). Similarity between obesity and drug addiction as assessed by neurofunctional imaging: a concept review. J Affect Disord 23: 39–53.
Yun IA, Wakabayashi KT, Fields HL, Nicola SM (2004). The ventral tegmental area is required for the behavioral and nucleus accumbens neuronal firing responses to incentive cues. J Neurosci 24: 2923–2933.
Zangen A, Solinas M, Ikemoto S, Goldberg SR, Wise RA (2006). Two brain areas for cannabinoid reward. J Neurosci 26: 4901–4907.
Acknowledgements
Project funding was provided by the Canadian Institute of Health Research.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Davis, C., Levitan, R., Kaplan, A. et al. Dopamine Transporter Gene (DAT1) Associated with Appetite Suppression to Methylphenidate in a Case–Control Study of Binge Eating Disorder. Neuropsychopharmacol 32, 2199–2206 (2007). https://doi.org/10.1038/sj.npp.1301348
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.npp.1301348
Keywords
This article is cited by
-
Neural circuit control of innate behaviors
Science China Life Sciences (2022)
-
The association of insertions/deletions (INDELs) and variable number tandem repeats (VNTRs) with obesity and its related traits and complications
Journal of Physiological Anthropology (2017)
-
Genetic Similarities between Compulsive Overeating and Addiction Phenotypes: A Case for “Food Addiction”?
Current Psychiatry Reports (2015)
-
Association of a carboxylesterase 1 polymorphism with appetite reduction in children and adolescents with attention-deficit/hyperactivity disorder treated with methylphenidate
The Pharmacogenomics Journal (2013)
-
Reward circuitry dysfunction in psychiatric and neurodevelopmental disorders and genetic syndromes: animal models and clinical findings
Journal of Neurodevelopmental Disorders (2012)
