
Abstract
Evidence suggests that manipulating spatial information within working memory depends upon a circuitry organized around the prefrontal cortex (PFC) and the activity of the catecholamine systems. Other evidence attests to the effects of Δ-9 tetrahydrocannabinol (THC) on short-term spatial memory function, most probably involving CB1 receptor activity within hippocampal circuitries. At the current time, there have been no systematic studies of the effects of THC on spatial working memory in human subjects using tasks known to depend upon frontotemporal neural circuitries. We examined the effects of a single sublingual 5 mg dose of THC on a test of spatial working memory (requiring active manipulation of remembered spatial information for the management of future behavior) and a test of spatial span (requiring only the reproduction of sequences of previously presented spatial cues). In all, 19 healthy adults were administered 5 mg THC and placebo in a double-blind, placebo-controlled, within-subject, crossover design. Male participants performed more accurately than female participants. THC significantly enhanced spatial working memory performance of female participants. By contrast, male and female participants produced more intrusion errors during performance of the Spatial Span task. These results suggest that THC has relatively complex effects on spatial memory in human subjects, perhaps reflecting altered CB1 receptor activity within frontotemporal circuits or altered activity of mesocortical dopaminergic pathways in PFC areas associated with spatial memory.
Similar content being viewed by others

INTRODUCTION
The ability to represent and manipulate information within short-term memory is a critical mechanism underpinning the flexible control of behavior and the successful attainment of (changing) behavioral goals (Fuster, 1989). Converging evidence, garnered from experimental work in both animal and human subjects, has convincingly demonstrated that this ‘working memory’ function depends both upon a neural circuitry organized round the lateral areas of the prefrontal cortex (PFC) and its neuromodulation by the catecholamines, dopamine (DA) and noradrenaline (NA). Focal lesions of the PFC in monkeys and in human neurological patients impair the capacity to retain spatial information over short intervals and use it to guide subsequent behavior (eg Petrides and Milner, 1982), while comparable deficits have been repeatedly demonstrated following depletion of DA within this cortical area in primate models (Brozoski et al, 1979; Roberts et al, 1994).
Follow-up work indicates that the contribution of DA to spatial working memory is mediated by the D1 (Arnsten et al, 1994; Sawaguchi and Goldman-Rakic, 1991) and D2 families of receptors (Arnsten et al, 1995; Zhang et al, 2004) that may influence mnemonic and response aspects of information processing within primate PFC (Wang et al, 2004; Williams and Goldman-Rakic et al, 1995). Other research attests to the importance of NA transmission, and the balanced activity of α1- and α2-adrenoceptors, in protecting the cognitive functions of the lateral PFC from the deleterious effects of stress (Arnsten, 2000; Arnsten and Contant, 1992; Arnsten and Jentsch, 1997; Birnbaum et al, 2000). Therefore, despite occasional failures to find catecholamine influences in some working memory models (Collins et al, 1998) and continuing uncertainty about the relative importance of the D2 family of receptors (Barch, 2004; Müller et al, 1998), the weight of the available evidence suggests that DA and NA have complementary roles in modulating the prefrontal substrates of spatial working memory.
Studies in humans largely confirm the influence of catecholamines on spatial memory. Withdrawal of L-DOPA medication from patients with Parkinson's disease has been found to impair performance of cognitive tasks dependent on lateral sectors of the PFC, including one test of spatial working memory known to be highly sensitive to focal lesions of the frontal lobes (Lange et al, 1992; Owen et al, 1990; see below). By contrast, administration of the mixed DA and NA agonist, methylphenidate, to healthy participants facilitated performance of the same task (Elliott et al, 1997), probably by modulating neuronal activity within a distributed circuitry encompassing lateral PFC and inferior parietal cortex (Mehta et al, 2000). Agents that act (with varying selectivity) on D2 receptors (including bromocriptine, sulpiride, and pergolide) have produced less consistent effects (Kimberg et al, 1997; Kimberg and D'Esposito, 2003; Luciana et al, 1992; Mehta et al, 2001, 2004). Finally, treatment with the mixed α1/α2-adrenoceptor agonists, clonidine, and the more selective α2-adrenoceptor agonist, guanfacine, have also shown complimentary impairments and improvements in spatial working memory (Coull et al, 1995; Jakala et al, 1999).
Δ-9-tetrahydrocannibinol (THC) has consistently been found to affect verbal learning and memory (see, Hollister, 1986; Miller and Branconnier, 1983; Ameri, 1999, for a review), and such impairments are likely to underpin difficulties with more complex mental activities such as arithmetic and planning (Casswell and Marks, 1973; Chait and Perry, 1994). However, the evidence that THC particularly impairs working memory in human subjects is slightly more equivocal, with positive (Heishman et al, 1997; D'Souza et al, 2004) but also recent negative findings (Curran et al, 2002). Recent animal research has utilized spatial radial arm maze tests, the Morris water maze task, and delayed-to-matching (and nonmatching) tasks to examine the role of the hippocampus in short-term spatial memory (Lichtman and Martin, 1996; Hampson and Deadwyler, 1999, 2000; Varvel and Lichtman, 2002). These studies have demonstrated that administration of CB1 receptor agonists, such as WIN 55,212-2, produce delay-dependent (and, therefore, properly mnemonic) deficits that can be reversed with the antagonist, SR141716A (Mallet and Beninger, 1998). Other evidence suggests that these deficits are mediated by CB1 receptors on hippocampal neurones or, perhaps, GABAergic interneurones (Heyser et al, 1993; Hampson and Deadwyler, 1999).
Studies of THC–PFC interactions in working memory have been more limited despite the presence of significant numbers of CB1 receptors within anterior cortical areas (Herkenham et al, 1990) and the finding that THC administration increases DA and acetycholine activity, within the PFC (Diana et al, 1998; Verrico et al, 2003). Jentsch et al (1997) have also reported that THC dose dependently activated DA and NA but not 5-HT, within rat PFC with an associated impairment in spatial working memory, perhaps mediated by hyperdopaminergic activity within frontostriatal circuitry (Robbins, 1996).
In this study, we investigated the effects of a relatively low dose of THC plant extract (5 mg delivered sublingually) on two measures of spatial memory in healthy human subjects. One task—Spatial Working Memory—is derived from the self-ordered pointing task originally designed for assessing working memory deficits in human neurological patients (Petrides and Milner, 1982). Performance of this task has been shown to be sensitive to focal lesions of the frontal and, to a lesser extent, temporal lobes (Owen et al, 1990, 1996b), to be associated with increased neural activity within dorsolateral PFC (Owen et al, 1996a, 1996b) and to be influenced by catecholamine activity in healthy volunteers (Coull et al, 1995; Elliott et al, 1997). This task explicitly requires subjects to use stored spatial information in order to guide future responding, and comes with a reliable measure of strategy.
The second task—Spatial Span—is based on the Corsi block-tapping test (Milner, 1971), and requires subjects to simply reproduce sequences of presented spatial cues; no manipulation or strategy is required to ensure good performance. Performance of this task has also been found to be sensitive to damage within frontotemporal circuitry (see, Lezak, 1995, for a review) and to be associated with increased neural activity within ventrolateral rather than dorsolateral PFC (Owen et al, 1996a). We sought to test the hypothesis that acute administration of 5 mg THC to a sample of young, healthy adults would alter performance of a Spatial Working Memory task, requiring the manipulation of information for the guidance of future behavior, with lesser changes evident on the performance of a Spatial Span task requiring only the accurate reproduction of previously presented spatial information.
MATERIALS AND METHODS
Subjects
In all, 12 healthy males and seven healthy females participated. General practitioner approval was obtained, and a full medical history and examination taken. Participants were carefully screened for any clinically significant psychiatric or physical illness. One male and five female participants reported less than 10 lifetime uses of cannabis; eight males and two females reported between 10 and 100; and three males reported more than 100. The study was approved by the Oxford Psychiatric Research Ethics Committee and all participants gave written informed consent. Their mean age was 21.8±0.93 years (SE) and mean verbal IQ as estimated by the National Adult Reading Test (NART; Nelson, 1982) was 113.4±1.10 (NART scores for two participants were unavailable).
Design
This study consisted of a double-blind, placebo-controlled, within-subject, crossover design. In all, 10 participants received placebo on the first study day and THC on the second study day; nine received THC on the first study day and placebo on the second study day. The two study days were separated by at least 1 week. Participants were asked to abstain from recreational drugs for the duration of the study, and from alcohol intake for 24 h and caffeine for 12 h before each study day. On attendance at the start of each study day, urine was screened for amphetamines, benzodiazepines, cocaine, methamphetamine, opiates and THC using immunometric assay kits. A pregnancy test was also performed for female participants.
Materials
THC extracted from standardized plants was administered in an ethanol and propylene glycol solution at 8.5 mg/ml concentration, using a pump-action sublingual spray. The pharmacokinetics of this method of THC administration indicates relatively wide intersubject variability in terms of AUC values; however, a Phase I trial with healthy adults suggested that mean plasma concentration values for THC tends to peak between 2 and 3 h postdosing (Guy and Robson, 2003). The total dose delivered was 5 mg THC in six actuations at 6-min intervals, with blood pressure and heart rate monitoring 5 min after each actuation. Dosing was incremental to allow termination in the event of significant adverse events. The matching placebo employed a peppermint flavoring to aid blinding.
Addiction Research Center Inventory (ARCI; Haertzen and Hickey, 1987)
The ARCI is a 53-item instrument consisting of six empirically derived subscales that are sensitive to various classes of drug effects: the Morphine–Benzedrine scale (MBG) is a measure of euphoria; the Pentobarbital–Chlorpromazine–Alcohol (PCAG) is a measure of sedation; the Amphetamine (A) and Benzedrine Group (BG) are measures of stimulant-like effects; the Lysergic acid (LSD) is a measure of dysphoric and somatic effects; and the Marijuana (M) scale is sensitive to marijuana effects.
Visual Analog Scales (VAS; Bond and Lader, 1974)
Subjective state was assessed using 16 VAS that combine to measure mental sedation (M), physical sedation (P), feelings of tranquility (T), and other sociability feelings (S).
The two spatial memory tests were taken from CANTAB (Cambridge Cognition, 1999).
Spatial Working Memory Task
On each trial, an array or ‘set’ of boxes was presented on a computer screen, which participants were required to ‘search through’ by touching each one. This resulted in the box ‘opening up’ to reveal whether a blue square or ‘token’ was hidden inside. Participants were asked to find the blue tokens and use them to fill an empty column located towards one the side of the screen. On any one search, only a single box within the displayed set contained a token. Participants searched the boxes until they found it; then, a new search for the next token would begin. The key instruction was that once a blue token had been found within a particular box, that box would not be used again to hide a token. Two types of search error were possible. First, participants may return to open a box in which a blue token had already been found during the same trial (‘between-search’ error). Second, participants may return to a box already opened and shown to be empty earlier in the same search (‘within-search’ error).
The task commenced with two practice trials with four boxes each, followed by four trials with four, six, and then eight boxes. The task was scored according to the number of between- and within-search errors at each level of difficulty. Previous research has shown that an efficient search strategy for completing this task is to follow a predetermined search sequence, beginning with a particular box and then returning to start each new search with that same box as soon as a token had been found (Owen et al, 1990). The extent to which this repetitive searching pattern was used as a strategy for approaching the task was estimated from the total number of sequences started with the same box, within each of the more difficult levels of six and eight boxes. The total of these scores provided a single measure of strategy for each participant, with a high score (ie many searches beginning with a different box) representing relatively poor strategy and a low score (ie many sequences starting with the same box) representing good strategy.
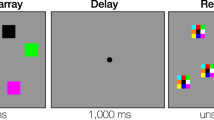
Spatial Span
On each trial, participants were shown an array of nine white boxes presented on a computer screen. Some of these boxes changed color (to green for 1 s) in a sequence; participants were then required to reproduce this sequence by touching each box in the same sequence. Two practice trials of two boxes were followed by one trial at each of three, four, five, and six boxes. If an error was made, then two more attempts were permitted with the same number of boxes. The length of the sequences presented increased up to a maximum sequence of nine items. The dependent measure for this task were (i) the spatial span, that is, the maximum length of sequence successfully reproduced, (ii) the total number of errors committed during performance of the whole task; and (iii) total usage errors (defined as the number of times the participants touched a box not in the original sequence to be reproduced).
Procedure
Participants attended the laboratory at 0830 hours in the morning. They completed the VAS and ARCI before dosing, at +2 h postdosing (just before administration of the cognitive test battery), +4 h, and +6 h postdosing. The dosing was followed by 90 min during which the participants were supervised and asked not to sleep. At +2 h, the participants completed the spatial working memory and Spatial Span memory tasks as part of a broader cognitive battery (the data for which are not reported here). Finally, participants were assessed by a doctor before discharge.
Statistics
The data were analyzed using the Statistical Package for Social Scientists version 12.0 (SPSS). Ratings data from the VAS and ARCI subscales were analyzed with repeated measures analysis of variance (ANOVA) with gender and treatment order (placebo/THC and THC/placebo) as between-subject factors, treatment as a within-subject factor (placebo, THC 5 mg), and time as a within-subject factor (baseline, +2, +4, and +6 h). Between-subject errors and within-search errors from the Spatial Working Memory task were analyzed with repeated measure ANOVA with gender and treatment order as between-subject factors, and treatment and difficulty (four, six, and eight boxes) as within-subject factors. The strategy scores from the Spatial Working Memory task, and span scores, total errors, and total usage errors from the Spatial Span task were analyzed with a repeated measures ANOVA with gender and treatment order as between-subject factors, and treatment as the single within-subject factor. The index of variation presented in the tables and figures is always the standard error of the mean. Pearson's correlation coefficients were calculated to examine associations involving between-search errors (summed over the six- and eight-box levels of difficulty) and strategies on the Spatial Working Memory task; and between span, total errors and total usage errors from the Spatial Span task, marijuana effects (ARCI (M) scale), and mental sedation (VAS (M) scale) at +2 h postdosing with THC.
RESULTS
All participants tested negative for alcohol and other illicit drugs, and were able to tolerate six dose increments (as described above), to receive the full dose of 5 mg THC.
Subjective Effects
ARCI
Participants reported typical, if variable, subjective effects associated with THC treatment. First, THC significantly increased self-reported marijuana effects compared to placebo (1.30±0.46 vs 0.42±0.28) (F(1, 15)=9.32, p<0.01), with a trend for this effect to be maximal at +2 h onward (see Figure 1; M scale) (F(3, 45)=2.57, p=0.07). Sedative effects were also increased but not significantly so (Figure 1; PCAG scale) (F(1, 15)=2.90). There was no indication that THC induced euphoria in comparison with placebo (Figure 1; MBG scale) (F<1.00) or that it produced stimulant effects (Figure 1; BG and A scales) (both F's<1.00). However, THC tended to enhance dysphoria and somatic effects (see Figure 1; LSD effects) (F(1, 15)=4.53, p=0.05), and particularly so in the female (2.45±0.54 to 3.55±0.37) compared to male participants (3.33±0.40 to 3.33±0.27) (F(1, 15)=4.53, p=0.05).

Mean self-report scores (±SEs) on scales of the ARCI (Haertzen and Hickey, 1987) following 5 mg THC and placebo. Marijuana scale (M); Pentobarbital–Chlorpromazine–Alcohol (PCAG) scale; Morphine–Benzedrine scale (MBG); Amphetamine scale (A); Benzedrine-Group (BG) scale; and Lysergic acid (LSD) scale.
VAS
THC treatment was associated with significantly higher ratings of mental sedation compared to placebo treatment (154.41±16.12 vs 108.57±13.17) (F(1, 15)=7.26, p<0.05), increasing significantly over +6 h after treatment with THC while remaining unchanged after treatment with placebo (see Figure 2; F(3, 45)=5.25, p<0.005). Female participants also reported greater increases in mental sedation (82.45±21.25 to 172.00±26.12) compared to male participants (134.69±15.56 to 136.81±19.12) (F(1, 15)=6.60, p<0.05). Physical sedation also tended to increase after THC compared to placebo (114.54±11.96 vs 144.00±15.75) (F(1, 15)=3.84, p=0.07), with some indication that this increase was maximal at +4 h postdosing (Figure 2; F(3, 45)=2.64, p=0.06). Feelings of tranquility increased after THC treatment compared with placebo treatment (see Figure 2; 83.50±6.88 vs 98.85±9.57) (F(1, 15)=5.26, p<0.05), the more so in female (72.05±11.11 to 100.99±15.44) compared to male participants (94.95±8.13 to 96.70±11.30) (F(1, 15)=4.13, p=0.06). Finally, sociability did not change following placebo but tended to increase following THC treatment (Figure 2; F(3, 45)=2.49, p=0.07).

Mean self-report scores (±SE) on four scales of the VAS for drug effects (VAS; Bond and Lader, 1974) following administration of 5 mg THC and placebo. Mental sedation (M); physical sedation (P); feelings of tranquility; and other feelings of sociability (S).
Spatial Working Memory
Treatment with 5 mg THC significantly reduced the number of between-search errors (ie number of returns to open a box in which a counter had already been found on the same trial) committed while performing the Spatial Working Memory task in comparison to placebo (3.09±0.70 vs 4.91±0.95) (F(1, 15)=8.92, p<0.01). This improvement was most apparent at the highest level of difficulty (F(2, 30)=5.82, p<0.01). In general, the effects of THC on the between-search errors were evident in female (7.57±1.53 vs 3.35±1.13) but not male participants (2.25±1.12 vs 2.83±0.82), so that the two-way interaction between treatment and gender was highly significant (F(1, 15)=15.57, p<0.005). Moreover, the greater impact of THC (relative to placebo) on the between-search errors of female compared to male participants was most apparent with the largest search set sizes, so that the three-way interaction between treatment, gender, and difficulty was also significant (Figure 3; F(2, 30)=7.32, p<0.005).

Mean between-search errors (±SEs) on the Spatial Working Memory test (Cambridge Cognition Ltd, 1999) as a function of search set size following administration of 5 mg THC and placebo. Male and female volunteers.
Participants who first completed the Spatial Working Memory task after being treated with placebo showed a reduced number of between-search errors when subsequently completing the task after being treated with THC (7.21±1.44 vs 2.67±1.06) compared to participants who first completed the task with the reverse treatment order (2.61±1.23 vs 3.52±0.90) (F(1, 15)=20.07, p<0.001).
Within-search errors (ie the number of returns to boxes previously checked and shown to be empty earlier in the same search sequence) were not significantly altered after treatment with THC compared to treatment with placebo (0.24±0.09 vs 0.11±0.51) (F(1, 15)=2.21). Neither was there any significant interactions involving treatment, gender, and difficulty. Finally, there was no significant difference between overall strategy scores after THC compared to placebo treatment (26.93±1.51 vs 28.06±1.44) (F<1.00). However, female participants who completed the task first after placebo treatment showed improved strategy scores when completing the task again after THC (35.00±3.93 vs 26.50±4.12) compared to females who completed the task with the reverse treatment order (24.60±2.49 vs 27.20±2.61). By contrast, there were no significant differences between the strategy scores after THC and placebo in male participants who completed the task in either treatment order (25.13±1.96 vs 27.25±2.10 and 27.50±2.78 vs 26.75±2.91, respectively). This was reflected in a significant three-way interaction between treatment, treatment order, and gender (F(1, 15)=8.43, p<0.05).
Finally, there was a significant association between participants' strategy scores and the between-search errors summed over the six- and eight-box levels of difficulty after placebo treatment (r(19)=0.74, p<0.001) and a trend for a similar association apparent after THC treatment (r(19)=0.42, p=0.07). Additionally, the between-search errors after THC treatment were also significantly associated with the degree of mental sedation as measured by the VAS at +2 h dosing (r(19)=0.48, p<0.05).
Spatial Span
The maximum memory span reached on the Spatial Span task was not significantly altered following THC treatment compared to placebo treatment (6.73±0.39 vs 7.01±0.27) (F<1.00) in either the male or female participants, so that the two-way interaction between treatment and gender was not significant (see Figure 4; F<1.00). However, the total number of errors was significantly reduced after THC treatment compared to placebo treatment in the male participants (F(1, 10)=6.92, p<0.05) but increased in the female participants (F(1, 5)=6.18, p=0.06), so that the two-way interaction between treatment and gender was significant (Figure 4; F(1, 15)=10.74, p<0.01). The total usage errors (ie the number of times volunteers touched a square that was not part of the to-be-recalled spatial sequence) was significantly increased after THC compared to placebo (3.29±0.85 vs 2.17±0.67) (F(1, 15)=5.86, p<0.05). There was also a trend for this increase to be greater in female participants compared to male participants (see Figure 4; F(1, 15)=3.54, p=0.08). Finally, there were no significant correlations between spatial span, total errors, or total usage errors and either marijuana effects measured by the ARCI (M) scale or mental sedation as measured by the VAS at +2 h postdosing with THC.

Performance of the Spatial Span test (Cambridge Cognition Ltd, 1999) following administration of 5 mg THC and placebo. Spatial span; total number of errors; and total usage errors.
DISCUSSION
The principal findings of this study are that (i) a sublingual 5 mg dose of THC reduced the number of search errors while performing a self-ordered spatial working memory task (compared to placebo) in female but not male participants; (ii) there was little overall effect on the strategy employed by participants when completing the task; (iii) THC did not reduce the maximal number of spatial cues that volunteers could reproduce (‘span’) in a Spatial Span task; (iv) THC reduced the number of errors in reproducing spatial sequences in male participants but increased them for female participants during the Spatial Span task; and (v) THC increased the number of occasions that all participants produced spatial cues not included in the original sequences of the Spatial Span task. Before considering the significance of these results, we consider some methodological issues that are relevant to interpretation.
First, the sublingual dose of THC produced broadly typical, if variable, effects that are characteristic of cannabis administration. Specifically, the ratings on the ARCI demonstrated statistically significant marijuana-like effects (as measured by the M scale) in the absence of euphoria (BG scale) or stimulant-like effects (A and MBG scales). Consistent with previous studies, THC also increased dysphoria and somatic symptoms (LSD scale) (Kirk and DeWit, 1999) and produced mild but significant sedative effects, as well as increased feelings of tranquility (VAS). All of these effects were maximal at about the time the participants completed the memory tasks (+2 h; cf. Kirk et al, 1998), making it at least possible that the cognitive effects of the THC treatment reflect (in part) nonspecific changes in subjective state. This possibility is strengthened by the observation that the subjective effects (such as those reflected in the LSD scale and sedative subscales) were significantly enhanced in female compared to male participants, perhaps reflecting their more limited prior experience of cannabis as estimated by their number of lifetime uses. On the other hand, it is clear that the current results are not simply attributable to changes in subjective state since the male participants experienced these effects also but showed only minimal performance changes, while THC had complex effects on spatial memory with some dependent measures (between-search errors) being reduced but others increased (total usage errors).
Second, THC produced more marked effects on the spatial memory of female participants compared to male participants, reflecting the generally poorer performance of the former group compared to the latter group. Importantly, this effect cannot easily be attributed to differences in treatment order such that more female than male participants completed the Spatial Working Memory and Spatial Span tasks first after placebo and then again after THC treatment. In this case, reduced between-search errors in females following THC might reflect only improved performance associated with task practice. In this study, gender was allowed to vary randomly with recruitment but, in fact, only two out of seven females completed the memory tasks first after placebo and again after THC compared to eight out of 12 male participants. Therefore, it is unlikely that the greater effects of THC on the memory scores of the female participants compared to male participants can be attributed to confounded practice effects. However, we do acknowledge that further experimentation is needed to examine systematically potential interactions involving THC and placebo treatments, treatment order, and gender.
Gender differences in memory function continues to attract significant investigation and controversy, with recent evidence suggesting a male advantage in relational/route-finding function (Brown et al, 1998) but a disadvantage in verbal and episodic memory (Herlitz et al, 1997). Recently, a consensus has emerged that gender-differences likely reflect a mixture of differences in abilities and the impact of psychosocial factors such as differential training in specific cognitive domains (Stumpf, 1995). Particularly pertinent to the current data are observations that males show an advantage in number ability, space orientation, and space visualization (Stumpf, 1995) that may reflect differences in the functional organization of anterior cortical systems responsible for working memory (Speck et al, 2002). It seems likely that the greater effects of THC on the memory scores of female compared to male participants is consistent with observations that pharmacological effects depend upon the level of baseline performance of participants under placebo, and are greatest in those whose baseline scores allow greater room for change (Kimberg and D'Esposito, 2003; Luciana et al, 1992; Miller et al, 1977).
The present study demonstrates divergent effects of a low dose of THC on aspects of spatial memory, with some indication that relatively poor performance of a self-ordered spatial search can be improved while items reproduced during simple recall of a spatial span include some not in the original sequence (ie intrusion errors). Our data also highlight the possibility that THC has effects on working memory systems mediated by anterior cortical as well as hippocampal systems (eg Heyser et al, 1993). Broadly, there are two possible pharmacological explanations for the THC effects on spatial memory in the current study. First, these effects may be mediated directly by increased CB1 receptor activity within the lateral PFC itself or CB1 receptors within the broader interconnected circuitry including, for example, the basal ganglia and hippocampus that help mediate working memory function.
Secondly, it may be that the increase in DA activity within the PFC consequent to THC intake (Diana et al, 1998; Jentsch et al, 1997) is just enough to facilitate the performance of the self-ordered spatial search (in the Spatial Working Memory test; cf. the facilitatory effects of methylphenidate on the same task; Elliott et al, 1997) but at the expense of an increased number of intrusions in the recall of spatial sequences (in the Spatial Span test). In this case, the findings that THC has more marked effects on the spatial memory of female compared to male participants is in line with observations that females show greater susceptibility to the behavioral, and sensitizing, effects of psychostimulants (Becker et al, 2001), lending support to the proposal that THC affects spatial memory through catecholaminergic mechanisms. Finally, if the present findings were mediated by predominantly CB1 activity, then they could be blocked by administration of the CB1 receptor antagonist, SR141716A; however, if they arise through catecholamine activity, they could be countered by manipulations that challenge DA activity.
At a neuropsychological level of analysis, one conception of working memory posits that dorsolateral and ventrolateral PFC sectors (above and below the principal sulcus, respectively) support the same cognitive/mnemonic function with different types of information (dorsolateral PFC → spatial information; ventrolateral PFC → object-based information; Courtney et al, 1997). By contrast, another proposal posits that dorsolateral PFC is critical for the manipulation of stored information of all kinds (spatial or object based), while ventrolateral PFC mediates the relatively more straightforward retrieval and output of already sequenced information (Petrides, 1996; Owen, 1997). The current results suggest that THC facilitates the actions of the dorsolateral PFC but impairs the actions of ventrolateral PFC. Research might attempt further pharmacological dissociation by examining whether low doses of THC have greater or comparable effects on the manipulation and recall of spatial vs object-based working memory.
Finally, the finding that THC increased the number of recalled cues that were not part of the original to-be-recalled spatial sequences in the Spatial Span task is reminiscent of the increased frequency of intrusions by which THC induces participants to recall falsely items that were not part of encoded word lists in free recall experiments (Dornbush et al, 1971; Hooker and Jones, 1987). Miller and Branconnier (1983) have suggested that this effect reflects failure to habituate to extraneous or irrelevant information, increasing the chances that it will be included as part of the list to-be-recalled. Alternatively, intrusions may reflect a weakening of associative links between encoded items, instead promoting new associations that could prompt intrusive errors (Block et al, 1992). Performing the Spatial Span task involves representing the order of presented cues, ready for recall. The current data suggest that while THC did not reduce the maximum ‘span’ of correctly recalled sequences, it did compromise the representation of which cues belong in the sequence and which do not, thereby increasing intrusions when recalling sequences of even abstract, austere spatial cues of the kind used here. In summary, the present data suggest that low doses of THC have both beneficial and detrimental effects on the spatial memory of healthy human subjects, perhaps facilitating the manipulation of information but impairing the interstimulus associations that would otherwise promote accurate recall.
References
Ameri A (1999). The effects of cannabinoids on the brain. Progr Neurobiol 58: 315–348.
Arnsten AF, Contant TA (1992). Alpha-2 adrenergic agonists decrease distractibility in aged monkeys performing the delayed response task. Psychopharmacology 108: 159–169.
Arnsten AFT (2000). Catecholamine modulation of prefrontal cortical cognitive function. Trends Cogn Sci 2: 436–447.
Arnsten AFT, Cai JX, Murphy BL, Goldman-Rakic PS (1994). Dopamine D1 receptor mechanisms in the cognitive performance of young adult and aged monkeys. Psychopharmacology 116: 143–151.
Arnsten AFT, Cai JX, Steere JC, Goldman-Rakic PS (1995). Dopamine D2 receptor mechanisms contribute to age-related cognitive decline: the effects of quinpirole on memory and motor performance in monkeys. J Neurosci 15: 3429–3439.
Arnsten AFT, Jentsch JD (1997). The alpha-1 adrenergic agonist, cirazoline, impairs spatial working memory. Pharmacol Biochem Behav 57: 1–5.
Barch DM (2004). Pharmacological manipulation of human working memory. Psychopharmacology 174: 126–135.
Becker JB, Molenda H, Hummer DL (2001). Gender differences in the behavioral responses to cocaine and amphetamine. Implications for mechanisms mediating gender differences in drug abuse. Ann NY Acad Sci 937: 172–187.
Birnbaum SG, Podell DM, Arnsten AFT (2000). Noradrenergic alpha-2 receptor agonists reverse working memory deficits induced by the anxiogenic drug, FG7142, in rats. Pharmacol Biochem Behav 67: 397–403.
Block RI, Farinpour R, Braverman K (1992). Acute effects of marijuana on cognition: relationships to chronic effects and smoking techniques. Pharmacol Biochem Behav 43: 907–917.
Bond A, Lader M (1974). The use of analogue scales in rating subjective feelings. Br J Med Psychol 47: 211–218.
Brown LN, Lahar CJ, Mosley JL (1998). Age and gender-related differences in strategy use for route information: a ‘map-present’ direction-giving paradigm. Environ Behav 30: 123–143.
Brozoski TJ, Brown RM, Rosvold HE, Goldman P (1979). Cognitive deficits caused by regional distribution of dopamine in prefrontal cortex in rhesus monkey. Science 205: 929–931.
Casswell S, Marks DF (1973). Cannabis and temporal disintegration in experienced and naive subjects. Science 179: 803–805.
Chait LD, Perry JL (1994). Acute and residual effects of alcohol and marijuana, alone and in combination, on mood and performance. Psychopharmacology 115: 340–349.
Collins P, Roberts AC, Dias R, Everitt BJ, Robbins TW (1998). Perseveration and strategy in a novel spatial self-ordered sequencing task for nonhuman primates: effects of excitotoxic lesions and dopamine depletions of the prefrontal cortex. J Cogn Neurosci 10: 332–354.
Coull JT, Middleton HC, Robbins TW, Sahakian BJ (1995). Contrasting effects of clonidine and diazepam on tests of working memory and planning. Psychopharmacology 120: 311–321.
Courtney SM, Ungerleider LG, Keil K, Haxby JV (1997). Transient and sustained activity in a distributed neural system for human working memory. Nature 386: 608–611.
Curran HV, Brignell C, Fletcher S, Middleton P, Henry J (2002). Cognitive and subjective dose–reponse effects of acute oral Δ9-tetrahydrocannabinol (THC) in frequent users. Psychopharmacology 164: 61–70.
Diana M, Melis M, Gessa GL (1998). Increase in meso-prefrontal dopaminergic activity after stimulation of CB1 receptors by cannabinoids. Eur J Neurosc 10: 2825–2830.
Dornbush RL, Fink F, Freedman AJ (1971). Marijuana, memory and perception. Am J Psychiatry 128: 194–197.
D'Souza DC, Perry E, MacDougall L, Ammerman Y, Cooper T, Wu YT et al (2004). The psychomimetic effects of intravenous delta-9-tetrahydrocannabinol in healthy individuals: implications for psychosis. Neuropsychopharmacology 29: 1558–1572.
Elliott R, Sahakian BJ, Matthews K, Bannerjea A, Rimmer J, Robbins TW (1997). Effects of methylphenidate on spatial working memory and planning in healthy young adults. Psychopharmacology 131: 105–111.
Fuster JM (1989). The Prefrontal Cortex. Raven Press: New York.
Guy GW, Robson PJ (2003). A Phase I, double-blind, three-way crossover study to assess the pharmacokinetic profile of cannabis based medicine extract (CBME) administered sublingually in variant cannabinoid ratios in normal healthy volunteers (GWPK0215). J Cannabis Therap 3: 121–152.
Haertzen CH, Hickey JE (1987). Addiction Research Center Inventory (ARCI): measurement of euphoria and other drug effects. In: Bozarth MA (ed). Methods of Assessing the Reinforcing Properties of Abused Drugs. Springer-Verlag: New York. pp 489–524.
Hampson RE, Deadwyler SA (1999). Cannabinoids, hippocampal function in memory. Life Sci 65: 715–723.
Hampson RE, Deadwyler SA (2000). Cannabinoids reveal the necessity of hippocampal neural encoding for short-term memory in rats. J Neurosci 20: 8932–8942.
Heishman SL, Arasteh K, Stitzer ML (1997). Comparative effects of alcohol and marijuana on mood, memory, and performance. Pharmacol Biochem Behav 58: 93–101.
Herkenham M, Lynn AB, Little MD, Johnson MR, Melvin LS, deCosta BR et al (1990). Cannabinoid receptor localization in brain. Proc Natl Acad Sci 87: 1932–1936.
Herlitz A, Nilsson LG, Baeckman L (1997). Gender differences in episodic memory. Mem Cogn 25: 801–811.
Heyser CJ, Hampson RE, Deadwyler SA (1993). The effects of delta-9-THC on delayed match to sample performance in rats: alterations in short-term memory produced by changes in task specific firing of hippocampal neurones. J Pharmacol Exp Ther 264: 294–307.
Hollister LE (1986). Health aspects of cannabis. Pharmacol Rev 38: 1–20.
Hooker WD, Jones RT (1987). Increased susceptibility to memory intrusions and Stroop interference effect during acute marijuana intoxication. Psychopharmacology 91: 20–24.
Jakala P, Riekkinen M, Sirvio J, Koivisto E, Kejonen K, Vanhanen M et al (1999). Guanfacine, but not clonidine, improves planning and working memory performance in humans. Neuropsychopharmacology 20: 460–470.
Jentsch JD, Andrusiak E, Tran A, Bowers Jr MB, Roth RH (1997). Delta 9-tetrahydrocannabinol increases prefrontal cortical catecholaminergic utilization and impairs spatial working memory in the rat: blockade of dopaminergic effects with HA966. Neuropsychopharmacology 16: 426–432.
Kimberg DY, D'Esposito M (2003). Cognitive effects of the dopamine receptor agonist pergolide. Neuropsychologia 41: 1020–1027.
Kimberg DY, D'Esposito M, Farah MJ (1997). Effects of bromocriptine on human subjects depend on working memory capacity. Neuroreport 8: 3581–3585.
Kirk JM, DeWit H (1999). Responses to oral Δ9-tetrahydrocannabinol in frequent and infrequent marijuana users. Pharmacol Biochem Behav 63: 137–142.
Kirk JM, Doty P, DeWit H (1998). Effects of expectancies on subjective responses to oral Δ9-tetrahydrocannabinol. Pharmacol Biochem Behav 59: 287–293.
Lange KW, Robbins TW, Marsden CD, James M, Owen AM, Paul GM (1992). L-DOPA withdrawal selectively impairs performance in tests of frontal lobe function in Parkinson's disease. Psychopharmacology 107: 394–404.
Lezak MD (1995). Neuropsychological Assessment, 3rd edn. Oxford University Press: New York.
Lichtman AH, Martin BR (1996). Delta 9-tetrahyrdocannabinol impairs spatial memory through a cannabinoid receptor mechanism. Psychopharmacology 126: 125–131.
Luciana M, Depue RA, Arbisi P, Leon A (1992). Facilitation of working memory in humans by a D2 dopamine receptor agonist. J Cogn Neurosci 4: 58–68.
Mallet PE, Beninger RJ (1998). The cannabinoid CB1 receptor antagonist SR141716A attenuates the memory impairment produced by delta 9-tetrahydrocannabinol. Psychopharmacology 140: 11–19.
Mehta MA, Manes F, Magnolfi G, Sahakian BJ, Robbins TW (2004). Impaired set-shifting and dissociable effects on tests of spatial working memory following the dopamine D2 antagonist, sulpiride, in human volunteers. Psychopharmacology 176: 331–342.
Mehta MA, Owen AM, Sahakian BJ, Mavaddat N, Pickard JD, Robbins TW (2000). Methylphenidate enhances working memory by modulating discrete frontal and parietal lobe regions in the human brain. J Neurosci 20: RC65.
Mehta MA, Swainson R, Ogilvie AD, Sahakian BJ, Robbins TW (2001). Improved short-term spatial memory but impaired reversal learning following the dopamine D2 agonist bromocriptine in human volunteers. Psychopharmacology 159: 10–20.
Miller LL, Branconnier RJ (1983). Cannabis: effects on memory and the cholinergic system. Psychol Bull 93: 441–456.
Miller LL, McFarland DJ, Cornett TL, Brightwell DR, Wilker A (1977). Marijuana: effects on free recall and subjective organization of pictures and words. Psychopharmacology 55: 257–262.
Milner B (1971). Interhemispheric differences in the localisation of psychological processes in man. Br Med Bull 27: 272–277.
Müller U, von Cramon DY, Pollman S (1998). D1 versus D2 receptor modulation of visuospatial working memory in humans. J Neurosci 18: 2720–2728.
Nelson HE (1982). National Adult Reading Test Manual. NFER-Nelson: Windsor, Berks.
Owen AM (1997). The functional organization of working memory processes within human lateral frontal cortex: the contribution of functional neuroimaging. Eur J Neurosci 9: 1329–1339.
Owen AM, Downes JJ, Sahakian BJ, Polkey CE, Robbins TW (1990). Planning and spatial working memory following frontal lobe lesions in man. Neuropsychologia 28: 1021–1034.
Owen AM, Evans AC, Petrides M (1996a). Evidence for a two-stage model of spatial working memory processing within lateral frontal cortex: a positron emission tomography study. Cerebr Cortex 6: 31–38.
Owen AM, Morris RG, Sahakian BJ, Polkey CE, Robbins TW (1996b). Double dissociations of memory and executive functions in working memory tasks following frontal lobe excisions, temporal lobe excisions or amygdalo-hippocampectomy in man. Brain 119: 1597–1615.
Petrides M (1996). Specialized systems for the processing of mnemonic information within the primate frontal cortex. Philos Trans R Soc Lond: Biol Sci 351: 1455–1461.
Petrides M, Milner B (1982). Deficits on subject-ordered tasks after frontal- and temporal-lobe lesions in man. Neuropsychologia 20: 249–262.
Robbins TW (1996). Dissociating executive functions of the prefrontal cortex. Philos Trans R Soc Lond: Biol Sci 351: 1463–1470.
Roberts AC, DeSalvia M, Wilkinson LS, Collins P, Muir JL, Everitt BJ et al (1994). 6-Hydroxydopamine lesions of the prefrontal cortex in monkeys enhance performance on an analogue of the Wisconsin Card Sorting Test: possible interactions with subcortical dopamine. J Neurosci 14: 2531–2544.
Sawaguchi T, Goldman-Rakic PS (1991). D1 dopamine receptors in prefrontal cortex. Science 251: 947–950.
Speck O, Ernst T, Braun J, Koch C, Miller E, Chang L (2002). Gender differences in the functional organization of the brain for working memory. Neuroreport 11: 2581–2585.
Stumpf H (1995). Gender differences in performance on tests of cognitive abilities: Experimental design issues and empirical results. Learn Individ Differ 7: 275–287.
Varvel SA, Lichtman AH (2002). Evaluation of CB1 receptor knockout mice in the Morris water maze. J Pharmacol Exp Ther 301: 915–924.
Verrico CD, Jentsch JD, Dazzi L, Roth RH (2003). Systemic, but not local, administration of cannabinoid CB1 receptor agonists modulate prefrontal cortical acetycholine efflux in the rat. Synapse 48: 178–183.
Wang M, Vijayraghavan S, Goldman PS (2004). Selective D2 receptor actions on the functional circuitry of working memory. Science 303: 853–856.
Williams GV, Goldman-Rakic PS (1995). Blockade of dopamine D1 receptors enhances memory fields of prefrontal neurones in primate cerebral cortex. Nature 376: 572–575.
Zhang K, Grady CJ, Tsapakis EM, Anderson SL, Tarazi FI, Baldessarini RJ (2004). Regulation of working memory by dopamine D4 receptor in rats. Neuropsychopharmacology 29: 1648–1655.
Acknowledgements
This research was funded by an independent grant from GW Pharmaceuticals Plc to Robert D Rogers. Zubin Bhagwagar was funded by an MRC Clinical Training Fellowship.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Makela, P., Wakeley, J., Gijsman, H. et al. Low Doses of Δ-9 Tetrahydrocannabinol (THC) Have Divergent Effects on Short-Term Spatial Memory in Young, Healthy Adults. Neuropsychopharmacol 31, 462–470 (2006). https://doi.org/10.1038/sj.npp.1300871
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.npp.1300871
Keywords
This article is cited by
-
Chronic adolescent exposure to cannabis in mice leads to sex-biased changes in gene expression networks across brain regions
Neuropsychopharmacology (2022)
-
Sex differences in the acute effects of intravenous (IV) delta-9 tetrahydrocannabinol (THC)
Psychopharmacology (2022)
-
Visuospatial Processing Decline Due to Cannabis Consumption in Nondependent High School Students
Educational Psychology Review (2021)
-
Cannabis Use: Neurobiological, Behavioral, and Sex/Gender Considerations
Current Behavioral Neuroscience Reports (2018)
-
Are adolescents more vulnerable to the harmful effects of cannabis than adults? A placebo-controlled study in human males
Translational Psychiatry (2016)
