
Abstract
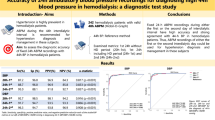
The purpose of our study was to evaluate the behaviour of blood pressure (BP) by ambulatory monitoring of blood pressure (AMBP) in 53 patients with primary hyperparathyroidism (PHPT) compared to 100 essential hypertensive (EH) and 31 healthy subjects (HS). The correlations between calcium–phosphorus metabolism and haemodynamic parameters in all groups are included in the study. AMBP was performed using the oscillometric technique (Space-Labs, 90207, Redmond, WA, USA) and the following AMBP parameters were evaluated: average day time systolic (S) and diastolic (D) blood pressure (BP) and heart rate (HR) (when awake), average night time SBP, DBP and HR (when asleep) and average 24-h-SBP, DBP and HR. The definition of ‘dipper’ or ‘non-dipper’ subjects was established if night time SBP and DBP fall was >10% and <10%, respectively. In total, 25 PHPT patients (47.2%) were hypertensive (HT-PHPT) and 28 PHPT (52.8%) were normotensive (NT-PHPT). Mean 24-h-SBP and DBP obtained by AMBP was higher in HT-PHPT (P<0.05) and EH (P<0.05) than in NT-PHPT and HS. The multiple linear regression has shown that in PHPT-HT patients ionized calcium is an independent factor for the rise of 24-h-DBP values (r: 0.497; P<0.05) and daytime DBP values (r: 0.497; P<0.05). In 56% of HT-PHPT patients there is an absence of physiological BP nocturnal fall (‘non-dipper’), which is statistically significant (P<0.05) compared with ‘non-dipper’ EH patients (30%). In conclusion, in our study the prevalence of hypertension in PHPT was 47%. AMBP revealed that the ‘non-dipping ‘pattern was much higher in HT-PHPT patients in respect to EH patients.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 digital issues and online access to articles
$119.00 per year
only $9.92 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

References
Boonen S et al. Primary hyperparathyroidism: pathophysiology, diagnosis and indications for surgery. Acta Oto-Rhino-Laryngol Belg 2001; 55: 119–127.
Kaplan EL, Yashro T, Salti G . Primary hyperparathryrodism in the 1990s. Ann Surg 1992; 215: 300–317.
Dominiczak AF, Lyall F, Morton JJ . Blood pressure, left ventricular mass and intracellular calcium in primary hyperparathyroidim. Clin Sci 1990; 78: 127–132.
Fardella C, Rodriguez-Portales JA . Intracellular calcium and blood pressure: comparison between primary hyperparathyroidism and essential hypertension. J Endocrinol Invest 1995; 18: 827–832.
Sangal AK, Beevers DG . Parathyroid hypertension. Br Med J 1983; 286: 498–499.
Nilson IL et al. Circadian cardiac autonomic dysfunction in primary hyperparathyridism improves after parathyroidectomy. Surgery 2003; 134 (6): 1013–1019.
Rosental FD, Roy S . Hypertension and hyperparathyroidism. Br Med J 1972; 4: 396–397.
Hellstrom J, Birke G, Edvall CA . Hypertension in hyperparathyroidism. Br J Urol 1958; 30: 13–24.
Dalberg K et al. Cardiac function in primary hyperparthyroidism before and after operation-an echocardiographic study. Eur J Surg 1996; 162: 171–176.
Millar-Graig MW, Bishop CN, Raftery EB . Circadian variation of blood pressure. Lancet 1978; 1: 795–797.
Littler WA et al. Sleep and blood pressure: further observations. Am Heart J 1979; 97: 35–37.
Mancia G et al. Blood and heart rate variabilities in normotensive and hypertensive human beings. Circ Res 1983; 53: 96–104.
Weber MA et al. The circadian blood pressure pattern in ambulatory normal subjects. Am J Cardiol 1984; 45: 115–119.
Harshfield GA, Hwang C, Grim CE . Circadian variation of blood pressure in blacks: influence of age, gender and activity. J Hum Hypertens 1990; 4: 43–47.
Mancia G et al. Blood pressure control in the hypertensive population. Lancet 1997; 349: 454–457.
Middeke M, Schrader J . Nocturnal blood pressure in normotensive subjects and those with white coat, primary, and secondary hypertension. BMJ 1994; 308: 630–632.
White WB et al. Ambulatory blood pressure monitoring: dippers compared with non-dippers. Blood Press. Monit. 2000; 5 (Suppl 1): 517–523.
O’Brien E, Sheridan J, O’Malley K . Dippers and non-dippers. Lancet 1988; 2: 397.
Middeke M, Klugich M, Holzgreve H . Circadian blood pressure rhythm in primary and secondary hypertension. Chronobiol Int 1991; 8: 451–459.
Imai Y et al. Does ambulatory blood pressure monitoring improve the diagnosis of secondary hypertension? J Hypertens Suppl 1990; 8 (6): S71–S75.
Kluglich M, Middeke M . Circadian blood pressure rhythm in hyperthyroidism and hyperparathyroidism. Z Kardiol 1992; 81 (Suppl 2): 33–36.
O’Brien E et al. Accuracy of the Space Labs 90207 determined by the British Hypertension Society protocol. J Hypertens 1991; 9: 573–574.
Verdecchia P et al. Ambulatory blood pressure: an independent predictor of prognosis in essential hypertension. Hypertension 1994; 24: 793–801.
Verdecchia P, Porcellati C . Definiting normal ambulatory blood pressure in relation to target organ damage and prognosis. Am J Hypertens 1993; 6: 207S–210S.
Mallion JM et al. Day and night blood pressure values in normotensive and essential hypertensive subjects assessed by 24-hours ambulatory monitoring. J Hypertens 1990; 8 (Suppl 6): S49–S55.
Lind L et al. Hypertension in primary hyperparathyroidism in relation to histopathology. Eur J Surg 1991; 157: 457–459.
Resnick LM et al. Calcium metabolism in hypertension and allied metabolic disorders. Diabetes Care 1991; 14 (6): 505–520.
Richards AM et al. Hormone, calcium and blood pressure relationships in primary hyperparathyroidism. J Hypertens 1988; 6: 747–752.
Schiffl H, Sitter T, Lang SM . Noradrenergic blood pressure dysregulation and cytosolic calcium in primary hyperparathyroidism. Kid Blood Press Res 1997; 20: 290–296.
Fliser D et al. Subacute infusion of physiological doses of parathyroid hormone raises blood pressure in humans. Nephrol Dial Transplant 1997; 12: 933–938.
Lind L, Ljunghall S . Parathyroid hormone and blood pressure—is there a relationship? Nefrol Dial Transplant 1995; 13 (4): 433–438, Editorial comments.
Brinton GS, Jubiz W, Lagerquist LD . Hypertension in primary hyperparathyroidism: the role of the renin–angiotensin system. J Clin Endocrinol Metab 1975; 41: 1025–1029.
Gennari C, Nami R, Gonnelli S . Hypertension and primary hyperparathyroidism: the role of adrenergic and renin–angiotensin–aldosterone systems. Miner Electrol Metab 1995; 21: 77–81.
Ganguly A et al. The renin–angiotensin–aldosterone sistems and hypertension in primary hyperparathyroidism. Metabolism 1982; 31 (6): 595–600.
Lakatos P et al. Endothelin concentrations are elevated in plasma of patients with primary and secondary hyperparathyroidism. Calcif Tiss Int 1996; 58: 70–71.
Letizia C et al. Adrenomedullin concentrations are elevated in plasma of patients with primary hyperparathyroidism. Metabolism 2003; 52: 159–162.
Halberg F, Tong YL, Johnson EA . Circadian system phase: an aspect of morphology: procedures and illustrative examples. In: Von Mayersbach (ed). The Cellular Aspects of Biorhythms. Springer-Verlag: Berlin, 1967, pp 20–48.
Verdecchia P et al. Blunted noctural fall in blood pressure in hypertensive women with future cardiovascular events [Abstract]. Circulation 1992; 86 (suppl 1): 1–678.
Shimada K et al. Diurnal blood pressure variations and silent cerebrovascular damage in elderly patients with hypertension. J Hypertens 1992; 10: 875–878.
Palatini P et al. Clinical relevance of night-time blood pressure and of day-time blood pressure variability. Arch Intern Med 1992; 152: 1855–1860.
Fogari R et al. Ambulatory blood pressure monitoring in normotensive and hypertensive type II diabetics: prevalence of impaired diurnal blood pressure patterns. Am J Hypertens 1993; 6: 1–7.
Acknowledgements
This work has been supported in part by Banca di Credito Cooperativo of Rome, Italy. We thank Mr Giovanni Clemente for his technical assistance.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Letizia, C., Ferrari, P., Cotesta, D. et al. Ambulatory monitoring of blood pressure (AMBP) in patients with primary hyperparathyroidism. J Hum Hypertens 19, 901–906 (2005). https://doi.org/10.1038/sj.jhh.1001907
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.jhh.1001907
Keywords
This article is cited by
-
Endocrine Causes of Hypertension
Current Hypertension Reports (2020)
-
Increased frequency of impaired fasting glucose and isolated systolic hypertension in Paget’s disease of bone
Endocrine (2019)
-
Ambulatory blood pressure monitoring-derived short-term blood pressure variability in primary hyperparathyroidism
Endocrine (2018)
-
Clinical Benefits of Unilateral Adrenalectomy in Patients with Subclinical Hypercortisolism Due to Adrenal Incidentaloma: Results from a Single Center
High Blood Pressure & Cardiovascular Prevention (2017)
-
Relationship Between Aldosterone and Parathyroid Hormone, and the Effect of Angiotensin and Aldosterone Inhibition on Bone Health
Clinical Reviews in Bone and Mineral Metabolism (2015)
