
Abstract
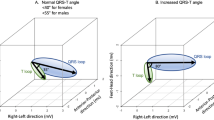
The sum of time–voltage QRS areas in the 12-lead electrocardiogram (ECG) has outperformed other 12-lead ECG indices for detection of left ventricular hypertrophy (LVH). We assessed indices of time–voltage QRS and T-wave (QRST) areas from body surface potential mapping (BSPM) for detection of and quantitation of the degree of LVH. We studied 42 patients with echocardiographic LVH (LVH group) and 11 healthy controls (controls). QRST area sums were calculated from 123-lead BSPM and from the 12-lead ECG for comparison. Leadwise discriminant indices and correlation coefficients were used to identify optimal recording locations for QRST area-based LVH assessment. BSPM QRS area sum was greater in the LVH group than in controls (3752 ± 1259 vs 2278 ± 627 μV s, respectively; P<0.001) and at 91% specificity showed 74% sensitivity for LVH detection. The 12-lead QRS area sum performed similarly. Taking T-wave areas into account did not improve the results. QRS area sum from two most informative leads (located in the upper and lower right precordium) also separated the LVH group from controls (61.1 ± 23.5 vs 27.8 ± 6.5 μV s, respectively; P<0.00001). This 2-lead QRS area sum showed 90% sensitivity with 100% specificity for LVH detection and maintained high correlation to indexed left ventricular mass (r=0.732; P<0.001). In conclusion, the BSPM QRS area sum compared to 12-lead QRS area sum does not substantially improve LVH assessment. The 2-lead QRS area sum may improve ECG QRS area-based LVH assessment.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 digital issues and online access to articles
$119.00 per year
only $9.92 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others
References
Casale PN et al. Value of echocardiographic measurement of left ventricular mass in predicting cardiovascular morbid events in hypertensive men. Ann Intern Med 1986; 105: 173–178.
Levy D et al. Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. N Engl J Med 1990; 322: 1561–1566.
Schillaci G et al. Continuous relation between left ventricular mass and cardiovascular risk in essential hypertension. Hypertension 2000; 35: 580–586.
Devereux RB et al. Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J Cardiol 1986; 57: 450–458.
Myerson SG, Bellenger NG, Pennell DJ . Assessment of left ventricular mass by cardiovascular magnetic resonance. Hypertension 2002; 39: 750–755.
Devereux RB, Pini R, Aurigemma GP, Roman MJ . Measurement of left ventricular mass: methodology and expertise. J Hypertens 1997; 15: 801–809.
Holland RP, Arnsdorf MF . Solid angle theory and the electrocardiogram: physiologic and quantitative interpretations. Prog Cardiovasc Dis 1977; 19: 431–457.
Surawicz B . Electrocardiographic diagnosis of chamber enlargment. J Am Coll Cardiol 1986; 8: 711–724.
Okin PM et al. Electrocardiographic diagnosis of left ventricular hypertrophy by the time–voltage integral of the QRS complex. J Am Coll Cardiol 1994; 23: 133–140.
Okin PM, Roman MJ, Devereux RB, Kligfield P . Time–voltage area of the QRS for the identification of left ventricular hypertrophy. Hypertension 1996; 27: 251–258.
Okin PM et al. Time–voltage QRS area of the 12-lead electrocardiogram. Detection of left ventricular hypertrophy. Hypertension 1998; 31: 937–942.
Kornreich F et al. Identification of best electrocardiographic leads for diagnosing left ventricular hypertrophy by statistical analysis of body surface potential maps. Am J Cardiol 1988; 62: 1285–1291.
Thiry PS, Rosenberg RM, Abbott JA . A mechanism for the electrocardiogram response to left ventricular hypertrophy and acute ischemia. Circ Res 1975; 36: 92–104.
Devereux RB, Reichek N . Repolarization abnormalities of left ventricular hypertrophy. Clinical, echocardiographic and hemodynamic correlates. J Electrocardiol 1982; 15: 47–54.
Okin PM et al, for The LIFE Study Investigators. Relationship of the electrocardiographic strain pattern to left ventricular structure and function in hypertensive patients: The LIFE Study. J Am Coll Cardiol 2001; 38: 514–520.
Sokolow M, Lyon TP . The ventricular complex in left ventricular hypertrophy as obtained by unipolar precordial and limb leads. Am Heart J 1949; 37: 161–168.
Sahn DJ, DeMaria A, Kisslo J, Weyman A . Recommendations regarding quantitation in M-mode echocardiography: results of a survey of echocardiographic measurements. Circulation 1978; 58: 1072–1083.
Liu JE, Devereux RB . Clinical assessment of cardiac hypertrophy. In: Sheridan DJ (ed). Left Ventricular Hypertrophy. Churchill-Livingstone: London, 1998, pp 11–16.
Reichek N, Devereux RB . Reliable estimation of peak left ventricular systolic pressure by M-mode echographic-determined end-diastolic relative wall thickness: identification of severe valvular aortic stenosis in adult patients. Am Heart J 1982; 103: 202–209.
Simelius K et al. A body surface potential mapping system in clinical use. Med Biol Eng Comput 1996; 34: 107–108.
Takala P et al. Magnetocardiographic and electrocardiographic exercise mapping in healthy subjects. Ann Biomed Eng 2001; 29: 501–509.
Hänninen H et al. ST-segment level and slope in exercise-induced myocardial ischemia evaluated with body surface potential mapping. Am J Cardiol 2001; 88: 1152–1156.
Simson MB . Use of signals in the terminal QRS complex to identify patients with ventricular tachycardia after myocardial infarction. Circulation 1981; 64: 235–242.
Oikarinen L et al. Magnetocardiographic QT interval dispersion in postmyocardial infarction patients with sustained ventricular tachycardia: validation of automated QT measurements. Pacing Clin Electrophysiol 1998; 21: 1934–1942.
Kornreich et al. Identification of best electrocardiographic leads for diagnosing anterior and inferior myocardial infarction by statistical analysis of body surface potential maps. Am J Cardiol 1986; 58: 863–871.
Altman DG . Comparing groups — continuous data. In: Altman DG (ed). Practical Statistics For Medical Research. Chapman & Hall: London, 1995, pp 179–228.
Macfarlane PW . Lead systems. In: Macfarlane PW, Lawrie TDV (eds). Comprehensive Electrocardiology. Pergamon Press: Oxford, 1989, pp 315–352.
Salton CJ et al. Gender differences and normal left ventricular anatomy in an adult population free of hypertension. A cardiovascular magnetic resonance study of the Framingham Heart Study offspring cohort. J Am Coll Cardiol 2002; 39: 1055–1060.
Kornreich F et al. Diagnostic body surface potential map patterns in left ventricular hypertrophy during PQRST. Am J Cardiol 1989; 63: 610–617.
Kornreich F et al. Improved prediction of left ventricular mass by regression analysis of body surface potential maps. Am J Cardiol 1990; 66: 485–492.
Holt JH, Barnard ACL, Lynn MS . A study of the human heart as a multiple dipole electrical source. II. Diagnosis and quantitation of left ventricular hypertrophy. Circulation 1969; 40: 697–710.
Holt JH, Barnard ACL, Kramer JO . Multiple dipole electrocardiography. A comparison of electrically and angiographically determined left ventricular masses. Circulation 1978; 57: 1129–1133.
Dunn RA et al. Performance of conventional orthogonal and multiple-dipole electrocardiograms in estimating left ventricular muscle mass. Circulation 1979; 60: 1350–1353.
Yamaki M et al. Improved diagnostic performance on the severity of left ventricular hypertrophy with body surface potential mapping. Circulation 1989; 79: 312–323.
Palmieri V et al. Reliability of echocardiographic assessment of left ventricular structure and function. The PRESERVE Study. J Am Coll Cardiol 1999; 34: 1625–1632.
Montague TJ et al. Isointegral analysis of body surface maps: surface distribution and temporal variability in normal subjects. Circulation 1981; 63: 1166–1172.
Rautaharju PM, Zhou SH, Park LP . Improved ECG models for left ventricular mass adjusted for body size, with specific algorithms for normal conduction, bundle branch blocks, and old myocardial infarction. J Electrocardiol 1996; 29(Suppl): 261–269.
Acknowledgements
This work was supported by grants from the Finnish Foundation for Cardiovascular Research and the Aarne Koskelo Foundation.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Oikarinen, L., Karvonen, M., Viitasalo, M. et al. Electrocardiographic assessment of left ventricular hypertrophy with time–voltage QRS and QRST-wave areas. J Hum Hypertens 18, 33–40 (2004). https://doi.org/10.1038/sj.jhh.1001631
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.jhh.1001631
