
Abstract
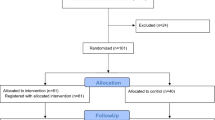
Lifestyle programmes delivered by academic nurse-counsellors in a primary care setting lowered blood pressure (BP) among at-risk patients. We examined whether the programmes could be successfully implemented by nurses employed in Australian general practices. In a randomised controlled trial, 212 of 591 eligible 20–75-year olds with hypertension, Type II diabetes or coronary disease from seven practices volunteered. Patients were randomised to: a ‘Low’ group with one face-to-face individual counselling session, then monthly telephone contacts for 1 year (n=69); a ‘High’ group with individual face-to-face counselling up to 1 h monthly for 1 year (n=74) or a control group receiving usual care only (n=69), and were evaluated at baseline and 12 and 18 months later; 164 individuals completed the study. Patients' usual doctors continued to prescribe in all groups. Changes in 24 h ambulatory BP did not differ significantly between groups at 12 months (Low, −2±2/1±1 mmHg; High, +4±2/1± 1 mmHg; usual care, +1±2/1±1 mmHg) or 18 months (−2±2/2±1 mmHg; −4±2/3±2 mmHg; −1±2/2± 1 mmHg, respectively). Antihypertensive drugs prescribed decreased by 12 months in 33% of the High, 5% of the Low and 13% of the control groups (P=0.008) and by 36, 7 and 16% at 18 months (P=0.018). After 18 months, targets for BP control were not met in about 60% of patients and almost 50% had clinic BP above 140/90 mmHg. Year-long interaction with nurse-counsellors may influence longer-term antihypertensive drug prescription, possibly by improving compliance. Suboptimal BP control suggests that continuing physician education on BP targets is needed.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 digital issues and online access to articles
$119.00 per year
only $9.92 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others

References
Beilin LJ, Puddey IB, Burke V . Lifestyle and hypertension. Am J Hypertens 1999; 12: 934–945.
Ebrahim S, Smith Davey G . Systematic review of randomised controlled trials of multiple risk factor interventions for preventing coronary heart disease. BMJ 1997; 314: 1666–1674.
Cupples ME, McKnight A . Randomised controlled trial of health promotion in general practice for patients at high cardiovascular risk. BMJ 1994; 309: 993–996.
Ebrahim S, Smith Davey G, Bennett R . Health promotion activity should be retargeted at secondary prevention. BMJ 2000; 320: 185.
Steptoe A et al. Behavioural counselling in general practice for the promotion of healthy behaviour among adults at increased risk of coronary heart disease: randomised trial. BMJ 1999; 319: 943–948.
Prochaska JO, DiClemente CC, Norcross JC . In search of how people change. Am Psychol 1992; 47: 1102–1114.
Woollard J et al. A controlled trial of nurse counselling on lifestyle change for hypertensives treated in general practice: preliminary results. Clin Exp Pharmacol Physiol 1995; 22: 466–468.
Woollard J et al. Effects of a general practice-based intervention on diet, body mass index and blood lipids in patients at cardiovascular risk. J Cardiovasc Risk 2003; 10: 31–40.
Wheeler C et al. Reproducibility of a meal-based food frequency questionnaire. The influence of format and time interval between questionnaires. Eur J Clin Nutr 1994; 48: 795–809.
Blair SN et al. Assessment of habitual physical activity by a seven day recall in a community survey and controlled experiments. Am J Epidemiol 1985; 122: 794–804.
Mori TA et al. Effects of varying fat, fish and fish oils on blood lipids in a randomized controlled trial in men at risk of heart disease. Am J Clin Nutr 1994; 59: 1060–1068.
Anonymous. WHO-International Society of Hypertension guidelines for the management of hypertension, guidelines subcommittee. J Hypertens 1999; 17: 151–183.
Aminoff UB, Kjellgren KI . The nurse — a resource in hypertension care. J Adv Nursing 2001; 35: 582–589.
Alderman MH, Madhavan S, Cohen H . Antihypertensive drug therapy: the effect of JNC criteria on prescribing patterns and patient status through the first year. Am J Hypertens 1996; 9: 413–418.
Flack JM, Novikov SV, Ferrarrio CM . Benefits of adherence to anti-hypertensive drug therapy. Eur Heart J 1996; 17 (Suppl A): 16–20.
Feldman R et al. Adherence to pharmacologic management of hypertension. Can J Public Health 1998; 89: 116–118.
Caro JJ et al. Persistence with treatment for hypertension in actual practice. Can Med Assoc J 1999; 160: 31–37.
Cohen JS . Adverse drug effects, compliance, and initial doses of antihypertensive drugs recommended by the Joint National Committee vs the Physicians' Desk Reference. Arch Intern Med 2001; 161: 880–885.
Mar J, Rodriguez-Artalejo F . Which is more important for the efficiency of hypertension treatment: hypertension stage, type of drug or therapeutic compliance? J Hypertens 2001; 19: 149–155.
Acknowledgements
This study was supported by Healthway.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Woollard, J., Burke, V. & Beilin, L. Effects of general practice-based nurse-counselling on ambulatory blood pressure and antihypertensive drug prescription in patients at increased risk of cardiovascular disease. J Hum Hypertens 17, 689–695 (2003). https://doi.org/10.1038/sj.jhh.1001593
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.jhh.1001593
Keywords
This article is cited by
-
Adherence to Antihypertensive Medications: Current Status and Future Directions
Current Cardiovascular Risk Reports (2014)
