« Prev Next »
Birth defects are the leading cause of infant mortality worldwide, and affected children who survive infancy often struggle with lifelong physical and mental disabilities. Congenital defects arise for a variety of reasons; some defects are genetic, others are caused by environmental factors, and still others involve a combination of genetics and environment. But can anything be done to limit the frequency and impact of birth defects? In some cases-especially those that involve inherited conditions-the answer is no. However, in other instances, factors such as favorable prenatal environment and early treatment can prevent or reduce the phenotypic effects of birth defects, including a variety of defects that have a genetic basis.
Prevention and Prenatal Environment
As previously mentioned, a significant percentage of birth defects are triggered either wholly or in part by environmental factors. The most critical of these factors are those that affect a woman's body before or during pregnancy, because the woman's body forms her child's basic prenatal environment. Thus, strategies aimed at improving this environment can help reduce the effects of some types of birth defects.
Increasing Folic Acid Intake
One example of a successful prevention effort aimed at modification of the prenatal environment was the fortification of the United States' food supply with a B vitamin called folic acid. In 1992, the U.S. Public Health Service recommended that all women of childbearing age consume 400 micrograms of this vitamin daily (Blom et al., 2006). Folic acid is the synthetic form of the vitamin folate, which is available in many foods and in high concentrations in leafy, green vegetables. Normally, around the twenty-eighth day after fertilization, the cells responsible for developing an embryo's nervous system fold to form the neural tube, which is the precursor to the brain and spinal cord (Figure 1). However, deficiencies in maternal folic acid levels are associated with neural tube defects in developing embryos (Smithells et al., 1976). Thus, when taken early in pregnancy, folic acid reduces the risk of birth defects of the brain and spinal cord (Blom et al., 2006; Smithells et al., 1981; Smithells et al., 1983; Laurence et al., 1981.
The intake of folic acid supplements has been shown to prevent approximately 50% to 75% of neural tube defect cases. Nonetheless, in spite of the connection between folic acid and birth defects, women often do not ingest adequate amounts of folic acid during their first 28 days of pregnancy; after all, many women are just learning they are pregnant by the time their embryo's neural tube is nearly completely closed. Thus, in 1998, in an attempt to combat this problem, the United States government made fortification of flour and other enriched grain products with folic acid compulsory. Since then, the frequency of neural tube defects among U.S. newborns has dropped by 19% (Blom et al., 2006).
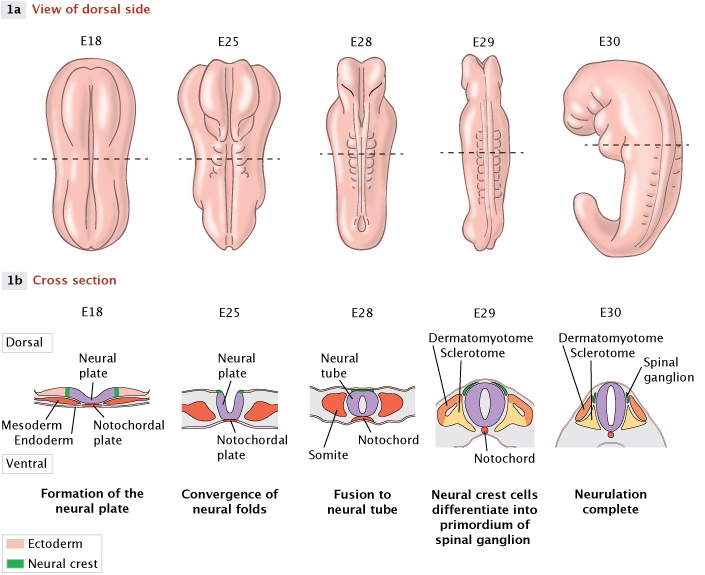
Figure 1: The major phases of neural tube closure
In the developing human embryo, there are major phases of neural tube closure that are common to all mammals. If the neural tube fails to close completely along its dorsal seam, this can result in spina bifida. Here, from left to right, the embryo is maturing, beginning with embryonic day 18 (E18). In row 1a, we see the embryo as a whole, from a dorsal viewpoint. In row 1b, we see a cross-section of underlying tissue along the horizontal dotted line shown in row 1a. Beginning near E18, tension brings the neural folds inward, in a process called bidirectional fusion. This process forms a depression in the neural plate called the neural groove, and the neural plate eventually fuses together on the dorsal side to make a hollow form called the neural tube (row 1b, purple). The hollow cavity eventually becomes the central canal of the mature spinal cord. This tube formation process sets the axial body plan along the spine, and determines the structure of the peripheral nervous system that grows out from it. As the tube first forms and closes, there are cells that derive from the neural plate but are not enclosed in the tube, and instead rest atop it; these are called neural crest cells (green), which eventually migrate to form a variety of peripheral body tissues. The neural tube is flanked by somites which eventually form the ribcage, bones, and muscle. On the ventral side of the neural tube is an important structure called the notochord that also helps define the longitudinal body axis during early development. Closure of the neural tube is normally complete by the E30.
© 2014 Nature Education All rights reserved. 
Reducing Sugar Intake
As the folic acid example illustrates, the right prenatal nutrient balance is a key environmental factor in the development of a healthy child. Although nutritional deficiencies can have devastating consequences, excess consumption of other substances, such as sugar, can also have a negative effect. For instance, gestational diabetes is a condition that can occur in pregnant women who have no prior history of diabetes. A pregnant woman can develop resistance to insulin because of hormonal changes related to the formation of the placenta (Buchanan & Xiang, 2005). Women can be screened for gestational diabetes, and the condition can generally be controlled by limiting sugar intake and exercising. Gestational diabetes can also pose risks for the infant, who might be born prematurely with a larger or smaller weight than average babies. These children can show growth abnormalities after birth and have a greater risk of obesity in childhood and adulthood (Boney et al., 2005; Whitaker et al., 1998). Premature infants also have a greater risk of respiratory difficulties because their lungs have not fully matured. Furthermore, mothers with gestational diabetes are at a greater risk of developing diabetes following pregnancy (Buchanan & Xiang, 2005).
Limiting Exposure to Teratogens and Mutagens
Although researchers have identified the majority of nutritional deficiencies that have a negative impact on prenatal environment, the true extent of the effect of nutrition remains an active area of research. Similarly, research also continues as to the precise effects of various teratogens and mutagens on fetal development.
A teratogen is any substance that is known to cause birth defects in humans; common examples include alcohol, cigarette smoke, certain medications, and numerous industrial chemicals. These substances promote birth defects by altering the actual environment within the womb. For instance, the elevated nicotine levels associated with smoking during pregnancy have been linked to an increased risk of stillbirth, low birth weight, and cleft lip and/or palate. Similarly, alcohol can be classified as a teratogen because use of this substance during pregnancy may result in fetal organ defects, abnormal facial features, and mental retardation, among other problems.
Just as exposure to teratogens during pregnancy can be devastating, so can maternal exposure to mutagens even before conception. Quite simply, a mutagen is any agent that alters the structure of a cell's genetic material. Thus, if a woman is exposed to a mutagen even before she becomes pregnant, and if this mutagen alters the DNA in one or more of her reproductive cells, the woman's eventual offspring could be negatively affected. Mutagens exist in a variety of forms, from chemical substances to ionizing radiation. A number of common teratogens, including cigarette smoke and alcohol, can also have mutagenic effects. Therefore, limiting exposure to mutagens and teratogens both before and during pregnancy is one major environmental factor that is within a woman's control.
Detection and Early Treatment of Birth Defects
Of course, many birth defects cannot be prevented; this is especially true of defects that have a genetic component. Thankfully, screening and treatment methods can be implemented to avoid the complications of birth defects and increase an affected child's possibilities of a better quality of life. For example, ultrasonography and maternal serum screening can be used to detect serious fetal anomalies, including neural tube defects and chromosomal disorders. In addition, after birth, infants can be screened for a variety of genetic, hematological, metabolic, and hormonal disorders to provide early diagnoses.
Early detection and treatment of birth defects can help prevent stillbirth or physical and intellectual disabilities. Consider the case of congenital hearing impairment, which can result from a number of environmental and/or genetic causes. Without early testing, a diagnosis of hearing loss might not occur until a child is two or three years old, resulting in delayed speech and language development. Another example is a condition called phenylketonuria, which is an inherited disorder characterized by the inability to synthesize the amino acid tyrosine from phenylalanine. Treatment of this condition involves a diet low in phenylalanine and high in tyrosine, and treatment results are best if this diet is implemented at birth.
Surgery can also be used to treat many birth defects, including cleft lip and palate and spina bifida, sometimes even before a child is born. The idea behind prenatal surgery is to limit long-term damage through early intervention. Prenatal heart and renal-tract defects are often treated surgically while the child is still in the womb, providing decompression and early correction for a better developmental prognosis. Finally, although gene therapy is also a possible option for treating certain genetic defects, it is not yet used on a wide scale.
Summary
Although many birth defects cannot be prevented, the probability of some such conditions can be reduced through awareness of the effects of various prenatal factors, including nutrients, teratogens, and mutagens. Furthermore, early detection and/or treatment of congenital defects can sometimes reduce the long-term impact of these conditions, perhaps even alleviating them completely. As researchers learn even more about the environmental and genetic factors that contribute to birth defects, it is likely that they will continue to reduce the prevalence of these conditions, thereby improving the quality of life for millions of people throughout the world.
References and Recommended Reading
Blom, H. J., et al. Neural tube defects and folate: Case far from closed. Nature Reviews Neuroscience 7, 724–731 (2006)
Boney, C. M., et al. Metabolic syndrome in childhood: Association with birth weight, maternal obesity, and gestational diabetes mellitus. Pediatrics 115, e290-296 (2005)
Buchanan, T.A., & Xiang, A.H. Gestational diabetes mellitus. Journal of Clinical Investigation 115, 485-491 (2005)
Christianson, A., Howson, C. P., & Modell, B. March of Dimes Global Report of Birth Defects: The Hidden Toll of Dying and Disabled Children. (2006) (accessed May 12, 2008).
Ericson, A., et al. Cigarette smoking as an etiologic factor in cleft lip and palate. American Journal of Obstetrics and Gynecology 135, 348–351 (1979)
Hanson, J. W., et al. Fetal alcohol syndrome. Experience with 41 patients. Journal of the American Medical Association 235, 1458–1460 (1976)
Laurence, K. M., et al. Double-blind randomized controlled trial of folate treatment before conception to prevent recurrence of neural-tube defects. British Medical Journal 282, 1509-1511 (1981)
Pearce, E. National trends in iodine nutrition: Is everyone getting enough? Thyroid 17, 823-827 (2007) (doi: 10.1089/thy.2007.0102)
Potter, J. D., et al. Iodization and thyroid status in relation to stillbirths and congenital anomalies. International Journal of Epidemiology 8, 137–144 (1979)
Smithells, R. W., et al. Vitamin deficiencies and neural tube defects. Archives of Disease in Childhood 51, 944-950 (1976)
———. Apparent prevention of neural tube defects by periconceptional vitamin supplementation. Archives of Disease in Childhood 56, 911–918 (1981)
———. Further experience of vitamin supplementation for prevention of neural tube defect recurrences. Lancet 1, 1027–1031 (1983)
Whitaker, R. C., et al. Gestational diabetes and the risk of offspring obesity. Pediatrics 101, e9 (1998)