
Abstract
Fabry disease is an important underlying disease in young cryptogenic stroke patients. However, little is known regarding the frequency of Fabry disease in the general stroke population, especially in elderly patients. A total of 588 stroke patients (61.7% men; average age 74.1±12.5 years) were enrolled in this prospective study. Blood samples were obtained to produce blood spots to determine α-galactosidase A (α-GalA) activity and for GLA gene analysis. One 65-year-old female patient had a known GLA gene mutation, c.2T>C (p.M1T), causing Fabry disease. Five male patients and two female patients had GLA c.196G>C (p.E66Q) variant, which is not associated with the full clinical manifestations of Fabry disease. The allele frequency of GLA c.196G>C was significantly higher in male patients with small-vessel occlusion (odds ratio 3.95, P=0.048) and non-cardioembolism (odds ratio 4.08, P=0.012) than that in the general Japanese population. Fabry disease is rare in the general Japanese stroke population. However, screening identified one elderly female patient with Fabry disease. GLA c.196G>C variant is a genetic risk factor for cerebral small-vessel occlusion and non-cardioembolism in Japanese males but not in females.
Similar content being viewed by others
Introduction
Fabry disease (MIM301500) is an X-linked lysosomal storage disorder caused by mutations in the GLA gene encoding the lysosomal enzyme, α-galactosidase A (α-Gal A; EC3.2.1.22).1 α-Gal A hydrolyses the terminal α-galactosyl moieties from glycolipids and glycoproteins, and therefore its deficiency results in progressive accumulation of globotriaosylceramide (GL-3) and related glycosphingolipids in the vascular endothelial lysosomes of the kidneys, heart, brain and skin. Fabry disease is classified into three major subtypes; that is, classic, late onset, and female Fabry disease. The classic phenotype develops in hemizygous males who have little or no detectable α-Gal A activity with childhood-onset of acroparesthesia, hypohidrosis and angiokeratoma. The occurrence of renal failure, cardiac disease and stroke with advancing age lead to a decline in activities of daily living and premature death. On the other hand, the late-onset phenotype develops in hemizygous males with substantial levels of residual α-Gal A activity.2, 3 Heterozygous females with GLA mutation were initially thought to be clinically unaffected. However, a large-scale study showed that 69.4% of such females have symptoms and signs of Fabry disease.4 As most patients with late-onset and female Fabry disease have adult onset and frequently lack a relevant family history, there is a concern that many Fabry patients may be underdiagnosed and classified as having other more common diseases. Indeed, considerable numbers of adult patients with Fabry disease were found through screening of high-risk populations, including those with chronic kidney disease, left ventricular hypertrophy/hypertrophic cardiomyopathy and young stroke.2, 3, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14 Recently, we analyzed the frequency of GLA mutations in male Japanese ischemic stroke patients and showed that GLA c.196G>C (p.E66Q) variant is a genetic risk factor for cerebral small-vessel occlusion in elderly Japanese men.15 In this previous study, the frequency of c.196G>C variant may have been underestimated as DNA sequencing was performed only in patients with reduced α-Gal A activity15 and individuals with this variant occasionally showed blood α-Gal A activity within the normal range. In addition, female and hemorrhagic stroke patients have yet to be analyzed. In the present study, we performed additional screening for GLA gene mutation in a new set of Japanese stroke patients, including female and hemorrhagic stroke patients, with screening for GLA c.196G>C variant in all patients.
Materials and methods
Patients
Six clinical neurology departments in Nagano prefecture, Japan participated in this prospective study. From May 2012 to March 2016, a total of 588 stroke patients (61.7% men; average age 74.1±12.5 years) were enrolled in this study (Table 1). The etiology of ischemic stroke was classified according to the Trial of Org 10172 in Acute Stroke Treatment criteria16 as large-artery atherosclerosis in 113 patients, cardioembolism in 88 and small-vessel occlusion (lacunar infarction) in 179. Eight patients showed ischemic stroke of other determined etiology: cervicocephalic arterial dissection (n=5), patent foramen ovale plus venous thrombosis of lower extremity (n=1), paraneoplastic coagulopathy (n=1), and sinus thrombosis (n=1). Ischemic stroke of undetermined etiology was present in 88 patients. Cerebral hemorrhage was present in 126 patients. Subtypes of stroke overlapped in 14 patients, as they had histories of multiple strokes with different subtypes. Patients who were unable to provide informed consent or who had already been diagnosed with Fabry disease were excluded from the study. After obtaining informed consent, demographic data, cerebrovascular risk factors, presence of signs and symptoms of Fabry disease and clinical and neuroimaging data were registered in a database using case report forms.
α-Gal A enzyme assay and GLA gene analysis
A blood sample was obtained for production of blood spots for measurement of α-Gal A activity. α-Gal A activity was determined using a fluorescent substrate as described previously.15, 17
If blood αGal A activity was decreased (<10 AgalU), the entire GLA gene was analyzed. For DNA analysis, total genomic DNA was extracted from the leukocytes of patients. All seven exons and the flanking intronic sequences of the GLA gene were amplified by PCR, and the amplification products were analyzed by direct sequencing. All patients were screened for GLA c.196G>C (p.E66Q) variant (rs104894833), as individuals with this variant occasionally showed blood αGal A activity within the normal range. Genotyping of rs104894833 was performed using the ABI TaqMan Allelic Discrimination Kit and the ABI7500 Sequence Detection System (Applied Biosystems, Carlsbad, CA, USA) in accordance with the manufacturer’s instructions. If GLA c.196G>C was detected, whole GLA gene was analyzed by PCR and direct sequencing as described above.
Statistical analysis
To analyze the impact of GLA c.196G>C variant on the onset of stroke, we compared allele frequencies of GLA c.196G>C variant in stroke patients with that in the general Japanese population; we utilized the data from newborn screening for Fabry disease15 as a control (general Japanese population). We also compared blood α-Gal A activity of patients with c.196G>C variant with that of patients without the variant. Statistical comparisons were performed using Fisher’s exact test for binary outcomes and Mann–Whitney U-test for continuous variables. In all analyses, P<0.05 was taken to indicate statistical significance.
Protocol approvals and patient consent
This study was approved by the Ethical Committee of Shinshu University School of Medicine and the ethics committees of each of the participating clinical neurology centers. Written informed consent was obtained from each patient prior to enrollment.
Results
α-Gal A enzyme assay and GLA gene analysis
The average blood α-Gal A activities of the male and female study populations were 25.0±8.8 and 25.5±11.0 AgalU, respectively (Figure 1). We performed whole GLA gene analysis in two female patients with low blood α-Gal A activity (<10 AgalU), and the results indicated c.2T>C (p.M1T) mutation in one patient. The other patient showed no mutations or polymorphisms. Screening for c.196G>C variant in the whole study population detected five male patients and two female patients with this variant (Table 2). Whole GLA gene analysis of the seven patients detected no mutations or polymorphisms in coding regions other than c.196G>C. One female patient (patient 7, Table 2) had a known polymorphism in the 5′ non-coding region (c.-10C>T) in addition to c.196G>C.

The distribution of α-Gal A activity in all of the patients included in this study. The y axis indicates α-Gal A activity (AgalU). The cutoff α-Gal A activity was 10 AgalU. α-Gal A activity of male patients with c.196G>C variant (13.1±2.6) was significantly lower than that in male patients without the variant (25.2±8.7, P=0.0005) (a). α-Gal A activity of female patients with c.196G>C variant was not significantly different from that of female patients without the variant (b).
Clinical data of the patient with Fabry disease identified through screening of stroke patients.
The patient was a 65-year-old Japanese woman (II-2, Figure 2a). Her father (I-1, Figure 2a) died of sepsis at age 31 and her mother (I-2, Figure 2a) died of myocardial infarction at age 60 years. Her 63-year-old brother (II-3, Figure 2a), 41-year-old daughter (III-1, Figure 2a) and 38-year-old son (III-2, Figure 2a) had no obvious relevant medical history. There was no family history of acroparesthesia, hypohidrosis, angiokeratoma, renal failure, cardiomyopathy or stroke.

Pedigree (a), brain magnetic resonance (MR) imaging (b), diffusion-weighted image (c), MR angiography, chest X-ray (d) and electrocardiographic (e) findings of the Fabry patient with GLA c.2T>C (p.M1T) mutation. A full color version of this figure is available at the Journal of Human Genetics journal online.
The patient (II-2, Figure 2a) had been well until age 59 years, when she developed cardiac failure and hypertension, which was treated with amlodipine, enalapril maleate and betaxolol hydrochloride. At age 65 years, she developed acute onset of left-sided weakness and was admitted to our hospital. Brain magnetic resonance imaging and magnetic resonance angiography showed an acute infarction in the right temporal lobe due to right middle cerebral artery occlusion (Figures 2b and c). Chest X-ray revealed enlarged cardiac shadow (Figure 2d) and electrocardiography showed atrial fibrillation, left ventricular hypertrophy and ST-T abnormality (Figure 2e). Echocardiography showed mild symmetrical thickening of the ventricular wall (diastolic thickness of the left ventricular posterior wall, 12 mm; diastolic thickness of the interventricular septum, 12 mm) and diastolic dysfunction (ratio of early mitral inflow velocity to mitral annular early diastolic velocity (E/e' ratio), 17.3), although cardiac systolic function was preserved (left ventricular ejection fraction, 57.8%; fractional shortening, 30.3%). Measurement of α-Gal A in the whole blood revealed markedly reduced activity of 5.5 AgalU (Figure 1b), and direct DNA sequencing of the GLA gene revealed a single base sequence change (c.2T>C) causing substitution of a methionine reside with threonine at codon 1 (p.M1T), the known mutation causing classic Fabry disease.18
Clinical characteristics of patients with GLA c.196G>C variant
The clinical characteristics of the seven patients with GLA c.196G>C variant are summarized in Table 2. Five patients were hemizygous males, and the others were heterozygous females. Patients were aged >70 years except for two males (44 and 59 years). In the male patients with c.196G>C variant, mean blood α-Gal A activity was 13.1±2.6 (ranged from 10.1 to 17.8), which was significantly lower than that in male patients without the variant (25.2±8.7, ranged from 10.4 to 61.6, P=0.0005, Figure 1a). On the other hand, α-Gal A activity of female patients with c.196G>C variant (31.7±10.3, ranged from 21.4 to 41.9) was not significantly different from that of female patients without the variant (25.5±11.0, ranged from 9.5 to 95.0, P=0.402, Figure 1b).
Four male patients (patients 2–5) had multiple small-vessel occlusions, which were accompanied by mild white matter lesions (leukoaraiosis). One patient (patient 2) with small-vessel occlusions had a history of symptomatic thalamic hemorrhage and the other two patients (patients 3 and 5) had asymptomatic multiple microbleeds detected by T2*-weighted magnetic resonance imaging. Two male patients (patients 1 and 4) had large-artery atherosclerosis, one female patient (patient 6) had cardioembolism and one female patient (patient 7) had small-vessel cerebral infarction. No patients with GLA c.196G>C variant showed characteristic symptoms of Fabry disease, except one elderly male patient who had chronic kidney disease (serum creatinine level, 2.0 mg dl−1).
Statistical analysis of allele frequencies of the GLA c.196G>C variant in Japanese stroke patients
Statistical analysis using the Fisher’s exact test indicated that the allele frequencies of the GLA c.196G>C variant in male patients with small-vessel occlusion (2.46%, odds ratio 3.94, P=0.048) and non-cardioembolism (2.54%, odds ratio 4.08, P=0.012) were significantly higher than that in the general Japanese population (0.64%, Table 3). On the other hand, the allele frequencies of the male patients with all stroke, all ischemic stroke, large-artery atherosclerosis, cardioembolism and hemorrhagic stroke were 1.37, 1.65, 2.67, 0 and 1.37%, respectively; these differences were not statistically significant (Table 3). These results were compatible with our previous study.15 In this study, we analyzed female stroke patients in addition to male patients. In contrast to male patients, the allele frequency of the GLA c.196G>C variant in female stroke patients was not increased even in those with small-vessel occlusion (0.88%, odds ratio 1.39, P=0.52) and non-cardioembolism (0.53%, odds ratio 0.83, P=1.00).
Discussion
Stroke is one of the most common and serious complications of Fabry disease. According to the natural history data from the Fabry Registry, the prevalences of stroke in Fabry disease were 6.9% in male patients and 4.3% in female patients.19 Importantly, stroke may occur before diagnosis of Fabry disease and in the absence of other clinical manifestations of the disease.19 In fact, a recent large-scale screen (The Stroke in Young Fabry Patients Study) identified previously undiagnosed Fabry disease patients in 0.5% (definite Fabry disease) to 0.9% (definite+probable Fabry disease) of young stroke patients.13 On the other hand, Fabry disease was considered to be very rare in elderly stroke patients.15, 20 The present study identified a 65-year-old female Fabry patient who developed cardiogenic cerebral embolism. This is the first elderly patient identified through screening for Fabry disease in a stroke population, suggesting that Fabry disease should be considered in the differential diagnosis of underlying disease of stroke even in elderly patients, particularly in patients with left ventricular hypertrophy and/or chronic kidney disease.
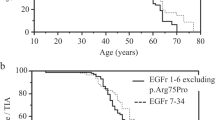
Another intriguing finding in the present study was the high prevalence of c.196G>C variant in male patients with small-vessel occlusion and non-cardioembolism. GLA c.196G>C is associated with relatively low α-GAL activity as compared with individuals without variants and had been considered as a pathogenic mutation, which induces late-onset Fabry disease associated with ventricular hypertrophy,8, 21, 22 renal failure2, 8, 22, 23 or cerebrovascular disease.24, 25 On the other hand, recent studies showed that c.196G>C is not a rare mutation but is found at certain frequencies in the general Korean26 and Japanese27 populations, suggesting that this variant is a functional polymorphism. In addition, pathological studies of biopsied renal,28 cardiac29 and skin tissues27 from male subjects with c.196G>C variant showed no abnormal accumulation of GL-3. At present, there is a consensus that c.196G>C variant is not associated with the full clinical manifestation of Fabry disease, but its pathogenesis remains controversial.15, 24, 25, 26, 27, 28, 29 Recently, Nakamura et al.15 reported that GLA c.196G>C variant is a genetic risk factor (allele frequency, 2.08; odds ratio=3.34) for cerebral small-vessel occlusion in elderly Japanese men. However, the frequency of c.196G>C in stroke patients may have been underestimated in the previous study as DNA sequencing was performed only in patients with reduced α-Gal A activity15 and individuals with this variant occasionally showed blood α-Gal A activity within the normal range. Therefore, we screened for GLA c.196G>C variant in all patients in this study and confirmed that the allele frequencies of GLA c.196G>C in male patients with cerebral small-vessel occlusion and non-cardioembolism were significantly higher than that in the general Japanese population (Table 3). In contrast to male stroke patients, the allele frequency of c.196G>C was not high in female patients with stroke even in cases of small-vessel occlusion or non-cardioembolism, suggesting that heterozygosity of this variant is not pathogenic. This appears to be reasonable considering the relatively mild impact of c.196G>C variant on onset of stroke in hemizygous male patients and the observation that blood α-Gal A activity was not decreased at all in heterozygous female patients (Figure 1b).
In Caucasian populations, the GLA c.937G>T (p.D313Y) variant is found with an allele frequency of 0.45%30 and showed relatively preserved α-Gal A activity11 similar to c.196G>C variant in the Japanese population. In the largest screen for Fabry disease in a young stroke population performed to date,13 patients with c.937G>T variant were regarded as ‘probable Fabry disease’, as patients harboring this variant showed significantly increased Gb3 and Gb3-C24 in addition to decreased α-Gal A activity. Similarly, Maruyama et al.31 reported that two of the nine patients with c.196G>C showed detectable levels of lyso-Gb3, a promising biomarker for Fabry disease. Taken together, these studies and the results of the present study suggest that GLA variants associated with relatively high residual α-Gal A activity may add to the risk of stroke, although they are not associated with full clinical presentation of Fabry disease with classical Mendelian effects.
Female Fabry patients may have been missed in the present study, as female patients could show normal α-Gal A activity. Therefore, plasma globotriaosylsphingosine (lyso-Gb3)31 in addition to α-Gal A activity should be analyzed in screening of female patients for Fabry disease in future studies. Our study was also limited by the relatively small sample size. Further large-scale epidemiological studies and biochemical and pathological examinations are necessary to elucidate the precise pathomechanism by which the c.196G>C variant increases the risk of stroke.
References
Desnick, R. J., Ioannou, Y. A., Eng, C. M. in The Metabolic and Molecular Bases of Inherited Disease, 8 edn (eds Scriver C. R., Beaudet A. L., Sly W. S. & Valle D.)37–74 McGraw-Hill, New York, USA, 2001).
Nakao, S., Kodama, C., Takenaka, T., Tanaka, A., Yasumoto, Y., Yoshida, A. et al. Fabry disease: Detection of undiagnosed hemodialysis patients and identification of a "renal variant" phenotype. Kidney Int. 64, 801–807 (2003).
Nakao, S., Takenaka, T., Maeda, M., Kodama, C., Tanaka, A., Tahara, M. et al. An atypical variant of Fabry's disease in men with left ventricular hypertrophy. N. Engl. J. Med. 333, 288–293 (1995).
Wilcox, W. R., Oliveira, J. P., Hopkin, R. J., Ortiz, A., Banikazemi, M., Feldt-Rasmussen, U. et al. Females with Fabry disease frequently have major organ involvement: lessons from the Fabry Registry. Mol. Genet. Metab. 93, 112–128 (2008).
Sachdev, B., Takenaka, T., Teraguchi, H., Tei, C., Lee, P., Mckenna, W. J. et al. Prevalence of Anderson-Fabry disease in male patients with late onset hypertrophic cardiomyopathy. Circulation 105, 1407–1411 (2002).
Monserrat, L., Gimeno-Blanes, J. R., Marin, F., Hermida-Prieto, M., Garcia-Honrubia, A., Perez, I. et al. Prevalence of fabry disease in a cohort of 508 unrelated patients with hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 50, 2399–2403 (2007).
Merta, M., Reiterova, J., Ledvinova, J., Poupetova, H., Dobrovolny, R., Rysava, R. et al. A nationwide blood spot screening study for Fabry disease in the Czech Republic haemodialysis patient population. Nephrol. Dial. Transplant. 22, 179–186 (2007).
Tanaka, M., Ohashi, T., Kobayashi, M., Eto, Y., Miyamura, N., Nishida, K. et al. Identification of Fabry's disease by the screening of alpha-galactosidase A activity in male and female hemodialysis patients. Clin. Nephrol. 64, 281–287 (2005).
Rolfs, A., Bottcher, T., Zschiesche, M., Morris, P., Winchester, B., Bauer, P. et al. Prevalence of Fabry disease in patients with cryptogenic stroke: a prospective study. Lancet 366, 1794–1796 (2005).
Wozniak, M. A., Kittner, S. J., Tuhrim, S., Cole, J. W., Stern, B., Dobbins, M. et al. Frequency of unrecognized Fabry disease among young European-American and African-American men with first ischemic stroke. Stroke 41, 78–81 (2010).
Baptista, M. V., Ferreira, S., Pinho, E. M. T., Carvalho, M., Cruz, V. T., Carmona, C. et al. Mutations of the GLA gene in young patients with stroke: the PORTYSTROKE study—screening genetic conditions in Portuguese young stroke patients. Stroke 41, 431–436 (2010).
Brouns, R., Thijs, V., Eyskens, F., Van Den Broeck, M., Belachew, S., Van Broeckhoven, C. et al. Belgian Fabry study: prevalence of Fabry disease in a cohort of 1000 young patients with cerebrovascular disease. Stroke 41, 863–868 (2010).
Rolfs, A., Fazekas, F., Grittner, U., Dichgans, M., Martus, P., Holzhausen, M. et al. Acute cerebrovascular disease in the young: the Stroke in Young Fabry Patients study. Stroke 44, 340–349 (2013).
Sarikaya, H., Yilmaz, M., Michael, N., Miserez, A. R., Steinmann, B. & Baumgartner, R. W. Zurich Fabry study-prevalence of Fabry disease in young patients with first cryptogenic ischaemic stroke or TIA. Eur. J. Neurol. 19, 1421–1426 (2012).
Nakamura, K., Sekijima, Y., Hattori, K., Nagamatsu, K., Shimizu, Y., Yazaki, M. et al. p.E66Q mutation in the GLA gene is associated with a high risk of cerebral small-vessel occlusion in elderly Japanese males. Eur. J. Neurol. 21, 49–56 (2014).
Adams, H. P. Jr, Bendixen, B. H., Kappelle, L. J., Biller, J., Love, B. B., Gordon, D. L. et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 24, 35–41 (1993).
Chamoles, N. A., Blanco, M. & Gaggioli, D. Fabry disease: enzymatic diagnosis in dried blood spots on filter paper. Clin. Chim. Acta 308, 195–196 (2001).
Eng, C. M., Ashley, G. A., Burgert, T. S., Enriquez, A. L., D'souza, M. & Desnick, R. J. Fabry disease: thirty-five mutations in the alpha-galactosidase A gene in patients with classic and variant phenotypes. Mol. Med. 3, 174–182 (1997).
Sims, K., Politei, J., Banikazemi, M. & Lee, P. Stroke in Fabry disease frequently occurs before diagnosis and in the absence of other clinical events: natural history data from the Fabry Registry. Stroke 40, 788–794 (2009).
Marquardt, L., Baker, R., Segal, H., Burgess, A. I., Poole, D., Hughes, D. A. et al. Fabry disease in unselected patients with TIA or stroke: population-based study. Eur. J. Neurol. 19, 1427–1432 (2012).
Yoshitama, T., Nakao, S., Takenaka, T., Teraguchi, H., Sasaki, T., Kodama, C. et al. Molecular genetic, biochemical, and clinical studies in three families with cardiac Fabry's disease. Am. J. Cardiol. 87, 71–75 (2001).
Shimotori, M., Maruyama, H., Nakamura, G., Suyama, T., Sakamoto, F., Itoh, M. et al. Novel mutations of the GLA gene in Japanese patients with Fabry disease and their functional characterization by active site specific chaperone. Hum. Mutat. 29, 331 (2008).
Fujii, H., Kono, K., Goto, S., Onishi, T., Kawai, H., Hirata, K. et al. Prevalence and cardiovascular features of Japanese hemodialysis patients with Fabry disease. Am. J. Nephrol. 30, 527–535 (2009).
Nakamura, K., Sekijima, Y., Nakamura, K., Hattori, K., Nagamatsu, K., Shimizu, Y. et al. Cerebral hemorrhage in Fabry's disease. J. Hum. Genet. 55, 259–261 (2010).
Tomizawa, Y., Okuzumi, A., Shiotsuki, H., Noda, K., Hattori, N. & Okuma, Y. A patient with the GLA p.E66Q mutation exhibiting vascular parkinsonism and bilateral pulvinar lesions. Intern. Med. 54, 2503–2506 (2015).
Lee, B. H., Heo, S. H., Kim, G. H., Park, J. Y., Kim, W. S., Kang, D. H. et al. Mutations of the GLA gene in Korean patients with Fabry disease and frequency of the E66Q allele as a functional variant in Korean newborns. J. Hum. Genet. 55, 512–517 (2010).
Togawa, T., Tsukimura, T., Kodama, T., Tanaka, T., Kawashima, I., Saito, S. et al. Fabry disease: biochemical, pathological and structural studies of the alpha-galactosidase A with E66Q amino acid substitution. Mol. Genet. Metab. 105, 615–620 (2012).
Satomura, A., Fujita, T., Nakayama, T., Kusano, H., Takayama, E., Hamada, H. et al. Pathological renal findings of chronic renal failure in a patient with the E66Q mutation in the alpha-galactosidase A gene. Intern. Med. 54, 1819–1824 (2015).
Kobayashi, M., Ohashi, T., Fukuda, T., Yanagisawa, T., Inomata, T., Nagaoka, T. et al. No accumulation of globotriaosylceramide in the heart of a patient with the E66Q mutation in the alpha-galactosidase A gene. Mol. Genet. Metab. 107, 711–715 (2012).
Yasuda, M., Shabbeer, J., Benson, S. D., Maire, I., Burnett, R. M. & Desnick, R. J. Fabry disease: characterization of alpha-galactosidase A double mutations and the D313Y plasma enzyme pseudodeficiency allele. Hum. Mutat. 22, 486–492 (2003).
Maruyama, H., Takata, T., Tsubata, Y., Tazawa, R., Goto, K., Tohyama, J. et al. Screening of male dialysis patients for fabry disease by plasma globotriaosylsphingosine. Clin. J. Am. Soc. Nephrol. 8, 629–636 (2013).
Acknowledgements
We thank Kana Fukushima and Yuki Akahane for their technical assistance. This study was supported in part by a Grant-in-Aid for Pediatric Research from the Ministry of Health, Labor and Welfare; a Grant-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science, and Technology; a Grant-in-Aid for Research on Rare and Intractable diseases, Health, and Labor Sciences; a Grant-in-Aid for Guidelines and lifetime medical support systems for inborn errors of metabolism found by newborn screening; and a Grant-in-Aid for the Practical Research Project for Rare/Intractable Diseases from Japan Agency for Medical Research and Development, AMED.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Nagamatsu, K., Sekijima, Y., Nakamura, K. et al. Prevalence of Fabry disease and GLA c.196G>C variant in Japanese stroke patients. J Hum Genet 62, 665–670 (2017). https://doi.org/10.1038/jhg.2017.31
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jhg.2017.31
This article is cited by
-
High-risk screening for Anderson–Fabry disease in patients with cardiac, renal, or neurological manifestations
Journal of Human Genetics (2019)
