
Abstract
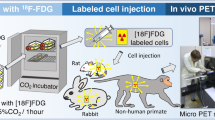
Assessing the retention of cell therapies following implantation is vital and often achieved by labelling cells with 2′-[18F]-fluoro-2′-deoxy-D-glucose (18F-FDG). However, this approach is limited by local retention of cell-effluxed radiotracer. Here, in a preclinical model of critical limb ischemia, we assessed a novel method of cell tracking using 3′-deoxy-3′-L-[18F]-fluorothymidine (18F-FLT); a clinically available radiotracer which we hypothesise will result in minimal local radiotracer reuptake and allow a more accurate estimation of cell retention. Human endothelial cells (HUVECs) were incubated with 18F-FDG or 18F-FLT and cell characteristics were evaluated. Dynamic positron emission tomography (PET) images were acquired post-injection of free 18F-FDG/18F-FLT or 18F-FDG/18F-FLT-labelled HUVECs, following the surgical induction of mouse hind-limb ischemia. In vitro, radiotracer incorporation and efflux was similar with no effect on cell viability, function or proliferation under optimised conditions (5 MBq/mL, 60 min). Injection of free radiotracer demonstrated a faster clearance of 18F-FLT from the injection site vs. 18F-FDG (p ≤ 0.001), indicating local cellular uptake. Using 18F-FLT-labelling, estimation of HUVEC retention within the engraftment site 4 hr post-administration was 24.5 ± 3.2%. PET cell tracking using 18F-FLT labelling is an improved approach vs. 18F-FDG as it is not susceptible to local host cell reuptake, resulting in a more accurate estimation of cell retention.
Similar content being viewed by others

Introduction
There is a rapidly growing interest in the use of cell-based therapies in the clinical management of cardiovascular disease. These developments require complementary imaging techniques to help assess the biodistribution and retention of cells in target tissues. It is important to understand cell retention in order to understand their mechanism of action, to develop techniques which help retain cells at the site of injury and to clarify optimal dosing regimens. There are different imaging modalities which can be employed in cardiovascular cell tracking studies1 including; magnetic resonance imaging2,3, optical4, ultrasound5, single-photon emission computed tomography (SPECT)6,7 and positron emission tomography (PET)8,9. With PET, cells can either be directly labelled, transplanted and tracked; or indirectly tracked post-transplantation using PET reporter genes10. However, due to regulatory hurdles the use of reporter genes in humans is limited.
One of the most commonly applied clinical PET cell tracking approaches in cardiovascular studies uses direct cell labelling with 2′-[18F]-fluoro-2′-deoxy-D-glucose (18F-FDG)8,9,11,12,13,14,15,16. 18F-FDG is a glucose analogue which becomes phosphorylated and trapped intracellularly and therefore can be used as a marker of metabolic activity as well as for cell tracking. However, there are two major limitations with this technique; first 18F-FDG can be effluxed from labelled cells and, second, this free radiotracer can then be taken up by local host cells making analysis of cell retention difficult. These limitations have led to efforts to reduce the efflux of 18F-FDG from labelled cells with limited success17. In addition, 18F-FDG is rapidly taken up by inflammatory cells and has been used as a marker of inflammation18,19,20 and, therefore, may not be suitable for PET cell tracking in cardiovascular diseases with an inflammatory component, such as myocardial infarction, atherosclerotic plaque development and limb ischemia. With the objective of developing an improved and readily translatable PET cell tracking imaging agent which has no (or negligible) transfer to non-target cells in vivo, we investigated a novel approach to direct cell labelling and tracking using the thymidine analogue 3′-deoxy-3′-L-[18F]-fluorothymidine (18F-FLT). Cellular uptake of 18F-FLT is limited to proliferating cells during DNA synthesis21. Therefore, efflux of 18F-FLT is unlikely to be scavenged and retained by non-dividing inflammatory cells which are locally present in this model, allowing more accurate interpretation of cell movement.
As part of our efforts to translate the use of human embryonic stem cell-derived endothelial cells into the clinic for treatment of critical limb ischemia22, we aimed to optimise and develop methods for the accurate assessment of cell tracking post-implantation. This investigation addressed the hypothesis that any 18F-FLT effluxed from labelled cells would not be incorporated at the site of injection by host cells, providing an improved method for tracking endothelial cell fate in an in vivo model of ischemia-induced angiogenesis compared to 18F-FDG labelling. The key aims were to determine; 1) whether cells could be labelled with 18F-FLT and how this compared to 18F-FDG labelling, 2) the effect of radiolabelling human umbilical vein endothelial cells (HUVECs) with 18F-FDG and 18F-FLT on cell viability, proliferation and function in vitro, and 3) if 18F-FLT cell labelling is an improved approach compared with 18F-FDG for assessing cell fate in vivo due to the absence of local re-uptake of effluxed radiotracer.
Results
Optimisation of cell radiolabelling with 18F-FDG or 18F-FLT and characterisation of in vitro radiotracer efflux
Incorporation of 18F-FDG into HUVECS (relative to supernatant) reached a plateau at 1.8 ± 0.1% following 90 min incubation with 5 MBq/mL in EGM-2 (Sup. Fig. 1a). When incubations were performed under starvation conditions (serum-free PBS), cellular uptake of 18F-FDG increased, with a plateau of 13.2 ± 1.3% reached following a 60 min incubation with 5 MBq/mL (Fig. 1a). A similar level of incorporation into HUVECs (12.7 ± 1.7%) was achieved with 18F-FLT following a 60 min incubation with 5 MBq/mL in EGM-2 (Fig. 1c). For both radiotracers, two PBS washes were sufficient to remove free agent from the supernatant (Sup. Fig. 1b,c).

(a) Optimisation of 18F-FDG labelling concentrations performed at different time-points under starvation conditions (PBS), expressed as % incorporation relative to incubation medium and washes, n = 3–4. Data presented as dose-response curves for three separate incubation time-points. (b) Leakage of intracellular 18F-FDG over time at room temperature, n = 3. (c) Optimisation of 18F-FLT labelling concentrations performed at different time-points under growth conditions (EGM-2), expressed as % incorporation relative to incubation medium and washes, n = 5. Data presented as dose-response curves for three separate incubation time-points. (d) Leakage of intracellular 18F-FLT over time at room temperature, n = 4–5.
To estimate the level of radiotracer leakage prior to administration, efflux from cells was investigated over the first hour post-labelling at room temperature. Efflux of 18F-FDG from cells stabilised at 13.9 ± 4.4% after 30 min (Fig. 1b). Likewise, efflux of 18F-FLT from the cells was stable at 17.8 ± 1.5% after 15 min (Fig. 1d).
Assessment of the effects of radiotracer labelling on HUVEC viability, proliferation and function
Radiolabelling cells with either 18F-FDG or 18F-FLT was not associated with any alteration of cell viability (Fig. 2a,b, respectively) at the investigated concentrations. However, 7 days post-radiolabelling, HUVECs incubated with 18F-FDG (10 MBq/mL) showed impaired proliferation (p = 0.0073) vs. vehicle treated cells. 18F-FDG labelling (10 MBq/mL) also caused an accumulation of cells within the ‘S’ phase of the cell cycle (p = 0.0089, Fig. 2c) vs. vehicle treated cells, which correlated with their proliferative capacity (p = 0.006). No such effect was observed with 18F-FLT labelling (Fig. 2d). Endothelial cell function, assessed by the cells’ ability to form 2D tubule networks on Matrigel, was not altered by 18F-FDG or 18F-FLT labelling (Fig. 3).

(a) Viability of 18F-FDG (n = 4–8) and (b) 18F-FLT (n = 6–7) labelled cells at 2 and 7 days post-labelling, assessed by trypan blue exclusion. The effect of (c) 18F-FDG (n = 3–6) and (d) 18F-FLT (n = 5–7) on cell proliferation 7 days post-labelling, assessed by total viable cell counts and FACs cell cycle analysis. **p ≤ 0.01 vs. control using a one-way ANOVA with post-hoc Dunnett’s test.

(a) 18F-FDG-treated HUVEC tubule formation on matrigel matrix 7 days post-labelling and (b) branch-point and network length quantification, n = 4–5. (c) 18F-FLT-treated HUVEC tubule formation and (d) branch-point and network length quantification, n = 5–7.
Dynamic PET imaging of free 18F-FDG and 18F-FLT distribution profiles
Following injection of free 18F-FDG or 18F-FLT in mice which had undergone the induction of hind-limb ischemia, the distribution of radiotracer was dynamically imaged (Fig. 4). At the first imaging time-point (16.7 ± 2.2 min post-injection, mean ± SD, n = 6), 29.8 ± 2.1% ID and 19.8 ± 4.3% ID of 18F-FDG and 18F-FLT signals, respectively, were still present within the injection site. In experiments performed with free 18F-FLT, remaining radiotracer cleared completely from the injection site. In contrast, experiments performed with free 18F-FDG demonstrated a significantly higher signal within the injection site at all time points vs. 18F-FLT. At the end of the study, 18F-FDG failed to clear from the injection site with 17.4 ± 2.7% ID remaining (Fig. 4c). In animals which received 18F-FDG, radioactivity accumulated at other highly metabolic sites, namely the myocardium and brain, as well as in the kidneys and urinary bladder which is consistent with 18F-FDG metabolic uptake and elimination (Fig. 4a, Sup. Fig. 2a). Following injection of 18F-FLT, no measurable PET signal was detected in any of the major organs apart from the kidneys and the urinary bladder, consistent with known excretion route of 18F-FLT (Fig. 4b, Sup. Fig. 2b).

Representative averaged (1 hr) images from each hour post-injection (P.I.) of (a) free 18F-FDG- and (b) free 18F-FLT. IS = injection site, M = myocardium and UB = urinary bladder. (c) Free 18F-FDG and 18F-FLT time activity curves at the injection site, *p < 0.05, **p ≤ 0.01, ***p ≤ 0.001 for 18F-FDG- vs. 18F-FLT, two-way ANOVA with post-hoc Bonferroni’s multiple comparisons test, n = 3.
Dynamic PET imaging of 18F-FDG and 18F-FLT-labelled HUVEC distribution profiles
In both cell labelling approaches, radioactivity in the engraftment site of mice which had undergone the induction of hind-limb ischemia reduced over the 4 hr acquisition (Fig. 5a,b). However, the rate of signal clearance with the 18F-FLT-HUVECs was faster compared with 18F-FDG-HUVECs (Fig. 5c). Similar to the free radiotracer experiment, 18F-FDG radioactivity accumulated in highly metabolic sites, namely the myocardium and brain, as well as in the kidneys and urinary bladder (Fig. 5a, Sup. Fig. 3a). Again, the 18F-FLT labelling approach did not result in uptake at any of the major organs apart from the kidneys and the urinary bladder (Fig. 5b, Sup. Fig. 3b). Neither approach resulted in accumulation of signal in the lungs, contralateral limb, liver or blood pool (Sup. Fig. 3).

Representative averaged (1 hr) images from each hour post-injection (P.I.) of (a) 18F-FDG- and (b) 18F-FLT-labelled HUVECs. IS = injection site, M = myocardium and UB = urinary bladder. (c) 18F-FDG- and 18F-FLT-labelled HUVECs time activity curves at the injection site and source organs, n = 3.
Estimation of cell retention at the engraftment site when using the 18F-FDG-labelling approach was hampered by local reuptake of effluxed radiotracer, as demonstrated in the free radiotracer experiments. Conversely, estimation of cell retention at the engraftment site when using the 18F-FLT-labelling approach was feasible; demonstrating that labelled cell retention decreased over time compared to the first time point (p ≤ 0.001 at 4 hr) (Fig. 6). At 4 hr post-transplantation, 24.5 ± 3.2% of cells remained within the engraftment site.

Retention was estimated relative to the inverse efflux rate of free radiotracer based on activity uptake at the source organs, *p < 0.05, **p ≤ 0.01, ***p ≤ 0.001 vs. first time-point, one-way ANOVA with post-hoc Dunnett’s test, n = 3.
Discussion
In this study, we explored the use of direct labelling of endothelial cells with 18F-FLT as an alternative to the commonly used 18F-FDG radiolabelling approach. To our knowledge, this is the first study to investigate 18F-FLT as a cell labelling agent. We hypothesised that, due to the nature of the 18F-FLT uptake mechanism, this approach would be suitable for labelling cells in culture. More importantly, we hypothesised that the 18F-FLT approach would not be confounded by local retention of radiotracer leakage from the transplanted cells in a murine model of critical limb ischemia; contrary to 18F-FDG which would be retained. We have demonstrated that both uptake and leakage of 18F-FLT by HUVECs was comparable to that of 18F-FDG. Also, 18F-FLT-labelling was not associated with any impact on cell characteristics; unlike 18F-FDG, which at high concentrations impaired the cells capacity to proliferate. In the murine model of hind-limb ischemia we demonstrated that free 18F-FLT is completely cleared from the injection site whereas a substantial proportion of 18F-FDG is retained. In 18F-FLT-labelled cell tracking experiments, estimation of cell retention was possible and revealed that one quarter of the cells were still present within the engraftment site 4 hours post-injection.
When comparing the level of 18F-FLT incorporation which was achieved in this study to other approaches, it is important to note that there are a number of factors which may affect cell uptake/yields, such as; incubation conditions, cell type, cell number, incubation volume and labelling agent uptake mechanism. Also, methods of reporting uptake/yield differ across studies making it difficult to directly compare. While uptake in this study (12%) may be considered to be at the lower end of what is reported in the literature, particularly compared to [89Zr]oxinate4 which has been reported to be in the range of 40–61%23, the levels which were achieved in this study were sufficient to accurately measure the signal within the engraftment site for up to 4 hours. In addition, studies previously performed with 111In-tropolone-labelling6,7 of endothelial cells have resulted in 0.1 Bq/cell, which is the same value achieved within this study. This allows for successful scaling up to clinical translation, where the total injected activity will be sufficient for in vivo imaging.
The negative impact of 18F-FDG on cell proliferative capacity is an important observation which highlights the need to assess the effect of labelling agents on cell properties prior to in vivo studies, an aspect which is often under-studied. Not surprisingly, we found that 18F-FDG-induced impairment of cell proliferation correlated with an accumulation of cells in the S phase of the cell cycle, indicative of radiation-induced DNA damage. The effect of 18F on DNA damage has been demonstrated previously24. Kashino et al. assessed the effect of poorly absorbed 18F ion versus highly absorbed 18F-FDG on double strand DNA breaks. Intracellular 18F in the form of FDG caused more double stranded breaks and lower cell proliferation in Chinese Hamster Ovary cells compared with 18F ion. Similarly, 18F-FDG labelling of adipose-derived stem cells also caused DNA damage and impaired proliferation25. In contrast, however, other studies using mesenchymal and embryonic stem cells have reported no such detrimental effects following labelling with 18F-FDG15,26. These conflicting reports may be due to differences in uptake levels which were achieved across the studies. Data from our study are consistent with prior observations that cellular damage by 18F radiolabelling is dependent on the radiotracer used as this influences the delivery of dose to key intracellular structures. The lack of detrimental effect evident on the total population of HUVECs post-18F-FLT may be due to this approach only labelling a subset of the cells which are undergoing S-phase of the cell cycle due to the uptake mechanism of this radiotracer21,27. The uptake mechanism of 18F-FDG28 is likely to result in greater homogeneity of individual cell uptake, making total population effects more obvious.
In order to accurately quantify cell tracking, an ideal cell-labelling agent should be specific for the transplanted cell with no or negligible transfer to non-target cells locally or systemically in vivo. This allows for an accurate estimation of cell engraftment and distribution29. Efflux of labelling agents from cells can interfere with this goal. In this study we demonstrated that prior to injection, around 14–18% of the labelling agent had leaked from the cells in vitro. This degree of leakage is similar to other reported values when using direct cell labelling methods25, albeit some studies have reported cell efflux values as high as 40–50% up to 2 hours post-labelling15,17. Differences in radiotracer leakage are likely due to different levels of incorporation which were achieved across studies and is also likely to be cell-type dependent. As a degree of labelling agent leakage from cells is unavoidable when using direct cell labelling methods, consideration of the specificity of the radiotracer uptake mechanism is paramount to best tailor in vivo cell tracking techniques to a given application, particularly in studies with a highly localised delivery site. In light of the well described uptake mechanisms of 18F-FDG and 18F-FLT21,28, we hypothesised that efflux of 18F-FDG would result in local retention unlike 18F-FLT which would be cleared. We were led to this hypothesis due to a number of factors. Activation and infiltration of inflammatory cells to the injury site is a major event during hind-limb ischemia30, and results in a local increase of highly metabolically-active cells. In other murine models of cardiovascular injury, acute recruitment of inflammatory cells to an injury site can occur in the first few hours of reperfusion (1–5 hr)31,32. Another source of local radiotracer retention may include increased metabolism during skeletal muscle ischemia33, as well as locally increased energy demand due to ischemia-induced switching of native endothelial cells from a quiescent to an angiogenic phenotype34,35.
In this current study, the leakage profiles measured were similar for both radiotracers. In addition, the finding that a significant proportion of 18F-FDG is retained within the ischemic hind-limb indicates that the signal measured in the injection site when using 18F-FDG labelling represents three different compartments. Specifically: 18F-FDG-labelled HUVECs, secondary cell labelling via transfer of 18F-FDG to local cells, and free 18F-FDG. Conversely, using the 18F-FLT approach, there are two major compartments: 18F-FLT-labelled cells and free 18F-FLT. A third potential minor compartment would include free or metabolised (in various cells) radiotracer, although this is unlikely based on the results collected during the free radiotracer experiments. Therefore, 18F-FLT-labelling of cells allows for more accurate assessment of cellular engraftment/kinetics within highly metabolic sites compared with 18F-FDG based approaches. This 18F-FLT-based cell tracking approach will also be particularly valuable in cell tracking studies within the heart (such as following myocardial infarction), given that free 18F-FLT is not taken up by cells in the myocardium. The fact that 18F-FDG is often used in studies of cardiac inflammation and injury further indicates that 18F-FDG is not optimal for these purposes19,36. Therefore, the novel 18F-FLT cell labelling approach presented here can be valuable in multiple clinical cardiovascular applications and potentially cell tracking in other biomedical applications.
Due to improved compartmental definition within the 18F-FLT signal of this study, an attempt has been made to estimate cell retention within the engraftment site. This interpretation is based on the inverse rate of free radiotracer accumulation relative to the total injected dose within source organs, which for 18F-FLT consisted of the elimination organs (kidney and bladder). It should be noted that this interpretation may be confounded by variability in urinary excretion that can affect uptake at the elimination organs. However, urinary voiding was not observed during these scanning sessions, and care was taken to ensure consistent animal preparation and surgical procedures across individual animals. Within this study, estimated cell retention at the engraftment site was 24.5 ± 3.2% at 4 hours post-injection, suggesting a rapid clearance of cells. This estimation follows the range of early retention rates reported in previous clinical studies37,38,39 using alternative cell tracking methods, with one study in particular reporting an average cell retention rate of 21.3 ± 5.2% at 2 hours post-injection following transendocardial delivery of bone marrow mononuclear cells40. Thus, despite cell retention post-injection being largely dependent on the administration route, type of cells and type of pathology; the rates reported in this study are in-line with previously reported values in other applications. In addition to cell retention, this study explored the potential fate of 18F-FLT-labelled cells which may have left the engraftment site by evaluating the signals within the liver and lungs. These organs demonstrated negligible levels of radioactivity, indicating negligible accumulation of cells within these structures. In contrast, the previously demonstrated fate of intravenously administered 18F-FDG-labelled mesenchymal stem cells demonstrated significant accumulation within these organs26. It is conceivable that the majority of the injected cells in this study have lost their cellular arrangement or died locally and released free radiotracer, which could explain the observed high uptake in the kidneys and urinary bladder. This is consistent with prior reports that only 1–5% of delivered cells engraft within the target site for regeneration41.
While the lower impact of 18F-FLT-labelling on the total population of HUVECs is certainly an advantage over 18F-FDG-labelling endothelial cells, labelling only a subpopulation of cells has some limitations. In studies which administer smaller cell doses, the lack of whole population labelling may limit the ability to detect small or diffuse cell populations. In addition, heterogeneous cell uptake could further complicate interpretation of the cell retention profile when using direct cell labelling methods. Cells which have taken up larger amounts of radioactivity could be at greater risk of damage, and this may affect their fate following transplantation (thus complicating interpretation of cell fate). However, in this particular short-term cell tracking study this effect is likely to be less prominent than in long-term tracking. Moreover, in this study we have demonstrated that radiolabelling of cells with 18F-FLT had no effect on cell viability, proliferation and function in vitro. It should be noted that the value of this novel approach, as with any other 18F-based stem cell labelling and tracking approach, lies on the early assessment of cell engraftment and biodistribution within the first few hours post-transplantation. For studies requiring longer term cell tracking other imaging approaches using PET tracers with longer lived radioisotopes such as 89Zr-Oxinate423 and 64Cu–PTSM42 are valuable alternatives, in addition to the widely used 111In-tropolone or 99mTc-HMPAO labelling for SPECT cell tracking6,7,43. Alternatively, magnetic resonance imaging of iron nanoparticle labelled cells has also been shown to be a suitable approach for longitudinal cell tracking2.
Conclusion
A novel methodology for labelling human endothelial cells using 18F-FLT was shown to result in efficient labelling of cells without affecting cell characteristics and, more importantly, without resulting in local retention of effluxed 18F-FLT from the labelled HUVECs. Consequently, cell labelling with 18F-FLT for in vivo tracking using PET is an improved technique to evaluate cell engraftment/kinetics at the delivery site. 18F-FLT direct cell labelling is a fully translatable method and could be used to assess cell engraftment during stem cell therapy in both preclinical and clinical studies.
Methods
Radiotracers
18F-FDG was prepared using standard FASTlab FDG cassettes (GE Healthcare, UK) or TRACERlab MX kits (ROTEM, Israel) and formulated in phosphate buffer solution. 18F-FLT was prepared using a standard FASTlab FLT Cassette (GE Healthcare, UK) and was formulated in 9% ethanol in water. Radiochemical purity was >99% for both 18F-FDG and 18F-FLT.
Cell Culture
In this study, HUVECs were chosen as a model endothelial cell line as they share many characteristics with other pro-angiogenic endothelial cell therapies44. Pooled donor primary HUVECs (C-12208, PromoCell, Germany) were cultured in endothelial growth medium 2 (EGM-2) (PromoCell, Germany) on 0.1% gelatine (Sigma, USA)-coated culture flasks/plates and, where stated, Dulbecco’s Phosphate-Buffered Saline (DPBS) (Lonza, Switzerland) or endothelial basal medium (EBM) (PromoCell, Germany). HUVECs were passaged when confluent using 0.05% trypsin/EDTA (Gibco, UK) and used between passages 2–8.
Cell Radiotracer Labelling Optimisation
HUVECs were seeded at 0.25 × 106 cells/well in a 6-well plate and left to adhere overnight. To yield maximal incorporation of radiotracer in cells, different incubation mediums were investigated based on known radiotracer uptake mechanisms21,28. As 18F-FDG is a glucose analogue, uptake was assessed both in the presence of full growth medium (EGM-2) and under starvation (serum free PBS) conditions. 18F-FLT uptake was assessed using full growth medium (EGM-2). Immediately prior to incubation, adhered cells were washed with DPBS, then 1 mL of the radiotracer solution/well (1.25–10 MBq/mL) was added. The cells were then returned to the incubator (37 °C, 5% CO2, 100% humidity) for 30, 60 or 90 min. At the end of the incubation each well was washed twice with 1 mL DPBS, with the incubation medium and washes collected separately for counting. The remaining cells were then lysed by the addition of 200 μL RIPA buffer and transferred to corresponding tubes. The activity of each sample was measured using an automatic gamma counter (Wizard 1470 Gamma Counter, Perkin Elmer), and intracellular uptake was calculated as a percentage of the total yield from incubation medium and washes. Optimised labelling conditions were used for in vivo imaging studies by linear “scaling-up” of volume, total activity and cell density (2 × 106 cells).
Cell Radiotracer Leakage
To assess in vitro cellular radiotracer leakage prior to injection, 0.25 × 106 radiolabelled cells were suspended in 60 μL of EBM and kept at room temperature for up to 1 hour. Cells were then re-spun (200 × g, 5 min) at selected time intervals. The supernatant was collected in a separate vial, after which the remaining pellet was lysed by the addition of 200 μL RIPA buffer (Sigma, USA). Radioactivity was then measured as described in the previous section.
Cell Viability and Proliferation
Following radiolabelling with 18F-FDG or 18F-FLT, cells were washed and returned to EGM-2. Two days post-radiolabelling, cell viability was assessed by trypan blue exclusion assay. HUVECs were trypsinised, spun and aliquoted before adding 10% trypan blue solution to a final concentration of 0.04% (Bio-Rad, USA). Using a hemocytometer, viable cells were identified and counted by the absence of blue dye uptake. HUVECs were then reseeded into a 6-well plate at 0.05 × 106 and cultured for a further 5 days in EGM-2 with one medium change. Cell viability was calculated again, and proliferation was calculated using the total number of viable cells. Results were normalised to a vehicle control (1 hr PBS for 18F-FDG experiments, 1 hr EGM-2 for 18F-FLT experiments) which was washed and returned to EGM-2 in parallel with radiolabelled groups.
FACs Cell Cycle Analysis
Cell cycle analysis was carried out seven days post-labelling using cells re-plated at 0.1 × 106 cells/well on day 2. Briefly, cells were collected and fixed in 70% ethanol at 4 °C for at least 1 hr. The fixed cells were then spun and re-suspended in 250 μL PBS containing 50 μg/mL Ribonuclease A and incubated for 1 hr at 37 °C. Lastly, 40 μg/mL of propidium iodide was added to each sample before analysis by flow cytometry. Results were compared to a vehicle control (1 hr PBS for 18F-FDG experiments, 1 hr EGM-2 for 18F-FLT experiments) which was washed and returned to EGM-2 in parallel with radiolabelled groups.
Tubule Formation Assay
Endothelial cell function was assessed seven days post-radiolabelling using a Matrigel (Corning, USA) tubule formation assay, as previously described45,46. Briefly, 1 × 104 cells were seeded onto Matrigel-coated 96 well plates (50 μL Matrigel/well) in EGM-2. After 6 hours at 37 °C (5% CO2, 100% humidity), capillary-like endothelial cell networks were examined by phase contrast microscopy (×5 lens). The angiogenesis analyser plugin for image J47 was used to quantify the capacity of the cells to form tubule networks. Results were compared to a vehicle control (1 hr PBS for 18F-FDG experiments, 1 hr EGM-2 for 18F-FLT experiments) which was washed and returned to EGM-2 in parallel with radiolabelled groups.
Murine Hind-Limb Ischemia Model and Free Radiotracer/Radiolabelled Cell Administration
Experimental procedures were approved by the local University of Edinburgh animal ethics committee, and were authorized by the Home Office under the Animals (Scientific Procedures) Act 1986. Male CD1-Foxn1nu mice aged between 12–18 weeks were used in this study. Anaesthesia was induced and maintained using isoflurane (1.5%, Oxygen 1 L/min) during the surgical procedure. The hind-limb ischemia was induced as described48. Briefly, the left femoral artery was ligated and cut proximal to the epigastric branch, and the saphenous artery was ligated distal to the popliteal branch. Post-surgery, mice received an intramuscular injection of free 18F-FDG or 18F-FLT (500–900 kBq), or 18F-FDG or 18F-FLT-labelled cells (100–800 kBq) into the ischemic limb. Free radiotracer (diluted in 15 μL EBM-2) or labelled HUVECs (1 × 106 diluted in 15 μL EBM-2) were injected into three sites (5 μL/site) along the projection of the adductor muscle. The wound was closed with interrupted sutures (4/0 silk) and the animal placed into the nanoPET/CT scanner. Anaesthesia was maintained throughout the imaging session using isoflurane (1.5%, 0.5:0.5 Oxygen/Nitrous Oxide, 1 L/min).
PET/CT Acquisition, Reconstruction and Image Analysis
All PET data were acquired using a nanoPET/CT scanner (Mediso, Hungary). Post administration of free 18F-FDG/FLT or radiolabelled cells, a 240 min whole-body emission scan was obtained using a 1:5 coincidence mode. Then, a CT scan was acquired (semi-circular full trajectory, maximum field of view, 480 projections, 35 kVp, 400 ms and 1:4 binning) for attenuation correction. PET data was reconstructed into 3 × 10, 3 × 30 and 2 × 60 min frames using Mediso’s iterative Tera-Tomo 3D reconstruction algorithm and the following settings: 4 iterations, 6 subsets, full detector model, normal regularisation, spike filter on, voxel size 0.6 mm and 400–600 keV energy window. PET data were corrected for randoms, scatter and attenuation.
Reconstructed scans were imported into PMOD 3.4 software (PMOD Technologies, Switzerland) and volumes of interest (VOIs) were drawn around organs of interest and sites displaying a higher radioactivity concentration than background. Source organs for 18F-FDG included the myocardium, brain, kidneys and bladder; and for 18F-FLT included the kidneys and bladder. Radioactivity in the blood was estimated using the blood pool in the left ventricular cavity. At each time point, the measured activity at different sites was expressed as the percent injected dose (%ID). The percentage cell retention within the engraftment site (IM) at each time-point was estimated relative to the inverse efflux rate of free radiotracer, based on activity uptake at the source organs (SO). This calculation assumes that the rate of clearance (free radiotracer and radiotracer released form lysed cells) can be estimated as total activity (100% injected dose) minus source organ activity.
Statistical Analysis
The following statistical analyses were carried out using GraphPad Prism V.6, as detailed in figure legends; two-way ANOVA with post-hoc Bonferroni’s multiple comparisons test, one-way ANOVA with post-hoc Dunnett’s test and correlation analysis. A two-sided p value of <0.05 was considered statistically significant. GraphPad prism was also used to generate all graphs, representative of the mean ± SEM.
Additional Information
How to cite this article: MacAskill, M. G. et al. PET Cell Tracking Using 18F-FLT is Not Limited by Local Reuptake of Free Radiotracer. Sci. Rep. 7, 44233; doi: 10.1038/srep44233 (2017).
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Azene, N., Fu, Y., Maurer, J. & Kraitchman, D. L. Tracking of stem cells in vivo for cardiovascular applications. J. Cardiovasc. Magn. Reson. 16, 7 (2014).
Richards, J. M. J. et al. In vivo mononuclear cell tracking using superparamagnetic particles of iron oxide: feasibility and safety in humans. Circ. Cardiovasc. Imaging 5, 509–17 (2012).
Li, X.-X. et al. In vivo MRI tracking of iron oxide nanoparticle-labeled human mesenchymal stem cells in limb ischemia. Int. J. Nanomedicine 8, 1063–73 (2013).
Huang, N. F. et al. Embryonic stem cell-derived endothelial cells engraft into the ischemic hindlimb and restore perfusion. Arterioscler. Thromb. Vasc. Biol. 30, 984–91 (2010).
Jaiswal, J. K. & Simon, S. M. Potentials and pitfalls of fluorescent quantum dots for biological imaging. Trends Cell Biol. 14, 497–504 (2004).
Sabondjian, E. et al. Hybrid SPECT/cardiac-gated first-pass perfusion CT: Locating transplanted cells relative to infarcted myocardial targets. Contrast Media Mol. Imaging 7, 76–84 (2012).
Mitchell, A. J. et al. Comparison of the myocardial clearance of endothelial progenitor cells injected early versus late into reperfused or sustained occlusion myocardial infarction. Int. J. Cardiovasc. Imaging 29, 497–504 (2013).
Doyle, B. et al. Dynamic tracking during intracoronary injection of 18F-FDG-labeled progenitor cell therapy for acute myocardial infarction. J. Nucl. Med. 48, 1708–1714 (2007).
Lang, C. et al. In-vivo comparison of the acute retention of stem cell derivatives and fibroblasts after intramyocardial transplantation in the mouse model. Eur. J. Nucl. Med. Mol. Imaging 41, 2325–36 (2014).
Yaghoubi, S. S. & Gambhir, S. S. PET imaging of herpes simplex virus type 1 thymidine kinase (HSV1-tk) or mutant HSV1-sr39tk reporter gene expression in mice and humans using [18F]FHBG. Nat. Protoc. 1, 3069–75 (2006).
Hofmann, M. et al. Monitoring of bone marrow cell homing into the infarcted human myocardium. Circulation 111, 2198–2202 (2005).
Terrovitis, J. et al. Noninvasive quantification and optimization of acute cell retention by in vivo positron emission tomography after intramyocardial cardiac-derived stem cell delivery. J. Am. Coll. Cardiol. 54, 1619–1626 (2009).
Faivre, L. et al. 18F-FDG labelling of hematopoietic stem cells: Dynamic study of bone marrow homing by PET-CT imaging and impact on cell functionality. Curr. Res. Transl. Med. 64, 141–148 (2016).
Mathiasen, A. B. & Kastrup, J. Non-invasive in-vivo imaging of stem cells after transplantation in cardiovascular tissue. Theranostics 3, 561–572 (2013).
Lang, C. et al. Positron emission tomography based in-vivo imaging of early phase stem cell retention after intramyocardial delivery in the mouse model. Eur. J. Nucl. Med. Mol. Imaging 40, 1730–1738 (2013).
Elhami, E. et al. Assessment of three techniques for delivering stem cells to the heart using PET and MR imaging. EJNMMI Res. 3, 72 (2013).
Stojanov, K. et al. [18F]FDG labeling of neural stem cells for in vivo cell tracking with positron emission tomography: Inhibition of tracer release by phloretin. Mol. Imaging 11, 1–12 (2012).
Rudd, J. H. F. Imaging Atherosclerotic Plaque Inflammation With [18F]-Fluorodeoxyglucose Positron Emission Tomography. Circulation 105, 2708–2711 (2002).
Thackeray, J. T., Bankstahl, J. P., Wang, Y., Wollert, K. C. & Bengel, F. M. Clinically relevant strategies for lowering cardiomyocyte glucose uptake for 18F-FDG imaging of myocardial inflammation in mice. Eur J Nucl Med Mol Imaging 42, 771–780 (2015).
Rudd, J. H. F. et al. Atherosclerosis inflammation imaging with 18F-FDG PET: carotid, iliac, and femoral uptake reproducibility, quantification methods, and recommendations. J. Nucl. Med. 49, 871–8 (2008).
McKinley, E. T. et al. Limits of [18F]-FLT PET as a Biomarker of Proliferation in Oncology. PLoS One 8, 1–9 (2013).
Kane, N. M. et al. Derivation of endothelial cells from human embryonic stem cells by directed differentiation: Analysis of microrna and angiogenesis in vitro and in vivo . Arterioscler. Thromb. Vasc. Biol. 30, 1389–1397 (2010).
Charoenphun, P. et al. [89Zr]Oxinate4 for long-term in vivo cell tracking by positron emission tomography. Eur. J. Nucl. Med. Mol. Imaging 42, 278–287 (2014).
Kashino, G., Hayashi, K., Douhara, K., Kobashigawa, S. & Mori, H. Comparison of the biological effects of 18F at different intracellular levels. Biochem. Biophys. Res. Commun. 454, 7–11 (2014).
Elhami, E. et al. Viability and proliferation potential of adipose-derived stem cells following labeling with a positron-emitting radiotracer. Eur. J. Nucl. Med. Mol. Imaging 38, 1323–1334 (2011).
Wolfs, E. et al. 18F-FDG labeling of mesenchymal stem cells and multipotent adult progenitor cells for PET imaging: effects on ultrastructure and differentiation capacity. J. Nucl. Med. 54, 447–54 (2013).
Rasey, J. S., Grierson, J. R., Wiens, L. W., Kolb, P. D. & Schwartz, J. L. Validation of FLT uptake as a measure of thymidine kinase-1 activity in A549 carcinoma cells. J. Nucl. Med. 43, 1210–1217 (2002).
James, M. L. & Gambhir, S. S. A Molecular Imaging Primer: Modalities, Imaging Agents, and Applications. Physiol. Rev. 92, 897–965 (2012).
Zhang, S. J. & Wu, J. C. Comparison of imaging techniques for tracking cardiac stem cell therapy. J. Nucl. Med. 48, 1916–9 (2007).
Egami, K., Murohara, T., Aoki, M. & Matsuishi, T. Ischemia-induced angiogenesis: role of inflammatory response mediated by P-selectin. J. Leukoc. Biol. 79, 971–976 (2006).
Frangogiannis, N. The inflammatory response in myocardial infarction. Cardiovasc. Res. 53, 31–47 (2002).
Birdsall, H. H. et al. Complement C5a, TGF-β1, and MCP-1, in Sequence, Induce Migration of Monocytes Into Ischemic Canine Myocardium Within the First One to Five Hours After Reperfusion. Circ. 95, 684–692 (1997).
Haljamäe, H. & Enger, E. Human skeletal muscle energy metabolism during and after complete tourniquet ischemia. Ann. Surg. 182, 9–14 (1975).
Vizán, P. et al. Characterization of the metabolic changes underlying growth factor angiogenic activation: Identification of new potential therapeutic targets. Carcinogenesis 30, 946–952 (2009).
Verdegem, D., Moens, S., Stapor, P. & Carmeliet, P. Endothelial cell metabolism: parallels and divergences with cancer cell metabolism. Cancer Metab. 2, 19 (2014).
Rischpler, C. et al. PET/MRI early after myocardial infarction: evaluation of viability with late gadolinium enhancement transmurality vs. 18F-FDG uptake. Eur. Hear. J. - Cardiovasc. Imaging 16, 661–669 (2015).
Schächinger, V. et al. Pilot trial on determinants of progenitor cell recruitment to the infarcted human myocardium. Circulation 118, 1425–1432 (2008).
Blocklet, D. et al. Myocardial homing of nonmobilized peripheral-blood CD34+ cells after intracoronary injection. Stem Cells 24, 333–336 (2006).
Silva, S. A. et al. Autologous bone-marrow mononuclear cell transplantation after acute myocardial infarction: comparison of two delivery techniques. Cell Transplant. 18, 343–352 (2009).
Vrtovec, B. et al. Comparison of transendocardial and intracoronary CD34+ cell transplantation in patients with nonischemic dilated cardiomyopathy. Circulation 128, 42–50 (2013).
Kurtz, A. Mesenchymal stem cell delivery routes and fate. Int. J. Stem Cells 1, 1–7 (2008).
Adonai, N. et al. Ex vivo cell labeling with 64Cu-pyruvaldehyde-bis(N4-methylthiosemicarbazone) for imaging cell trafficking in mice with positron-emission tomography. Proc. Natl. Acad. Sci. 99, 3030–3035 (2002).
Goussetis, E. et al. Intracoronary infusion of CD133+ and CD133−CD34+ selected autologous bone marrow progenitor cells in patients with chronic ischemic cardiomyopathy: cell isolation, adherence to the infarcted area, and body distribution. Stem Cells 24, 2279–83 (2006).
Cho, S.-W. et al. Improvement of postnatal neovascularization by human embryonic stem cell derived endothelial-like cell transplantation in a mouse model of hindlimb ischemia. Circulation 116, 2409–19 (2007).
Logie, J. J. et al. Glucocorticoid-mediated inhibition of angiogenic changes in human endothelial cells is not caused by reductions in cell proliferation or migration. PLoS One 5 (2010).
Tura, O. et al. Late outgrowth endothelial cells resemble mature endothelial cells and are not derived from bone marrow. Stem Cells 31, 338–48 (2013).
Carpentier, G., Martinelli, M., Courty, J. & Cascone, I. Angiogenesis Analyzer for ImageJ. 4th ImageJ User and Developer. Conference proceedings. Mondorf-les-Bains, Luxembourg. ISBN: 2–919941-18-6: 198–201 (2012).
Niiyama, H., Huang, N. F., Rollins, M. D. & Cooke, J. P. Murine model of hindlimb ischemia. J. Vis. Exp. 2–4, doi: 10.3791/1035 (2009).
Acknowledgements
This work was funded by the Medical Research Council (MR/K00719X/1), The University of Edinburgh British Heart Foundation Core (RE/13/3/30183), The University of Edinburgh British Heart Foundation Centre for Vascular Regeneration (RM/13/2/30158) and The University of Edinburgh School of Clinical Sciences Funding Challenge. DEN is funded by the British Heart Foundation (CH/09/002) and is the recipient of a Wellcome Trust Senior Investigator Award (WT103782AIA). AHB is funded by the British Heart Foundation Chair of Translational Cardiovascular Sciences. We would like to thank the radiochemistry team within the Edinburgh Clinical Research Imaging Centre, as well as Dr. Susan Champion, Dr. Sally Pimlott and their team at the Greater Glasgow and Clyde NHS PET Centre for their crucial work and efforts to supply the radiotracers used in this study.
Author information
Authors and Affiliations
Contributions
M.G.M., A.S.T., P.W.F.H. and D.E.N. contributed to study concept and design. M.G.M., A.S.T., J.W., C.L., P.W.F.H. conducted the experiments. M.G.M., A.S.T., J.C.M., A.H.B., D.E.N. and P.W.F.H. contributed to analysis or interpretation of data. All authors participated in the drafting of the article and have given full approval of this version to be submitted.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
MacAskill, M., Tavares, A., Wu, J. et al. PET Cell Tracking Using 18F-FLT is Not Limited by Local Reuptake of Free Radiotracer. Sci Rep 7, 44233 (2017). https://doi.org/10.1038/srep44233
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep44233
This article is cited by
-
Imaging cellular activity and proliferation in the aortic wall
Journal of Nuclear Cardiology (2021)
-
Simultaneous in vivo PET/MRI using fluorine-18 labeled Fe3O4@Al(OH)3 nanoparticles: comparison of nanoparticle and nanoparticle-labeled stem cell distribution
EJNMMI Research (2020)
-
In vivo 19F MR inflammation imaging after myocardial infarction in a large animal model at 3 T
Magnetic Resonance Materials in Physics, Biology and Medicine (2019)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
