
Abstract
Previous studies indicated that food consumption was associated with Helicobacter pylori infection, but no study has yet investigated the association between Helicobacter pylori infection and dietary patterns. The aim of this study was to evaluate the associations between Helicobacter pylori infection and dietary patterns in Tianjin, China. The final cross-sectional study population comprised 10407 participants. Dietary consumption of participants was assessed via food frequency questionnaire. Factor analysis was used to identify dietary patterns, and Helicobacter pylori infection status was diagnosis by H. pylori urease Immunogold Testing kit. Participants in the highest quartile of the high-carbohydrate/sweet pattern showed a multivariable-adjusted OR (95% CI) of 1.65 (1.27–2.17) for the prevalence of H. pylori infection compared with those in the lowest quartile. The multiple adjusted OR for scores of the extreme quartile of high-protein/cholesterol pattern was 0.75 (95% CI, 0.57–0.98). This study demonstrated that a diet rich in carbohydrates and sweets was positively associated with the prevalence of H. pylori infection; interestingly, a diet characterized by high intake of animal offal, animal blood, fish, seafood, and poultry was associated with a reduction of prevalence of H. pylori infection.
Similar content being viewed by others


Introduction
Helicobacter pylori (H. pylori) has been the subject of increased attention in the last 30 years1 and affects approximately 50–70% of the population worldwide2. The prevalence of H. pylori infection ranges from 41.5% to 72.3% and may vary with the population studied and with the geographic area in China3. H. pylori infection is an important cause of chronic active gastritis and is strongly associated with peptic ulcer disease and gastric cancer4 and classified as a Group 1 carcinogen by the World Health Organization (WHO) and International Agency for Research on Cancer (IARC)5. Moreover, H. pylori infection may be associated with an increased risk for pancreatic disease6, lymphoma7, and atherosclerosis8.
Previous studies examined the effects of different dietary components on risk of H. pylori infection. Some foods and components possess anti-H. pylori activity, such as bovine milk9, cranberry10, broccoli sprout11, fast food12, and virgin oil13. Most recently, a review demonstrated that a plenty of dietary components, including specific foods, food components, and food products, were associated with H. pylori infection14. A case-control study from Malaysia found that frequent consumption of tea (OR: 0.023, 95% CI: 0.01–0.07), frequent use of ‘budu’ or local anchovy sauce (OR: 0.09, 95% CI: 0.1–0.7), and frequent use of local foods ‘pegaga’ or centenella asiatica (OR: 0.25, 95% CI: 0.1–0.65) were inversely associated with H. pylori infection15. However, regular diets consist of complex combinations of foods and nutrients ingested together may act independently or may interact with one another. Therefore, examination of dietary patterns, which assess the effects of overall diet and determined by factor analysis can be proxy indicators of real food consumption and availability, providing a more realistic representation of everyday eating habits16. Previous studies demonstrated that dietary patterns were associated with prevalence of gastric cancer17,18. But no study has yet investigated the association between Helicobacter pylori infection and dietary patterns. Previous studies focused on the effect of single food item on H. pylori infection instead of the whole diets9,10,11. However, we cannot know how the regular diets in relation to the prevalence of H. pylori infections, even though we know the effects of all single food items on H. pylori infections because of the interactions between food items and nutrients. In contrast, studies on dietary patterns are meaningful in the area of health education, which means we could give dietary recommendations to participants based on overall dietary patterns instead of single dietary components for prevention and cure. To the best of our knowledge, no study has examined the association between dietary pattern and H. pylori infection. We thus designed a cross-sectional study to investigate associations between dietary pattern and H. pylori infection in an adult population.
Results
Characteristics of participants
A total of 10407 participants in Tianjin were included in this analysis. Characteristics of participants according to H. pylori infection status are shown in Table 1. Participants with H. pylori infection tended to be men (P < 0.0001), older (P < 0.0001), have higher BMI (P < 0.0001), higher physical activity (P = 0.01), higher salt intake (P < 0.0001), higher prevalence of metabolic syndrome (P < 0.001), and higher prevalence of type 2 diabetes (P = 0.03). Participants with H. pylori infection also trended to drink alcohol everyday (P < 0.01) and have lower education level (P < 0.0001).
Dietary patterns
After varimax rotation, factor analysis revealed three dietary patterns and the main factor loadings of each pattern (Table 2). The three dietary patterns accounted for 28.5% of the variance in total food intake. According to the contribution to the total variation, the three dietary patterns were: factor 1 was defined as high-carbohydrate/sweet pattern and characterized by high intake of candied fruits, cakes, and sugared beverages; factor 2, the balanced pattern, was typified by a balance intake of fruits, vegetables, and soya bean products; factor 3, identified as a high-protein/cholesterol pattern and included high intakes of animal offal, animal blood, fish, seafood, and poultry.
Dietary patterns and H. pylori infection
Associations between dietary patterns and the H. pylori infection status are shown in Table 3. The high-carbohydrate/sweet pattern was positively associated with the prevalence of H. pylori infection (P for trend < 0.001) after adjustment. Participants in the highest quartile of the high-carbohydrate/sweet pattern showed a multivariable-adjusted OR (95% CI) of 1.65 (1.27–2.17) for the prevalence of H. pylori infection compared with those in the lowest quartile. The high-protein/cholesterol pattern was associated with a lower prevalence of H. pylori infection (P for trend = 0.04) after adjustment. However, the association between high-protein/cholesterol pattern and H. pylori infection was not strong. The multiple adjusted OR for scores of the extreme quartile of high-protein/cholesterol pattern was 0.75 (95% CI, 0.57–0.98). However, the associations were not significant when adjusting for age, sex, and BMI, but only reached significance upon adjusting for a multitude of other, potential confounders. Thus, the results could be affected by these potential confounders. No significant association was observed between balanced pattern and H. pylori infection after adjustment.
The relations between major food group consumption and H. pylori infection are presented in Table 4. No significant association was observed between any food groups and H. pylori infection after adjustment.
Discussion
This is the first study to assess the associations between dietary patterns and H. pylori infection. Our results demonstrated that the high-carbohydrate/sweet pattern which characterized by high intake of candied fruits, cakes, and ice cream was positively associated with the prevalence of H. pylori infection.
Previous studies have reported the positive relationship between carbohydrates with H. pylori infection12. The mechanism that links carbohydrates to H. pylori infection is not clear. It has been shown that carbohydrates intake19 was associated with metabolic syndrome. Previous studies showed a low-carbohydrates diet was associated with a decreased risk of type 2 diabetes in Japanese women20. A large population study in Japan indicated that H. pylori infection was significantly associated with the presence of metabolic syndrome21. A case-control study shown that prevalence of H. pylori was significantly higher in those diagnosed with diabetes as compared to controls22. Accordingly, these results suggested that carbohydrate was linked to H. pylori infection. Moreover, we found that most food items of the high-carbohydrate/sweet pattern were raw food products, such as ice cream and fruits. A previous study demonstrated that some types of raw ready-to-eat food, such as fruit salad, maybe the sources of resistant and virulent strains of H. pylori23. The results suggested that raw food products may serve as one route of transmission of H. pylori, meaning that further research is needed to clarify the associations between cooking methods and H. pylori infection. The high-carbohydrate/sweet pattern in our study was also associated with high intake of alcohol. Our results agreed with previous studies, suggesting that heavy alcohol consumption is predictively associated with H. pylori infection24,25. One study proposed a hypothesis that acute and chronic alcohol consumption disrupts the gastric mucosal barrier and increases the mucosa’s permeability, resulting in chemical inflammation. Subsequently, macrophages and neutrophils release the cytokine interleukin-8 (IL-8), which combines with its receptor in the endotheliocyte, facilitating further development of the inflammation and up-regulate the expression of adhesion molecules such as inter-cellular adhesion molecule 1 and lymphocyte function-associated antigen-1. IL-8 may interact with HP0638, the outer inflammatory protein, augmenting the adherence capacity of H. pylori and increasing the colonization density25.
Our result showed that the high-protein/cholesterol pattern, which characterized by high intake of animal offal, animal blood, animal liver, fish, seafood, and poultry, was associated with a lower prevalence of H. pylori infection even though the association was not strong. The top food items of high-protein/cholesterol pattern are animal offal, animal blood, and animal liver which especially rich in selenium and vitamin A. The best-known function of selenium is to protect membranes from oxidative damage26. Plasma selenium levels were similar between H. pylori (+) gastritis and healthy controls, but in the gastric tissue selenium levels were significantly higher in H. pylori (+) gastritis in a previous study27. And there was significantly decrease in mucosal selenium levels in patients after successful H. pylori eradication therapy which means selenium accumulates in gastric when it is needed27. Moreover, vitamin D has emerged as a central regulator of host defense against infections28. A study indicated that the vitamin D3 decomposition product 1 (VDP1) exerts an antibacterial action against H. pylori but not against other bacteria. Treatment with VDP1 induced a collapse of cell membrane structures of H. pylori and ultimately lysed the bacterial cells29. Animal foods, especially animal offal, animal liver, fish, and seafood, are rich in vitamin D28. Therefore, high intake of these kinds of food may provide adequate vitamin D and decrease the prevalence of H. pylori infection. However, dietary patterns have more characteristics and are not sufficient to explain the associations between H. pylori infection and dietary patterns based on single nutrient intake, meaning that further studies are needed in this field. Moreover, previous studies demonstrated that a high intake of animal foods was associated with alcoholic fatty liver disease30, metabolic syndrome31, and diabetes32, suggesting it would not be always beneficial for health. Further studies should clarify the specific intake of such foods to effectively decrease the prevalence of H. pylori infection while also avoiding diseases caused by over intake.
We did not, however, observe the same associations between food items and H. pylori infection in our major food group analyses. It is because that foods and nutrients may act independently or may interact with one another, meaning that further research is needed to clarify the interactions of foods and nutrients in the relationship between dietary patterns and H. pylori infection.
We also found a negative association between higher level of education and H. pylori infection. This finding was in line with previous studies which showed that a lower education level was associated with a higher prevalence of H. pylori infection in adults33, pregnant women34, and children35. A study in Uganda34 suggested that education may influence personal and household hygiene practices which were associated with H. pylori infection. Unlike previous studies33,34, there was no association between household income and H. pylori infection in present study. It may be caused by the reason that most of the participants in our study were high-income and middle-income earners. A previous study demonstrated that the difference of H. pylori infection was significant only between participants with high-income and those with low-income35. According to the exchange rate in Dec. 5, 2015, one dollar is approximately equal to 6.4 Yuan. The average household income was about 1000 USD per month in Tianjin while most of our participants have a household income more than 1000 USD.
A few limitations are notable. First, because of the cross-sectional design of our study, we cannot assess the causal relationships between dietary patterns and the risk of H. pylori infection. For example, maybe individuals with greater health-care seeking behavior are more likely to have their H. pylori diagnosed, and thus change their dietary patterns. Second, because of the nature of the self-reporting questionnaire, recall bias exists, and the food intake may not be exact. Third, H. pylori infection status was evaluated solely with an H. pylori-specific IgG antibody without other confirmed assessments such as a urease breath test or a rapid urease test. The diagnosis of H. pylori infection may be not exact. Moreover, participants in this study are inhabitants in Tianjin (one of the big and developed cities in China) and most of them have higher socioeconomic status (education level and household income) than general Chinese populations. The high level of socioeconomic status could be a reason for the low prevalence of H. pylori infection in the present study. Thus, the presence of H. pylori infection is not completely in accordance with current H. pylori infection rates in China which are reaching 40–60% in adults36. Further research is needed to clarify the results in the present study. However, nearly all occupations are covered in this study, and we also included retired individuals living in residential communities. Thus, the sample population used here is representative of the general adult population in Tianjin. Despite these limitations, this is the first study to reveal the relationships between dietary patterns and H. pylori infection.
Materials and Methods
Participants
This cross-sectional study was based on the Tianjin Chronic Low-grade Systemic Inflammation and Health (TCLSIH) Cohort Study, which is a large prospective dynamic cohort study focusing on the relationships between chronic low-grade systemic inflammation and the health status of a population living in Tianjin, China37,38. General participants were recruited, while having their annual health examinations but not curing any disease at the Tianjin Medical University General Hospital-Health Management Center, the largest and most comprehensive physical examination center in Tianjin.
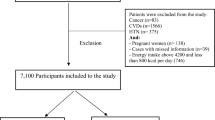
During the research period, there were 12096 participants with no history of H. pylori eradication therapy and gastrointestinal symptoms completed a comprehensive health examination and a study questionnaire reporting their personal information, dietary intake, lifestyles and health condition. We excluded participants who did not complete data collection (n = 633). Additionally, we excluded participants who had a history of cardiovascular disease (n = 828) or cancer (n = 228) because we considered cardiovascular disease and cancer could affect lifestyles of participants seriously. The final cross-sectional study population comprised 10407 participants for analyses. This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the medical ethics committee of Institutional Review Board of the Tianjin Medical University with the reference number of ‘TMUhMEC 201430’. Written informed consent was obtained from all subjects. The methods of this study were carried out in accordance with the approved guidelines.
Identification of dietary patterns
Dietary intake in last month was assessed using a modified version of the food frequency questionnaire (FFQ) that included 100 food items (the initial version of the FFQ included 81 food items30) with specified serving sizes. The FFQ included 7 frequency categories ranging from ‘almost never eat’ to ‘twice or more per day’ for foods and 8 frequency categories ranging from ‘almost never drink’ to ‘four or more times per day’ for beverages. The mean daily intake of nutrients was calculated by using an ad hoc computer program developed to analyze the questionnaire. The Chinese food composition tables39 were used as the nutrient database. The reproducibility and validity of the questionnaire were assessed in a random sample of 150 participants and living in Tianjin by comparing the data from the questionnaire with the data from 2 dietary questionnaires collected approximately 3 months apart and 4-day weighed dietary records (WDRs). Spearman rank correlation coefficient for energy intake between 2 food frequency questionnaires administered 3 months apart was 0.68. Correlation coefficients for food items (fruits, vegetables, fish, meat, and beverages) between 2 food frequency questionnaires administered 3 months apart ranged from 0.62 to 0.79 Spearman’s rank correlation coefficient for energy intake by the WDRs and the FFQ was 0.49. Correlation coefficients for nutrients (vitamin C, vitamin E, polyunsaturated fats, saturated fats, carbohydrate and calcium) by the WDRs and the FFQ ranged from 0.35 to 0.54. We applied factor analysis in order to generate major dietary patterns and factor loadings on all 100 food items. Varimax rotation40 was applied for greater interpretability. After evaluation of eigenvalues (greater than 1.0) and the scree test, 3 factors were determined. Food items with a factor loading greater than |0.30| were the main contributors to dietary pattern and representative of the character of each pattern. Factors were named descriptively according to the food items showing high loading (absolute value) with respect to each dietary pattern as follows: ‘high-carbohydrate/sweet’ pattern, ‘balanced’ pattern and ‘high-protein/cholesterol’ pattern.
Diagnosis of H. pylori infection
Blood samples of participants were used for serology, detecting anti-H. pylori antibodies (IgG) by enzyme-linked immunosorbent assay (ELISA). The H. pylori urease Immunogold Testing kit was from Beijing Tian Hong Sig biotechnology Co., Ltd. The sensitivity, specificity, and agreement were 98.91%, 98.29%, and 98.51%, respectively and similar to a former study used ELISA to detecting anti-H. pylori antibodies (IgG), which reported sensitivity and specificity as 95% and 82%41.
Assessment of other variables
Previous studies demonstrated that H. pylori infection was associated with socio-demographic conditions, such as age, sex, education, household income, and number of household34,35. Therefore, age, sex, education, household income, and living alone status were adjusted. Health status could also change one’s dietary habit and thus affect the associations between H. pylori infection and diet. Thus physical activity, metabolic syndrome, type 2 diabetes, and family history of diseases were adjusted. Furthermore, we additionally adjusted for other relevant variables such as smoking status, drinking status, and salt intake.
Anthropometric parameters (height, weight and waist circumference) were recorded using a standard protocol. Blood samples for the analysis of fasting blood glucose (FBG) and lipids were collected in siliconized vacuum plastic tubes. Fasting blood glucose (FBG) was measured by the glucose oxidase method, serum triglycerides (TG) were measured by enzymatic methods, and high-density lipoprotein cholesterol (HDL) was measured by the chemical precipitation method using reagents from Roche Diagnostics on an automatic biochemistry analyzer (Roche Cobas 8000 modular analyzer, Mannheim, Germany). Waist circumference was measured at the umbilical level with participants standing and breathing normally. Metabolic syndrome was defined in accordance with the criteria of the American Heart Association scientific statements of 200942. Diabetes was defined in the latest recommendations from American Diabetes Association43. BMI was calculated as weight/height2 (Kg/m2). A detailed personal and family history of physical illness and current medications were noted from ‘yes’ or ‘no’ responses to relevant questions in a self-reported questionnaire. Physical activity (PA) in the most recent week was assessed using the short form of the International Physical Activity Questionnaire (IPAQ)44. For socioeconomic characteristics, educational level was measured by asking the question ‘what is the highest degree you earned?’ and was divided into 2 categories: <College graduate or ≥College graduate. Household income was measured by asking the question ‘What’s your family’s income a month’ and was divided into 2 categories: <10000 Yuan or ≥10000 Yuan. The subjects were also classified as living alone or living with others.
Statistical analysis
All analysis were performed using the Statistical Analysis System 9.3 edition for Windows (SAS Institute Inc., Cary, NC, USA), and a P-value of 0.05 was considered to be statistically significant. Descriptive data are presented as the geometric mean (95% CI) for age, BMI, physical activity, salt intake and energy intake as these variables are not subject to normal distribution, and as percentages for categorical variables.
In order to characteristics of participants according to H. pylori infection status, continuous variables were examined using analysis of variance and chi-square test for categorical variables. Quartiles were categorized across the scores of each dietary pattern based on the distribution of the scores for all the participants and used for further analysis. Relationship between quartilecategories of dietary pattern scores and H. pylori infection status were examined using logistic regression by three different models. Odds ratios (OR) and 95% Confidence interval (CI) were calculated. Model 1 was used to calculate the crude OR, and model 2 was adjusted for age, sex, and BMI. Model 3 additionally adjusted for age, sex, BMI, smoking status, drinking status, physical activity, total energy intake, metabolic syndrome, type 2 diabetes, household incomes, educational levels, living alone, salt intake, and family history of diseases (cardiovascular, hypertension, hyperlipidemia, and diabetes). The variables which are not subject to normal distribution have been log-transformed before been included in the model. A linear trend cross increasing quartiles was tested using the median value of each quartile as a continuous variable based on linear regression. Model 3 was adjusted for analyses of major individual food groups: animal foods, fruits, vegetables, sugared beverages and snacks, and refined grain and grain products.
Transparency Declaration
The lead author affirms that this manuscript is an honest, accurate, and transparent account of the study being reported, that no important aspects of the study have been omitted and that any discrepancies from the study as planned have been explained. The reporting of this work is compliant with the “strengthening the reporting of observational studies in epidemiology” statement.
Additional Information
How to cite this article: Xia, Y. et al. Dietary Patterns are Associated with Helicobacter Pylori Infection in Chinese Adults: A Cross-Sectional Study. Sci. Rep. 6, 32334; doi: 10.1038/srep32334 (2016).
References
Montecucco, C. & Rappuoli, R. Living dangerously: how Helicobacter pylori survives in the human stomach. Nat Rev Mol Cell Biol 2, 457–466 (2001).
Calvet, X., Ramirez Lazaro, M. J., Lehours, P. & Megraud, F. Diagnosis and epidemiology of Helicobacter pylori infection. Helicobacter 18 Suppl 1, 5–11 (2013).
Xie, C. & Lu, N. H. Review: clinical management of Helicobacter pylori infection in China. Helicobacter 20, 1–10 (2015).
Lambert, J. R., Lin, S. K. & Aranda-Michel, J. Helicobacter pylori. Scand J Gastroenterol Suppl 208, 33–46 (1995).
Schistosomes, liver flukes and Helicobacter pylori. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Lyon, 7–14 June 1994. IARC Monogr Eval Carcinog Risks Hum 61, 1–241 (1994).
Bulajic, M., Panic, N. & Lohr, J. M. Helicobacter pylori and pancreatic diseases. World J Gastrointest Pathophysiol 5, 380–383 (2014).
Parsonnet, J. et al. Helicobacter pylori infection and gastric lymphoma. N Engl J Med 330, 1267–1271 (1994).
Vijayvergiya, R. & Vadivelu, R. Role of Helicobacter pylori infection in pathogenesis of atherosclerosis. World J Cardiol 7, 134–143 (2015).
Okuda, M. et al. Bovine lactoferrin is effective to suppress Helicobacter pylori colonization in the human stomach: a randomized, double-blind, placebo-controlled study. J Infect Chemother 11, 265–269 (2005).
Gotteland, M. et al. Modulation of Helicobacter pylori colonization with cranberry juice and Lactobacillus johnsonii La1 in children. Nutrition 24, 421–426 (2008).
Yanaka, A. et al. Dietary sulforaphane-rich broccoli sprouts reduce colonization and attenuate gastritis in Helicobacter pylori-infected mice and humans. Cancer Prev Res (Phila) 2, 353–360 (2009).
Mard, S. A., Khadem Haghighian, H., Sebghatulahi, V. & Ahmadi, B. Dietary Factors in Relation to Helicobacter pylori Infection. Gastroenterol Res Pract 2014, 826910 (2014).
Castro, M. et al. Assessment of Helicobacter pylori eradication by virgin olive oil. Helicobacter 17, 305–311 (2012).
Fahey, J. W., Stephenson, K. K. & Wallace, A. J. Dietary amelioration of Helicobacter infection. Nutr Res 35, 461–473 (2015).
Lee, Y. Y. et al. Sociocultural and dietary practices among Malay subjects in the north-eastern region of Peninsular Malaysia: a region of low prevalence of Helicobacter pylori infection. Helicobacter 17, 54–61 (2012).
Hu, F. B. Dietary pattern analysis: a new direction in nutritional epidemiology. Curr Opin Lipidol 13, 3–9 (2002).
Denova-Gutierrez, E., Hernandez-Ramirez, R. U. & Lopez-Carrillo, L. Dietary patterns and gastric cancer risk in Mexico. Nutr Cancer 66, 369–376 (2014).
Laroiya, I., Pankaja, S. S., Mittal, S. & Kate, V. A study of Helicobacter pylori infection, dietary pattern and habits in patients with gastric cancer in South India. Asian Pacific Journal of Tropical Disease 2, 24–26 (2012).
Sahyoun, N. R., Jacques, P. F., Zhang, X. L., Juan, W. & McKeown, N. M. Whole-grain intake is inversely associated with the metabolic syndrome and mortality in older adults. Am J Clin Nutr 83, 124–131 (2006).
Nanri, A. et al. Low-carbohydrate diet and type 2 diabetes risk in Japanese men and women: the Japan Public Health Center-Based Prospective Study. PLoS One 10, e0118377 (2015).
Gunji, T. et al. Helicobacter pylori infection is significantly associated with metabolic syndrome in the Japanese population. Am J Gastroenterol 103, 3005–3010 (2008).
Bajaj, S. et al. Association of helicobacter pylori infection with type 2 diabetes. Indian J Endocrinol Metab 18, 694–699 (2014).
Hemmatinezhad, B., Momtaz, H. & Rahimi, E. VacA, cagA, iceA and oipA genotypes status and antimicrobial resistance properties of Helicobacter pylori isolated from various types of ready to eat foods. Ann Clin Microbiol Antimicrob 15, 2 (2016).
Sanchez-Cuen, J. A., Cabrales, A. B., Magana, G. B. & Garay, F. J. [Helicobacter pylori infection and its association with alcohol consumption: a case-control study]. Rev Gastroenterol Mex 78, 144–150 (2013).
Zhang, L. et al. Relationship between alcohol consumption and active Helicobacter pylori infection. Alcohol Alcohol 45, 89–94 (2010).
Akcam, M. Helicobacter pylori and micronutrients. Indian Pediatr 47, 119–126 (2010).
Ustundag, Y., Boyacioglu, S., Haberal, A., Demirhan, B. & Bilezikci, B. Plasma and gastric tissue selenium levels in patients with Helicobacter pylori infection. J Clin Gastroenterol 32, 405–408 (2001).
Kroner, J. C., Sommer, A. & Fabri, M. Vitamin D Every Day to Keep the Infection Away? Nutrients 7, 4170–4188 (2015).
Hosoda, K. et al. Identification and characterization of a vitamin D(3) decomposition product bactericidal against Helicobacter pylori. Sci Rep 5, 8860 (2015).
Jia, Q. et al. Dietary patterns are associated with prevalence of fatty liver disease in adults. Eur J Clin Nutr (2015).
Lutsey, P. L., Steffen, L. M. & Stevens, J. Dietary intake and the development of the metabolic syndrome: the Atherosclerosis Risk in Communities study. Circulation 117, 754–761 (2008).
Feinman, R. D. Red meat and type 2 diabetes mellitus. JAMA Intern Med 174, 646 (2014).
Zaterka, S., Eisig, J. N., Chinzon, D. & Rothstein, W. Factors related to Helicobacter pylori prevalence in an adult population in Brazil. Helicobacter 12, 82–88 (2007).
Baingana, R. K., Kiboko Enyaru, J. & Davidsson, L. Helicobacter pylori infection in pregnant women in four districts of Uganda: role of geographic location, education and water sources. BMC Public Health 14, 915 (2014).
Nouraie, M. et al. Childhood hygienic practice and family education status determine the prevalence of Helicobacter pylori infection in Iran. Helicobacter 14, 40–46 (2009).
Chinese Society of Gastroenterology, C. S. G. o. H. p. et al. Fourth Chinese National Consensus Report on the management of Helicobacter pylori infection. J Dig Dis 14, 211–221 (2013).
Song, K. et al. Serum immunoglobulin M concentration is positively related to metabolic syndrome in an adult population: Tianjin Chronic Low-Grade Systemic Inflammation and Health (TCLSIH) Cohort Study. PLoS One 9, e88701 (2014).
Sun, S. et al. Subnormal peripheral blood leukocyte counts are related to the lowest prevalence and incidence of metabolic syndrome: Tianjin chronic low-grade systemic inflammation and health cohort study. Mediators Inflamm 2014, 412386 (2014).
Yuexin, Y., Y. W. China Food Composition. 2rd ed., 3–191 (Peking University Medical Press, 2009).
Kaiser, H. F. The varimax criterion for analytic rotation in factor analysis. Psychometrika 23, 187–200 (1956).
Chen, L. W. et al. Helicobacter pylori Infection Increases Insulin Resistance and Metabolic Syndrome in Residents Younger than 50 Years Old: A Community-Based Study. PLoS One 10, e0128671 (2015).
Alberti, K. G. et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 120, 1640–1645 (2009).
American Diabetes, A. Diagnosis and classification of diabetes mellitus. Diabetes Care 37 Suppl 1, S81–S90 (2014).
Craig, C. L. et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc 35, 1381–1395 (2003).
Acknowledgements
This study was supported by grants from the key technologies R&D program of Tianjin (Key Project: No. 11ZCGYSY05700, 12ZCZDSY20400, and 13ZCZDSY20200), the National Science and Technology Support Program (No. 2012BAI02B02), 2012 Chinese Nutrition Society (CNS) Nutrition Research Foundation—DSM Research Fund (No. 2014-071), the National Natural Science Foundation of China (No. 81372118, 81372467 and 81302422), the Technologies development program of Beichen District of Tianjin (No. bcws2013-21 and bc2014-05), the technologies project of Tianjin Binhai New Area (No. 2013-02-04 and 2013-02-06), the Science Foundation of Tianjin Medical University (No. 2010KY28 and 2013KYQ24), the Key Laboratory of Public Health Safety (Fudan University), Ministry of Education (No. GW2014-5), and the National Training Programs of Innovation and Entrepreneurship for Undergraduates (No. 201510062013), China. We gratefully acknowledge all of men and women who participated in the study and Tianjin Medical University General Hospital-Health Management Center for the opportunity to perform the study.
Author information
Authors and Affiliations
Contributions
Y.X. and K.N. contributed to the study conception and design; Y.X., G.M., Q.Z., L.L., H.W., H.S., X.B., Q.S., Y.G., L.F., F.Y. and H.Y. contributed to data collection, assembly, analysis and interpretation of the data; Y.X., B.Y., S.S., X.W., M.Z., Q.J., H.Z. and K.S. contributed to data collection; Y.X. and K.N. contributed to the manuscript drafting and approval of the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Xia, Y., Meng, G., Zhang, Q. et al. Dietary Patterns are Associated with Helicobacter Pylori Infection in Chinese Adults: A Cross-Sectional Study. Sci Rep 6, 32334 (2016). https://doi.org/10.1038/srep32334
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep32334
This article is cited by
-
Dietary habits and Helicobacter pylori infection: a cross sectional study at a Lebanese hospital
BMC Gastroenterology (2018)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
