
Abstract
The role of FEN1 genetic variants on gallstone and gallbladder cancer susceptibility is unknown. FEN1 SNPs were genotyped using the polymerase chain reaction-restriction fragment length polymorphism method in blood samples from 341 gallbladder cancer patients and 339 healthy controls. The distribution of FEN1-69G > A genotypes among controls (AA, 20.6%; GA, 47.2% and GG 32.2%) was significantly different from that among gallbladder cancer cases (AA, 11.1%; GA, 48.1% and GG, 40.8%), significantly increased association with gallbladder cancer was observed for subjects with both the FEN1-69G > A GA (OR = 1.73, 95% CI = 1.01–2.63) and the FEN1-69G > A GG (OR = 2.29, 95% CI = 1.31–3.9). The distribution of FEN1 -4150T genotypes among controls (TT, 21.8%;GT, 49.3% and GG 28.9%) was significantly different from that among gallbladder cancer cases (TT, 12.9%; GT, 48.4% and GG 38.7%), significantly increased association with gallbladder cancer was observed for subjects with both the FEN1-4150T GT(OR = 1.93, 95% CI = 1.04–2.91) and the FEN1-4150T GG(OR = 2.56, 95% CI = 1.37–5.39). A significant trend towards increased association with gallbladder cancer was observed with potentially higher-risk FEN1-69G > A genotypes (P < 0.001, χ2 trend test) and FEN14150G > T (P < 0.001, χ2 trend test) in gallstone presence but not in gallstone absence (P = 0.81, P = 0.89, respectively). In conclusion, this study revealed firstly that FEN1 polymorphisms and haplotypes are associated with gallbladder cancer risk.
Similar content being viewed by others

Introduction
Gallbladder cancer (GBC) is a relatively uncommon malignancy, but it has an unique geographical distribution in the world, with the highest incidence rate occurring in Chile, Poland, India, Japan and Israel and gallbladder cancer also occurs more common in certain ethnic population, such as Native American Indians and Hispanics1,2,3,4. In China, gallbladder cancer is relatively rare; however, its incidence has increased in the past several decades5,6. The pathogenesis of gallbladder cancer is not completely understood but a multifactorial etiology may be responsible for its development7,8. The risk factors for gallbladder cancer include female gender, obesity, chronic cholecystitis, cholelithiasis (gallstones) exposure to specific environmental chemicals (often occupational) and chronic bacterial infections of the gallbladder9,10. A recent study showed that single nucleotide polymorphisms (SNPs) of various genes are associated with gallbladder cancer risk11. As in other tissues, these risk factors contribute to the development of gallbladder cancer through multiple genetic alterations that activate oncogenes and silence tumor suppressor genes7. When carcinogens or other environmental factors alter DNA structure or modify DNA bases, DNA repair proteins repair the damage and maintain DNA integrity; however, alterations in the cell’s DNA repair proteins may reduce the cell’s ability to repair damaged DNA. The reduction or loss off a cell’s DNA damage repair capacity will lead to genetic alterations in that cell11. Four major DNA repair pathways have been identified to be responsible for repairing damaged DNA in cells. These pathways are the base excision, nucleotide excision (NER), double-strand break and mismatch repair pathways12. Research on DNA repair and the degree to which SNPs effect the function of important DNA repair genes could help identify genetic risk factors of gallbladder cancer development and help develop novel strategies for gallbladder cancer treatment.
To this end, we have studied the association of flap endonuclease 1 (FEN1; MIM 600393) SNPs with gallbladder cancer. FEN1 is multi-functional nuclease and is involved in DNA base-excision repair (BER) and DNA replication. FEN1 efficiently removes the 5′-flap during long-patch base-excision repair and processes Okazaki fragments during DNA replication13,14. Additionally, FEN1 promotes DNA fragmentation in apoptotic cells by acting as a 5′ exonuclease and a gap-dependent endonuclease15,16. Through these processes, FEN1 plays an essential role in the maintenance of genomic stability and protects against malignant transformation17. A previous study showed that yeast with functionally impaired FEN1 (RAD27 in yeast) had a remarkably increased rate of spontaneous mutation of genomic DNA18. In mice, haplo-insufficient FEN1 led to increased genome instability and carcinogenesis19 and FEN1 mutations in transgenic mice reduced nuclease activity and promoted cancer development in multiple organs20. Naturally occurring genetic variations in FEN1 expression or function may also contribute to cancer susceptibility21. FEN1 -69G > A (rs174538, in the FEN1 promoter region) and 4150G > T (rs4246215, in the FEN1 3′-untranslated region) SNPs are associated with elevated risks of breast cancer22, lung cancer23, hepatocellular carcinoma24, esophageal cancer25, gastric cancer26 and glioma27. Thus, we hypothesized that gallbladder cancer risk would be synergistically increased for the interaction of genetic variants with environmental factors (e.g. gallstones). We assessed the association of two functional FEN1 SNPs and their haplotypes with gallstone and gallbladder cancer risk in a Chinese population.
Material and Methods
Study subjects
We used blood samples from 341 gallbladder cancer patients and 339 healthy controls. This cohort was previously used to assess the association of xeroderma pigmentosum, complementation group C (XPC) Ala499Val (C > T) and Lys939Gln (A > C) polymorphisms with gallbladder cancer risk28. The cohort was composed of subjects who were residents of different geographic regions in China. Between January 2006 and December 2013, gallbladder cancer patients were recruited from four different hospitals (The First Affiliated Hospital of Sun Yat-Sen University, The First Affiliated Hospital of Xian Jiaotong University, The Second Affiliated Hospital of Guangzhou Medical University and the First Affiliated Hospital of Xian Medical College). Pathologists from the Pathology Department at the Sun Yat-Sen University School of Medicine histologically confirmed that all the cases in the cohort were gallbladder adenocarcinomas. We excluded patients with the following risk factors from this study: occupational exposure to ultraviolet radiation, occupational exposure to chemical carcinogens, chronic bacterial infections, carrier-state typhoid fever or ulcerative colitis. The control patients were recruited from the same four hospitals and were age and gender matched to the gallbladder cancer patients. Prior to inclusion in the study, the control patients were subjected to a routine health examination and were found to be free of cancer. Before participating our study, all subjects filled out a detailed questionnaire that included questions concerning patient demographics. Clinicopathological data from gallbladder cancer patients and healthy controls were also obtained. Since gallstones are an established gallbladder cancer risk factor (a risk that increases with increasing gallstone size)29,30, we recruited a panel of specialists to record the presence and size of gallstones using real-time ultrasound examination of all patients recruited for this study. Gallstones were identified based on the presence of movable hyperechoic foci casting acoustic shadows and measured using a PAV Electronic Sliding Caliper, Type Classic 6511. A pilot study was performed on 100 randomly selected healthy subjects who were not included in this study cohort. To assess inter-observer reliability, the Kappa value for gallstone diagnosis between specialists was 0.85 [95% confidence interval (CI): 0.74–0.95]. This study was approved by the Institution Review Board of the Ethics Committees of all participating institutes (The First Affiliated Hospital of Sun Yat-Sen University, Sun Yat-Sen University School of Medicine, Sun Yat-Sen University School of Pharmacy, The First Affiliated Hospital of Xian Jiaotong University, The Second Affiliated Hospital of Guangzhou Medical University, The First Affiliated Hospital of Xian Medical College, Shenzhen University School of Medicine, China. University Hospital Duisburg-Essen, Germany) and an informed consent form was obtained from each participant before the collection of blood samples and clinical evaluations. The methods were carried out in accordance with the approved guidelines.
Genotyping of FEN1 polymorphism
Genomic DNA was extracted from the peripheral blood of each participant. In brief, the buffy coat fraction from 4.9 ml venous blood in ethylenediaminetetraacetic acid was isolated and genomic DNA was extracted using a standard phenol-chloroform procedure31. FEN1 -69G/A (rs174538: G > A; NM_004111.4) and 4150G/T (rs4246215: G > T; NM_004111.4) SNPs were genotyped using a previously described polymerase chain reaction (PCR) restriction fragment length polymorphism assay23,31. PCR primers were designed based on the Genbank reference sequence: 5′-ggaggttccaggagcgtcta-3′ and 5′-ttctccaccgcttgtccc-3′ for FEN1-69G > A; 5′-tatgtcaggctcaaaccac-3′ and 5′-cagccagtaatcagtcacaa-3′ for FEN1 50G > T. PCR amplification was performed using a 25 μL reaction mixture containing 100 ng DNA, 0.1 mmol/L of each primer, 0.2 mmol/L deoxynucleoside triphosphate, 1.0 U rTaq DNA polymerase (TaKaRa, Dalian, Jinzhou, China), 1 x reaction buffer and 1.5 mmol/L MgCl2. PCR amplification consisted of an initial melting step of 2 min at 95 °C, followed by 35 cycles of 30 s at 94 °C, 30 s at 60 °C for FEN1 –69G/A and 55 °C for FEN1 4150G/T, 30 s at 72 °C and a final elongation step for 10 min at 72 °C. To distinguish the -69G/A or 4150G/T genotypes, PCR products were subjected to digestion with the restriction enzymes SalI (Sigma Genosys, St. Louis, MO, USA) or Alw26I (Sigma Genosys), respectively. For C.4150 G/T , the PCR product were digested with PvuII (New England Biolabs, Ipswich, MA, USA) overnight at 37 °C. The variant G allele had a PvuII restriction site and after digestion, 2 bands (147 and 112 bp) were generated, while the wild type T allele lacked this restriction site and a single band with a size of 259 bp were obtained. For C.-69G/A, the wild-type allele (A) produced 2 fragment of 112 and 35 bp and the polymorphic allele (G) produce a single 147 bp fragment. To avoid genotyping errors, two researchers independently repeated the genotyping of a limited number of random samples. Confirmation genotyping showed 100% agreement with the original results.
Statistical analyses
All the analyses were carried out using the Statistical Analysis System software (Version 9.0; SAS Institute, Cary, NC, USA). The PS: Power and Sample Size Calculation program (Vanderbilt School of Medicine, Nashville, TN, USA) were used to determine power and sample size computations according to the methods described in a previously published study32. Results of PS analysis indicated that both cancer and control populations were able to provide fair statistical power. In order to match cases and controls in terms of several putative confounding factors (e.g. age and gender), the chi-square and Student’s t-tests were used to assess the differences of several qualitative and quantitative traits. To evaluate deviation from the Hardy-Weinberg equilibrium, the discrepancies between observed and expected genotype frequencies in patients and controls were compared by using a chi-square test with one degree of freedom. Allelic association of the SNPs with disease traits was assessed using the Pearson’s 2 × 2 contingency table chi-square test. Gender typical risk of the SNPs for gallbladder cancer, in terms of odds ratio (OR) and 95% confidence interval (CI), was derived from logistic regression models with the SNP genotypes as the explainable variables. Finally, the effect of the FEN1 SNPs and gallstones on gallbladder cancer risk was analyzed using the logistic regression model. The two-locus genotypes, called diplotypes, were defined by the number of risk genotypes at -69G > A and 4150G > T loci. A p < 0.05 was considered statistically significant for point-wise statistical analysis. For multiple test analyses, the conservative Bonferroni method was used to correct the p value33.
Results
Characteristics of the study population
Prior to this study, we performed a statistical power analysis using the PS program33 to verify that the available cohort was of sufficient size to provide the statistical power necessary for our investigation. Using the population parameter set for effective sample size with an OR of 1.41 and allelic frequency of 0.29, the 341 gallbladder cancer cases and 339 age- and gender-matched healthy controls provided a statistical power of 71.29 and 80.93% at the nominal type I error rate of 0.05 and 0.025, respectively. These results were obtained after performing multiple tests of both SNPs.
Table 1 shows the distribution of age, gender, smoking status, drinking status and gallstone status among cases and controls. The patients and controls were adequately matched in terms of sex and age. The median age was 52.6 years (range, 37–79 years) for the cases and 52.3 years (range, 36–80 years) for the controls (P = 0.82). No significant difference was observed between patients and controls in sex distribution (31.7% males in patients vs.31.3% in controls; P = 0.99). However, smoking incidence, drinking incidence and gallstone incidence were significantly higher in cancer patients than in the control group (p < 0.001, P < 0.01, P < 0.001, respectively) and the OR for smoking-associated gallbladder cancer was 12.91 (95% CI, 9.86–26.42), the OR for drinking-associated gallbladder cancer was 9.23 (95% CI, 7.24–17.23) and the gallstone-associated gallbladder cancer was 17.25 (95% CI, 12.41–28.75), suggesting that smoking, drinking and gallstones are important predisposition factors for the development of gallbladder cancer. Of the 341 patients, 54 (15.8%) had pathology grade G1, 81 (23.8%) for grade G2, 162 (47.5) for grade G3 and 44 (12.9) for grade G4. In terms of TNM stage, 31 (9.1%) for 0 stage, 45 (13.2%) for I stage, 44 (12.9%) for II stage, 86 (25.2%) for III stage and 135 (39.6%) for stage IV. In terms of tumor differentiation, 47 (13.8%) patients were classified into the well, 123 (36.%) patients were classified into moderate, 144 (42.2%) patients were classified into poor and 27 (7.9%) were classified into undifferentiated. 202 (59.2%) patients had lymph node metastases, 108 (31.7%) patients had distant metastases and 146 patients (42.8%) its tumor size were smaller 2 cm (Table 1).
Association of FEN1 SNPs with gallbladder cancer risk
To determine whether the FEN1 allele contributed to increased association of gallbladder cancer, we examined the prevalence of FEN1 alleles in gallbladder cancer cases versus controls. The allelic frequencies of FEN1 -69A and -4150T were 0.378 and 0.373, respectively, among the 339 healthy controls and 0.301 and 0.296, respectively, among the 341 gallbladder cancer cases. The genotype frequencies in the control and patient groups conformed to Hardy-Weinberg equilibrium. Linkage disequilibrium analysis showed that FEN1 -69A and -4150T have strong correlation, with D′ = 0.95 and r2 = 0.96. The distribution of FEN1-69G > A genotypes among controls(AA, 20.6%; GA, 47.2% and GG 32.2%), the frequencies of the 3 genotypes among gallbladder cancer were AA,11.1%-; GA,48.1%- and GG, 40.8%. The GG genotypes were more prevalent in the cases than in the controls (P < 0.001). Significantly increased association with gallbladder cancer was observed for subjects with both the FEN1-69G > A GA (OR = 1.73, 95% CI = 1.02–2.63) and the FEN1-69G > A GG (OR = 2.29, 95% CI = 1.31–3.95) (Table 2). This association was not affected by adjusting other factors (age, sex and gallstone) via regression analysis (ORadjust = 1.74, 95% CI = 1.02–2.64 for the FEN1-69G > A GA genotypes; ORadjust = 2.31, 95% CI = 1.32–3.96 for the FEN1-69G > A GG genotypes). In the meantime, the distribution of FEN1 -4150T genotypes among controls(TT, 21.8%;GT, 49.3% and GG 28.9%), the frequencies of the 3 genotypes among gallbladder cancer were TT,12.9%-; GT, 48.4% and GG 38.7%. The GG genotypes was also more prevalent in the cases than in the controls (P < 0.001). Significantly increased association for gallbladder cancer was observed for subjects with both the FEN1-4150T GT(OR = 1.93, 95% CI = 1.04–2.91) and the FEN1-4150T GG(OR = 2.56, 95% CI = 1.37–5.39) (Table 2). These results was not affected by adjusting other factors (age, sex and gallstone) via regression analysis (ORadjust = 1.95, 95% CI = 1.09–2.94 for the FEN1-4150T GT genotype; ORadjust = 2.57, 95% CI = 1.39–5.42 for the FEN1-4150T GG genotype). These results where consistent with the fact that a significantly trend towards increased association was observed with predicted less protective FEN1 genotypes (P < 0.001, χ2 trend test, Table 2). Although stratification analyses by age, sex, smoking status or drinking status were also conducted, no further evidence was observed (data not shown). In this study, FEN1 -69GA and 4150GT SNPs were not associated with other clinicopathological parameters, such as age, sex, pathology grade , TNM stage , tumor differentiation , lymph node metastasis , size or metastasis of tumors (Table 3).
The relationship between FEN1 genotype gallbladder cancer association by exposure to gallstone
To determine the relationship between FEN1 genotype and gallbladder cancer by exposure to gallstone, we stratified study subjects by FEN1 genotype and gallstone status (Table 2). We observed no statistically significant association between FEN1 genotypes and gallbladder cancer in gallstone absence. In contrast, near-significant increases in risk for gallbladder cancer were observed for gallstone presence with the FEN1-69G > A GA (OR = 2.3, 95% CI = 1.5–3.5) and the FEN14150G > T GT (OR = 3.7, 95% CI = 1.4–9.8), whereas significant increases in association for gallbladder cancer were observed for gallstone presence with the FEN1-69G > A GG (OR = 6.8, 95% CI = 2.1–28.31) and the FEN14150G > T GG(OR = 7.2, 95% CI = 2.2–20.2). These data corresponded with the fact that a significant trend towards increased association for gallbladder cancer was observed with potentially higher-risk FEN1-69G > A genotypes (P < 0.001, χ2 trend test) and FEN14150G > T (P < 0.001, χ2 trend test) in gallstone presence but not in gallstone absence(P = 0.81, P = 0.89, respectively). A significant increase in risk for gallbladder cancer was observed for larger gallstone (those with stone diameters 2 cm or greater) with the FEN1-69G > A GA (OR = 2.1, 95% CI = 1.0–4.5) and the FEN14150G > T GT (OR = 2.3, 95% CI = 1.0–4.9), whereas significant increases in association for gallbladder cancer were also observed for larger gallstone (those with stone diameters 2 cm or greater) with the FEN1-69G > A GG (OR = 7.3, 95% CI = 1.8–18.8) and the FEN14150G > T GG (OR = 8.2, 95% CI = 1.5–19.8). These data are consistent with the observation that a significant increase trend risk for gallbladder cancer was obvious with potentially higher-risk FEN1-69G > A genotypes and FEN14150G > T genotypes in gallbladder cancer patients with larger gallstone(P < 0.001, P < 0.001, respectively, χ2 trend test). In the meantime, we observed a statistically significant association between FEN1genotype and gallbladder cancer risk in gallbladder cancer patients with smaller gallstone (those with stone diameters 2 cm smaller) (FEN1-69G > A GA:OR = 2.0, 95% = 0.7–3.9; FEN1-69G > A GG:OR = 3.5, 95% = 1.7–17.2; χ2 = 13.4, p < 0.001; FEN14150G > T GT:OR = 2.2, 95% = 0.8–4.3; FEN14150G > T GG:OR = 5.5, 95% = 1.3–16.7,χ2 = 13.7, P < 0.001).
Association of FEN1 haplotypes with gallbladder cancer risk
Haplotype analyses showed that the FEN1 A-69G4150, G-69G4150 and G-69T4150 haplotypes were associated with a significantly increased risk of gallbladder cancer. The adjusted ORs were 1.29 (95% CI = 1.11–1.52, p = 0.032); 2.14 (95% CI = 1.28–3.38, p = 0.023); 2.79 (95% = 1.94–3.99, P = 0.0009), respectively, when compared to the FEN1 A-69T4150 haplotype (Table 4).
Discussion
To the best of our knowledge, the current study is the first to assess the risk of gallbladder cancer associated with the FEN1 -69G > A and -4150G > T SNPs in a Chinese population. In this population, we found a significantly increased gallbladder cancer risk among carriers of the FEN1 -69G and 4150G alleles and the G-69G4150 haplotype compared with carriers of the -69A and 4150T alleles, the G-69T4150 T alleles or the G-69T4150 haplotype. Moreover, diplotypes and genotypic dosage was also associated with a significantly elevated risk when compared with the risk associated with individual loci. Our findings raised the possibility that the two loci may interact with gallstones to synergistically increase gallbladder cancer risk. Our data confirmed that FEN1 polymorphisms and haplotypes were associated with elevated gallbladder cancer risk and that gallstones synergistically increased this gallbladder cancer risk.
DNA repair enzyme maintenance of genomic integrity is an essential component of normal cell homeostasis and is necessary to maintain cell growth, differentiation and apoptosis34,35. Evidence increasingly indicates that polymorphisms in human DNA repair genes alter DNA repair capacity and are associated with increased solid tumor risk and susceptibility23,24. FEN1 is expressed in many species, from archaebacteria to humans and FEN1 functional deficiency may lead to genomic instability and cancer development18. One example illustrating the importance of the anti-cancer role of FEN1 was demonstrated using FEN1 knockout mice. While the homozygous FEN1 knockout was embryonically lethal, FEN1 heterozygous mice were viable and appeared to be healthy19. However, FEN1 heterozygous knockout mice that were also heterozygous for an APC gene mutation had increased cancer development and reduced survival36, indicating that FEN1 may function as a tumor suppressor gene14,37,38. Therefore, we predict that decreased FEN1 expression or altered FEN1 function could result in the malignant transformation of normal cells39 or increase the susceptibility of patients to other carcinogens or environmental factors17. Mechanistically, FEN1 mutations could induce single-stranded DNA breaks and the subsequent collapse of DNA replication forks, leading to DNA replication stress17. Polyploidy in cancer cells could lead to the overexpression of BRCA1, p19arf and other DNA repair genes in FEN1 mutant cells. This overexpression could trigger the single-stranded DNA break repair and non-homologous end-joining pathways, increasing DNA repair activity at the cost of frequent chromosomal translocations40. Our published28,29 and current data support the hypothesis that genetic variants that influence DNA repair capacity play an important role in human tumorigenesis.
No single causative factor has yet been identified for gallbladder cancer, but a number of predisposing and putative etiologies have been associated with altered DNA replication13,40. These include cholelithiasis, gallbladder polypoidal lesions, genetic predisposition, chemical carcinogens, anatomical variations of the pancreaticobiliary ductal system, infected bile, carrier-state typhoid fever and ulcerative colitis41,42,43. In this study, we found significantly increased gallbladder cancer risk among carriers of the FEN1 -69G and 4150G alleles and the G-69G4150 haplotype when compared with carriers of the -69A and 4150T alleles, the G-69T4150 T alleles or the G-69T4150 haplotype. These results are consistent with the findings, while other types indicate that of previous studies25,26,27, indicating that these genetic variants may be common cancer risk factors.
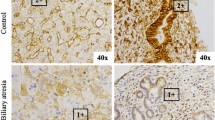
Gallstones are an established risk factor for gallbladder cancer44,45, the reported prevalence of gallstones in patients with gallbladder cancer ranges from 74% to 92% in European countries, whereas, in the U.S., gallstone prevalence is estimated to be 10% in the general population41. In China, a review of 3922 cases showed that the 49.7% of gallbladder cancer cases had concurrent gallstones43, while gallstone prevalence in the general Chinese population was estimated to be 7.2% (7,023/105,019). In previous clinical and population-based studies in China, inflammatory processes associated with gallstone and cholecystitis have been linked to the development of gallbladder cancer, gallstones are associated with an 18-fold risk of gallbladder cancer and the combination of gallstones and cholecystitis increases the risk of gallbladder cancer by 34-fold45. In this study, we found that 57.8% of gallbladder cancer patients had concurrent gallstones (197 of 341). This result was significantly higher than the percentage of cholelithiasis observed in the healthy control group (6.2%, 21 of 339). Additionally, physical trauma caused by gallstones or bile-containing carcinogens may synergistically induce epithelial dysplasia, encouraging the ultimate progression to carcinoma46,47. Our previous study demonstrated that cholelithiasis and cholecystitis produced a series of pathological epithelial changes, including simple epithelial hyperplasia, atypical hyperplasia and carcinoma in situ47. These pathological changes are all considered precancerous lesions of gallbladder carcinoma48,49. The current study demonstrated that the interaction of genetic factors and the environment, in this case the interaction of FEN1 polymorphisms and gallstones, could synergistically increase the risk of gallbladder cancer.
Potential Study Limitations
Our study has some limitations. First, since this study is a hospital-based case and control study, gallbladder cancer cases and controls from the hospital may have an inherent selection bias. Thus, a population-based prospective study is needed to validate our data. Second, only small number of the healthy controls in this study had gallstones. Therefore, the complicated genetic models of the FEN1 genotypes/diplotypes for gallbladder cancer could not be accurately matched with controls defined by the presence of gallstones or gallstones of varying size. Third, detection of both gene-gene and gene-environment interactions often requires a very large sample size; thus, the limited sample size of this study may not provide sufficient statistical power to explore these synergic effects. Significant interactions between FEN1 -69G > A (GA or GG) and 4150G > T (GT or GG) or between these genetic factors and cholelithiasis were identified. However, further investigation is needed in large and independent ethnic populations.
Additional Information
How to cite this article: Jiao, X. et al. Variants and haplotypes in Flap endonuclease 1 and risk of gallbladder cancer and gallstones : a population-based study in China. Sci. Rep. 5, 18160; doi: 10.1038/srep18160 (2015).
References
Pandey, M. Risk factors for gallbladder cancer: a reappraisal. Eur J Cancer Prev 12, 15–24 (2003).
Randi, G., Franceschi, S. & Vecchia, C. L. Gallbladder cancer worldwide: Geographical distributionand risk factors. Int J Cancer 118, 1591–1602 (2006).
Wood, R. et al. Epidemiology of gallbladder cancer and trends in cholecystectomy rates in Scotland, 1968–1998. Eur J Cancer 39, 2080–6 (2003).
Floreani, A. et al. Epidemiological aspects of biliary tree tumors in a region of northern Italy: emerging trends and sex-based differences. Eur J Gastroenterol Hepato 25, 1327–51 (2013).
Hsing, A. W. et al. Rising incidence of biliary tract cancers in Shanghai, China. Int J Cancer 18, 24–28 (1998).
Hsing, A. W. et al. Gallstones and the risk of biliary tract cancer: a population-based study in China. Br J Cancer 97, 1577–82 (2007).
Rustaqi, T. & Dasanu, C. A. Risk factors for gallbladder cancer and cholangiocarcinoma: similarities, differences and updates. J Gastrointest Cancer 43, 137–47 (2012).
Goeppert, B. et al. Prognostic impact of tumor-infilitrating immune cells on biliary tract cancer. Br J Cancer 109, 2665–74 (2013).
Robert, D. G. & Juan, C. R. Gallbladder cancer: a morphological and molecular update. Hispathology 55, 218–29 (2009).
Shukla, V. K. et al. Diagnostic value of serum CA 242, CA 19-9, CA 15-3 and CA125 in patients with carcinoma of the gallbladder. Trop Gastroenterol 27, 160–65 (2006).
Srivastava, K. et al. Candidate gene studies in gallbladder cancer: a systematic review and meta-analysis. Mutat Res 728, 67–79 (2011).
Pandey, S. N. et al. genetic polymorphisms in GSTM1, GSTT1, GSTP1, GTTM3 and the susceptibility to gallbladder cancer in North India. Biomarkers 11, 250–61 (2006).
Zheng, L. et al. Fen1 mutations that specifically disrupt its interaction with PCNA cause aneuploidy-associated cancer. Cell Res 21, 1052–67 (2011).
Zheng, L. et al. Fen1 mutations result in autoimmunity, chronic inflammation and cancers. Nat Med 13, 812–9 (2007).
Abdel-Fatah, T. M. et al. Genomic and protein expression analysis reveals flap endonuclease 1 (FEN1) as a key biomarker in breast and ovarian cancer. Mol Oncol 8, 1326–38 (2014).
Wang, K., Xie, C. & Chen, D. Flap endonuclease 1 is a promising candidate biomarker in gastric cancer and is involved in cell proliferation and apoptosis. Int J Mol Med 33, 1268–74 (2014).
Zhang, B. et al. Large-scale genetic study in East Asians identifies six new loci associated with colorectal cancer risk. Nat Genet 46, 533–42 (2014).
Wu, Z. et al. High risk of benzo[α]pyrene-induced lung cancer in E160D FEN1 mutant mice. Mutat Res 731, 85–91 (2012).
Xu, H. et al. Chemical-induced cancer incidence and underlying mechanisms in Fen1 mutant mice. Oncogene 30, 1072–81 (2011).
Kucherlapati, M. et al. Tumor progression in Apc(1638N) mice with Exo1 and Fen1 deficiencies. Oncogene 26, 6297–306 (2007).
Chung, L. et al. The FEN1 E359K germline mutation disrupts the FEN1-WRN interaction and FEN1 GEN activity, causing aneuploidy-associated cancers. Oncogene 34, 902–11 (2014).
Lv, Z. et al. Association of functional FEN1 genetic variants and haplotypes and breast cancer risk. Gene 538, 42–5 (2014).
Yang, M. et al. Functional FEN1 polymorphisms are associated with DNA damage levels and lung cancer risk. Hum Mutat 30, 1320–8 (2009).
Liu, L. et al. Functional FEN1 genetic variants contribute to risk of hepatocellular carcinoma, esophageal cancer, gastric cancer and colorectal cancer. Carcinogenesis 33, 119–23 (2013).
Chen, Y. et al. A NEIL1 single nucleotide polymorphism (rs4462560) predicts the risk of radiation-induced toxicities in esophageal cancer patients treated with definitive radiotherapy. Cancer 119, 4205–11 (2013).
Li,W. Q. et al. Genetic variants in DNA repair pathway genes and risk of esophageal squamous cell carcinoma and gastric adenocarcinoma in a Chinese population. Carcinogenesis 34, 1536–42 (2013).
Chen, Y. D. et al. Functional FEN1 genetic variants and haplotypes are associated with glioma risk. J Neurooncol 111, 145–51 (2013).
Jiao, X. et al. Ala499Val(C > T) and Lys939Gln (A > C) polymorphisms of the XPC gene: their correlation with the risk of primary gallbladder adenocarcinoma: a case-control study in China. Carcinogenesis 32, 496–501 (2011).
Jiao, X. Y. et al. hOGG1 Ser326Cys polymorphism and susceptibility to gallbladder cancer in a Chinese population. Int J Cancer 121, 510–5 (2007).
Moerman, C. J. et al. Gallstone size and the risk of gallbladder cancer. Scand J Gastroenterol 28, 482–6 (1993).
Mitra, A. K. et al. Association of polymorphisms in base excision repair genes with the risk of breast cancer: a case-control study in North Indian women. Oncol Res 17, 127–35 (2008).
Dupont, W. D. & J. Plummer, W.D. PS power and sample size program available for free on the Internet. Control Clin Trials 18, 274–275 (1997).
Bland, J. M. & J Altman, D. G. Multiple significance tests: the Bonferroni method. BMJ 310, 170 (1995).
Srivastava, S., et al. Single-nucleotide polymorphisms in the ABCG8 transporter gene is associated with gallbladder cancer susceptibility. Liver Int 29, 831–837 (2009).
Xu, H. L. et al. Variants in motilin, somatostatin and their receptor genes and risk of biliary tract cancers and stones in Shanghai, China. Meta Gene 2, 418–26 (2014).
Kucherlapati, M. et al. Haploinsufficiency of flap endonuclease (Fen1) leads to rapid tumor progression. Proc Natl Acad Sci. USA 99, 9925–29 (2002).
Singh, P. et al. Overexpression and hypomethylation of flap endonuclease 1 gene in breast and other cancers. Mol Cancer Res 6, 1710–7 (2008).
Abdel-Fatah, T. M., et al. Clinicopathological significance of human apurinic/apyrimidinic endonuclease 1 (APE1) expression in oestrogen-receptor-positive breast cancer. Breast Cancer Res Treat 143, 411–21 (2014).
Lam, J. S. et al. Flap endonuclease 1 is overexpressed in prostate cancer and is associated with a high Gleason score. BJU Int 98, 445–51 (2006).
Lazcano-Ponce, E. C. et al. Epidemiology and molecular pathology of gallbladder cancer. CA Cancer J ClinA 51, 349–364 (2001).
Henson, D. E. et al. Carcinomas of the pancreas, gallbladder, extrahepatic bile ducts and ampulla of vater share a field for carcinogenesis: a population-based study. Arch Pathol Lab Med 133, 67–71 (2009).
Park, S. K. et al. Polymorphisms of estrogen receptors and risk of biliary tract and gallstone: a population-based study in Shanghai, China. Carcinogenesis 31, 842–846 (2010).
Shi, J. S. et al. Studies on gallstones in China. World J Gastroeterol 7, 593–6 (2001).
Jiao, X. Y. et al. Genomic determination of CR1 CD35 density polymorphism on erythrocytes of patients with gallbladder carcinoma. World J Gastroenetrol 10, 3480–4 (2004).
Hsing, A. W. et al. Variants in inflammation genes and the risk of biliary tract cancers and stones: a population-based study in China. Cancer Res 68, 6442–6452 (2008).
Jain, K. et al. Sequential occurrence of preneoplastic lesions and accumulation of loss of heterozygosity in patients with gallbladder stones suggest causal association with gallbladder cancer. Ann Surg 260, 1073–80 (2014).
Jiao, X. Y. et al. Upregulated plasma and urinary levels of nucleosides as biological markers in the diagnosis of primary gallbladder cancer. J Sep Sci. 37, 3033–44 (2014).
Kirk, J. M., Martin, C. C. & James, G. F. Roles of infection, inflammation and the immune system in cholesterol gallstone formation. Gastroenterology 136, 425–440 (2009).
Ivan, R. et al. Preneoplastic lesions in gallbladder cancer. J Surg Oncology 93, 615–623 (2006).
Acknowledgements
This study was supported in part by the National Nature Science Foundation of China (#30840096 and #81071984) and Science Plan Foundation of Guangdong Province (#2013B3014). We would like to thank the medical staff of The First Affiliated Hospital, Sun Yat-Sen University, The First Affiliated Hospital, Xian Jiaotong University, The First Affiliated Hospital, Xian Medical College and The Second Affiliated Hospital, Guangzhou Medical University for their assistance in sample collection. We thank Medjaden Bioscience Limited for assisting in the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
Conceived and designed the experiments: X.J., D.L. and J.W. Performed the experiments: X.J., Y.W., L.Z., J.H.,C.Y., P.Z. and R.H. Contributed reagents/material/analysis tools: Y.W., C.L., J.D., J.F. and J.S. Wrote the main manuscript text: X.J., D.L., J.W. and Y.W. Reference collection and data management: P.Z., R.H. and R.H. Statistical analyses and paper writing: X.J., D.L., J.W. and Y.W. Study design: P.Z., R.H. and R.H. All authors reviewed the manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Jiao, X., Wu, Y., Zhou, L. et al. Variants and haplotypes in Flap endonuclease 1 and risk of gallbladder cancer and gallstones: a population-based study in China. Sci Rep 5, 18160 (2016). https://doi.org/10.1038/srep18160
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep18160
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
