
Abstract
Study design:
Retrospective, 1 year case series.
Objectives:
To analyze the relationship between gender, age, injury-related variables and rehabilitation outcomes in patients with spinal cord injury (SCI).
Setting:
Tertiary Rehabilitation Center, Inpatient rehabilitation unit, India.
Methods:
The data from a series of SCI cases were analyzed. Each case was followed from admission into the hospital until their discharge. Patients were described according to age, gender, etiology of SCI, neurological classification, medical complications, American spinal injury association (ASIA) classification, length of rehabilitation stay and spinal cord independence measure (SCIM).
Results:
Forty-seven new SCI cases, 37 (78.7%) male and 10 (21.3%) female patients, were reported over a 1-year period during 2009–2010. Male patients were younger than the female ones, but the difference was not statistically significant. There was no statistically significant relationship between age or gender, and the following SCI variables: ASIA classification, neurological classification, SCI complications and length of stay (P>0.05). Traumatic etiology and Pott’s disease was found be related with gender (P<0.05). There was no statistically significant relationship between age or gender and SCIM score at admission or discharge (P>0.05).
Conclusion:
Age and gender are not significantly related to outcomes of rehabilitation or characteristics of SCI in this sample. Further research is needed to confirm the generalizability of these findings and to identify which factors contribute more strongly to SCI rehabilitation outcomes.
Similar content being viewed by others

Introduction
Very little is known about the exact incidence of spinal cord injury (SCI) in India, as in most developing countries. The available, albeit limited, epidemiological research in this area indicates that ∼20 000 new cases of SCI occur every year.1 Sixty to seventy percent of these individuals are illiterate and belong to low socioeconomic status. Most sustain their injury by fall (that is, fall from unprotected roofs or trees, falls into uncovered wells) or road traffic accident, which represent primarily preventable traumatic causes.1 Although most of these traumatic spinal cord lesions occur in young patients, ∼20% of all spinal cord injuries occur in persons aged 65 years or older.2
It has been reported that older patients with SCI have different features with regard to etiology, ratio of male to female patients, neurological characteristics, complications, discharge placements and death after spinal cord lesions.3 Dave PK et al.4 concluded that older patients have a higher risk of mortality and complications, whereas Cifu et al.5 suggested that these patients obtain better outcomes as a result of the higher incidence of incomplete lesions in the elderly patients. However, others have found no relation between age and functional outcome.6, 7 Similarly, studies that explore gender issues in traumatic SCI have reported no gender differences in the rehabilitation length of stay (LOS), American Spinal Injury Association (ASIA) motor scores, disability or discharge to institutional care.7, 8
Given these conflicting findings, further epidemiological research is therefore needed to determine the incidence of SCI in developing countries, such as India, and the resultant demand on medical and social resources. Unlike other developing countries, there is no established national SCI registry in India. Similarly, there is no population-based data on SCI available in India. This information may help to formulate preventive measures that will modify or eliminate the risk factors and can decrease the incidence of this incapacitating injury. The purpose of this study was to therefore investigate the prevalence of SCI, and analyze the relationship between gender and age regarding a range of variables in patients with SCI during a 12-month period in 2009–2010.
Subjects and methods
The National Institute for the Orthopedically Handicapped (NIOH) is the apex institution under the Ministry of Social Justice and Empowerment, Government of India. It is a premier institution for rehabilitation in India, and serves the entire region and patients from other countries. The services provided at NIOH are rehabilitation and human resource development. A large number of SCI patients receive rehabilitation services at NIOH and return to their community as contributing citizens.
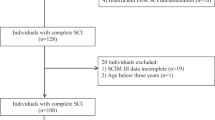
The present study involved a hospital-based retrospective review of all 47 patients with SCI that were admitted to the inpatient unit, NIOH, Kolkata, from April 2009 to March 2010. Each case is recorded only once (that is, on a patient’s initial admission) in the hospital's database. Age, gender, date of first admission, date of discharge, etiology, neurological classification, complications, ASIA classification, length of rehabilitation stay (LOS) and spinal cord independence measure (SCIM) was recorded for every patient.
Statistical analysis
Initial database entry was performed using Excel 2007 (Microsoft Corp, Redmond, WA, USA). Statistical analysis was done using SPSS 15.0 Software (SPSS Inc., Chicago, USA). Descriptive statistics, including proportions, means, medians and s.d.’s were calculated for age, gender, etiology, neurological classification, complications, ASIA classification, LOS for rehabilitation and SCIM. Spearman’s correlation coefficient test was used to assess the relationship between gender or age, and a range of injury-related variables. Wilcoxon Sign Rank test was used to examine the differences between age, SCIM at admission, SCIM at discharge and LOS between male and female patients. A statistically significant difference was defined as P<0.05.
Results
Patients characteristics
Forty-seven new SCI cases were reported during the study period including 37 (78.7%) male and 10 (21.3%) female patients. Male patients were younger (mean 34.81, s.d. 12.99 years) than female (mean 38.60, s.d. 9.93 years) ones, but the difference was not statistically significant (Wilcoxon Signed Ranks Test z=−0.764, P=0.445). Thirty-eight (80.9%) patients were paraplegic and nine (19.1%) patients were quadriplegic. The average LOS for rehabilitation was 93.34 (s.d. 40.95) days. Based on the ASIA Impairment Scale, the majority of patients were classified as ASIA A (36.2%, n=17) followed by ASIA B (25.5%, n=12), ASIA C (23.4%, n=11) and ASIA D (14.9%, n=7). None of the patients were classified as ASIA E.
Relationship between demographic and injury variables and rehabilitation outcome
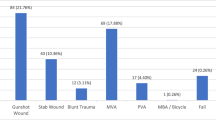
Trauma was most common cause of SCI (74.5%), followed by transverse myelitis (10.6%), myelopathy (4.3%), Pott’s disease (8.5%) and tumor (2.1%). The only etiology of SCI that was related to gender was trauma (male=66% versus female=8.5%, P=0.004) and Pott’s disease (male=2.1% versus female=6.4%, P=0.005). There was no correlation between gender and other causes of SCI. There was also no correlation between age and the etiology of SCI (P=0.267) (Table 1).
Pressure ulcer was the most common complication developed after SCI (34%), followed by urinary tract infection (19.1%), heterotropic ossification (2.1%) and respiratory tract infection (2.1%). There was no correlation between the occurrence of any of these SCI complications and the patient’s age (P=0.681) or gender (P=0.789) (Table 2).
There was no statistically significant relationship between age or gender, and SCIM score at admission or at discharge (P>0.05) (Table 3). Furthermore, there was no relationship between the age of patients and their LOS in rehabilitation (P=0.251) or their ASIA classification (Spearman’s ρ=0.158, P=0.288). There was also no relationship between the gender of patients and their LOS in rehabilitation (P=0.108) or their ASIA classification (Spearman’s ρ=0.226, P=0.127). Although there was a trend for male patients towards a shorter LOS (mean 88.10 days) compared with female patients (mean 112.70 days), this difference was not significant (P>0.05) (Table 3).
Discussion
SCI is a major cause of disability in India and the majority of new SCI cases are of traumatic origin. This retrospective review of SCI patients admitted to NIOH, Kolkata, over a 12-month period, highlighted that most patients are young and male. The prevalence of paraplegia was also greater than quadriplegia, whereas the most prevalent complication was pressure ulcer. Aside from a large incidence of traumatic SCIs among male patients, SCI rehabilitation outcomes were not significantly related to age or gender.
The SCI demographics identified in this study in relation to injury cause are distinct from that reported by the developed countries. For example, motor vehicle accidents are the leading causes of SCI in developed countries followed by falls.9 The reverse is true for most of the developing countries.1, 10 Sports and diving injuries are another important cause of traumatic SCI in the Western world,11 but this has rarely been reported from the developing countries. Among the non-traumatic SCIs, spinal tuberculosis is still an important cause in the developing countries of the world,12 whereas it is rarely seen in the developed countries nowadays. Another non traumatic cause of SCI in India, as evident in this study, is Pott’s disease.
This study also shares similarities with the available SCI research in relation to age of injury onset and gender. Indeed, the age distribution of patients in this study was comparable with studies from other parts of India and the world.1, 13 The mean age of male patients was 34.81 years and female patients was 38.60 years, signifying a higher incidence of SCI among younger, more active and more productive population of the country. This finding concurs with those of McKinley et al.14 in their 5-year prospective study. They reported that individuals with non-traumatic SCI were significantly males. The higher incidence of traumatic SCI in male patients, consistently found in the research, may be explained by examination of etiological factors, with men being exposed to more risk factors such as motor vehicle accident. Epidemiological studies of SCI have consistently shown a male predominance ranging from male to female ratio of 4:1 in the developed world15 to 13.5:1 in the developing countries.16 Results from the present study are no different, with the gender distribution showing a male to female ratio of 3.7:1, which is comparable to other recent studies.1, 4, 2 This statistic may reflect the changing face of social norms in India, with female individuals becoming a more active part of the workforce in India. This includes the main profession of agriculture, where female individuals are equal participants at work.
Our finding that gender was not related to ASIA classification at discharge from rehabilitation is consistent with previous studies of traumatic and non-traumatic SCI patients,4, 5 which have not found any significant influence of gender on ASIA motor scores. Similarly, the present study did not find an influence between gender and SCIM score at admission and discharge. This is consistent with previous SCI studies, which have shown that there is no influence of gender on disability after SCI measured using the Barthel Index.8, 16
Although previous research has reported that gender or age does not affect LOS, there was a trend for male patients in the present study to have a shorter LOS, by ∼25 days, compared with female patients.10, 17, 18, 19 However, the relationship between gender and LOS was not statistically significant. The finding that age did not influence LOS is also consistent with previous research, which has found that demographic variables are not predictors of LOS following traumatic SCI.5, 6, 20
The percentage of complications in our study was lower than that reported by other studies.21, 22 This may be due to the fact that the majority of patients in this study were paraplegic and not in the acute medical treatment phase of their SCI. The present study did not find any correlation between the occurrence of SCI complications and the patients’ age or gender’. This is similar to previous findings, with age not significantly related to complications such as urinary tract infection, pressure ulcer, spasticity, pneumonia, deep venous thrombosis or pulmonary embolism.7 In contrast, a previous study of traumatic SCI reported that older patients were more likely to develop complications like pneumonia, pulmonary embolism and renal calculi.20 Furthermore, a previous matched study in patients with traumatic and non-traumatic SCI reported no gender differences in relation to SCI complications, although the types of complications studied were not specified.22 However, other studies have reported some gender-related differences in the occurrence of SCI complications. One study of traumatic SCI reported that men were more likely to develop pressure ulcer and deep venous thrombosis.5 However, in the present study, none of the patients has developed deep venous thrombosis, pneumonia or pulmonary embolism during the study period.
The nonsignificant findings relating to the impact of age or gender on rehabilitation outcome may reflect the standardized measures used. In this study, the SCIM was adopted. In previous research, however, the functional independence measure (FIM) has been adopted, which has specific cognitive and psychosocial domains.23, 5 Both of these tools are reliable for measuring functional independence in SCI patients, as demonstrated by their high positive correlation coefficient (r=0.79, P<0.01). However, the SCIM is more responsive to changes than the FIM in the subscales of Respiration and sphincter management, and Mobility indoors and outdoors.24
There are some limitations of this study. As with all retrospective studies, inaccuracies due to incorrect or incomplete documentation may occur in the patients’ medical files and/or data transcription. We did not study the LOS in acute care before transfer to rehabilitation due to lack of information in the medical records. In addition, the number of participants in this study was relatively small, making a type-II error.
In many parts of the developing world, such as India, SCI remains a neglected and poorly managed condition. Furthermore, research on the incidence of SCI is sparse and, where available, data is missing. As demonstrated in this study, the demographics and epidemiological pattern of SCI share both similarities and differences from developed countries. Large-scale multicenter trials or population-based surveys are needed to assess the true magnitude of the problem in India and other developing countries. It is recommended to conduct studies on a large scale with longitudinal data, spanning 5–10 years, in order to describe the exact statistics of SCI in this region.
Conclusion
Retrospective studies, such as this study, provide statistical guidelines for the incidence of events or diseases for a specific area, region or country. Knowledge of the epidemiology of SCI in a given country is important not only for planning of resources, but also for adequate treatment and rehabilitation. Although this study may not be a true representation of epidemiology of all spinal injuries in society or in India, as it is restricted to one institution, it can be taken as a general trend, as we admit patients from a vast area of the country.
Data Archiving
There were no data to deposit.
References
Singh R, Sharma SC, Mittal R, Sharma A . Traumatic spinal cord injuries in Haryana: an epidemiological study. IJCM 2003; 28: 184–186.
Agrawal P, Upadhaya P, Raja KA . Demographic profile of traumatic and non-traumatic spinal injury cases: a hospital based study from India. Spinal Cord 2007; 45: 597–602.
Stover SL, Kartus PL, Rutt RD, Fine PR, Devivo MJ . Outcomes of the older patients with spinal cord injuries. Arch Phys Med Rehabil 1987; 68: 672.
Dave PK, Jayaswal A, Kotwal PP . Spinal cord injury- a clinico-epidemiological study. Ind J Orthop 1994; 28: 39–45.
Cifu DX, Huang ME, Kolakowsky-Hayner SA, Seel RT . Age, outcome, and rehabilitation costs after paraplegia caused by traumatic injury of the thoracic spinal cord, conus medullaris, and cauda equina. J Neurotrauma 1999; 16: 805–815.
Yarkony GM, Roth EJ, Heinemann AW, Lovell LL . Spinal cord injury rehabilitation outcome: the impact of age. J Clin Epidemiol 1988; 41: 173–177.
Greenwald BD, Seel RT, Cifu DX, Shah AN . Gender-related differences in acute rehabilitation lengths of stay, charges, and functional outcomes for a matched sample with spinal cord injury: a multicenter investigation. Arch Phys Med Rehabil 2001; 82: 1181–1187.
Scivoletto G, Morganti B . Sex-related differences of rehabilitation outcomes of spinal cord lesion patients. Clin Rehabil 2004; 18: 709–713.
Divanoglou A, Levi R . Incidence of traumatic spinal cord injury in Thessaloniki, Greece and Stockholm, Sweden: a prospective population-based study. Spinal Cord 2009; 47: 796–801.
Rathore FA, Farooq F, Muzammil S, New PW, Ahmad N, Haig AJ . Spinal cord injury management and rehabilitation: highlights and shortcomings from the 2005 earthquake in Pakistan. Arch Phys Med Rehabil 2008; 89: 579–585.
Boden BP, Jarvis CG . Spinal injuries in sports. Phys Med Rehabil Clin N Am 2009; 20: 55–68.
Turgut M . Spinal tuberculosis (Pott's disease): its clinical presentation, surgical management, and outcome. A survey study on 694 patients. Neurosurg Rev 2001; 24: 8–13.
Rahimi-Movaghar V, Saadat S, Rasouli MR, Ganji S, Ghahramani M, Zarei M et al Prevalence of spinal cord injury in Tehran, Iran. J Spinal Cord Med 2009; 32: 428–431.
Mckinley WO, Seel RT, Hardman JT . Non-traumatic spinal cord injury: incidence, epidemiology and functional outcome. Arch Phys Med Rehabil 1999; 80: 619–623.
Blering SE, Pederson V, Clausen S . Epidemiology of spinal cord lesions in Denmark. Paraplegia 1990; 28: 105–118.
Hoque MF, Grangeon C, Reed K . Spinal cord lesions in Bangladesh: an epidemiological study 1994-1995. Spinal Cord 1999; 37: 858–861.
McKinley WO, Tewksbury MA, Godbout CJ . Comparison of medical complications following nontraumatic and traumatic spinal cord injury. J Spinal Cord Med 2002; 25: 88–93.
Catz A, Goldin D, Fishel B, Ronen J, Bluvshtein V, Gelernter I . Recovery of neurologic function following nontraumatic spinal cord lesions in Israel. Spine 2004; 29: 2278–2282.
New PW, Epi MC . Influence of age and gender on rehabilitation outcomes in nontraumatic spinal cord injury. J Spinal Cord Med 2007; 30: 225–237.
Ronen J, Goldin D, Itzkovich M, Bluvshtein V, Gelernter I, Livshitz A et al Outcomes in patients admitted for rehabilitation with spinal cord or cauda equina lesions following degenerative spinal stenosis. Disabil Rehabil 2005; 27: 884–889.
DeVivo MJ, Kartus PL, Rutt RD, Stover SL, Fine PR . The influence of age at time of spinal cord injury on rehabilitation outcome. Arch Neurol 1990; 47: 687–691.
Nair KPS, Taly AB, Maheshwarappa BM, Kumar J, Murali T, Rao S . Nontraumatic spinal cord lesions: a prospective study of medical complications during in-patient rehabilitation. Spinal Cord 2005; 43: 558–564.
Furlan JC, Fehlings MG . The Impact of age on mortality, impairment, and disability among adults with acute traumatic spinal cord injury. J Neurotrauma 2009; 26: 1707–1717.
Itzkovich M, Gelernter I, Biering-Sorensen F, Weeks C, Laramee MT, Craven BC et al The Spinal Cord Independence Measure (SCIM) version III: reliability and validity in a multi-center international study. Disabil Rehabil 2007; 29: 1926–1933.
Acknowledgements
We acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. We are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Equebal, A., Anwer, S. & Kumar, R. The prevalence and impact of age and gender on rehabilitation outcomes in spinal cord injury in India: a retrospective pilot study. Spinal Cord 51, 409–412 (2013). https://doi.org/10.1038/sc.2013.5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2013.5
